
Abstract
Abstract
Background:
In the United States, breastfeeding initiation is reported for 75% of all live births; however, little information is available for mothers affected by severe preeclampsia (SP) who because of magnesium sulfate treatment are separated from their infants in the immediate postpartum period. This study examined feeding practices and factors associated with breastfeeding initiation in 281 women with SP and their 200 late-preterm and 81 term infants.
Subjects and Methods:
SP was diagnosed according to established clinical and laboratory criteria. Infant feeding preference was ascertained on admission to labor and delivery. Variables known to influence breastfeeding initiation, including maternal age, smoking, obesity, and racial and educational characteristics, were assessed.
Results:
All mothers received magnesium sulfate for 24 hours following delivery. Of 281 infants, 54% were admitted to the neonatal intensive care unit (NICU). All mothers and infants survived. On admission, 149 women intended to breastfeed, 73 intended to feed formula, and 59 were undecided. Four of 73 women who did not wish to breastfeed and 27 of 59 originally undecided later initiated breastfeeding. At discharge, 144 (51%) of all these mothers had successfully initiated breastfeeding. Factors associated with breastfeeding initiation failure included African American race, younger age, lower education, multiparity, smoking, and obesity. Of 149 women who intended to breastfeed, 76% were successful, and logistic regression analysis showed that intention to breastfeed was the most significant predictor of breastfeeding initiation. During the first 24 hours postpartum, 78% of infants receiving well-baby care, and 4% of those admitted to the NICU visited with their mother once. Among women who intended to breastfeed, successful breastfeeding initiation involved 85% of infants receiving routine well-baby care and 69% of those admitted to the NICU.
Conclusions:
In spite of the challenges created by SP, including early maternal separation, breastfeeding initiation is possible. The strongest predictor for breastfeeding success remains the intention to breastfeed, whereas race, lower level of education, and obesity are associated with breastfeeding initiation failure.
Background
The present study examined clinical and demographic factors including early maternal separation associated with breastfeeding initiation in women with SP who delivered late-preterm and term infants.
Subjects and Methods
This was a retrospective cohort investigation (2007–2010) approved by the Institutional Review Board of Wexner Medical Center, The Ohio State University, Columbus, OH. SP was diagnosed according to clinical and laboratory criteria. 14 Women with chronic hypertension and superimposed preeclampsia were included. Obesity was defined by a body mass index of 29–34 kg/m2 and morbid obesity by a body mass index of ≥35 kg/m2. 15 The study population consisted of pregnant women with SP and their live-born infants if delivered at ≥34 weeks, a point in gestation in which most infants are able to nipple feed. In cases of twin gestation, only the first born was reported. On arrival to labor and delivery, women's feeding preference for their infants (breastfeeding, formula feeding, or undecided) was ascertained.
According to our institutional standard of care, women with SP are given intravenous magnesium sulfate prior to and for 24 hours following delivery for prevention and/or treatment of convulsions. 16 Depending on the condition of the mother and their infant at delivery, mother–infant interaction (holding, skin-to-skin contact, or breastfeeding) and postpartum visitation was encouraged. After delivery, stable infants were transferred to the well-baby nursery (WBN) for routine management, whereas those who required specialized care were transferred to the newborn intensive care unit (NICU). All mothers remained in the labor and delivery suite for 24 hours following delivery. Infants admitted to the NICU were seldom stable enough to visit. Because of the clinical effects of SP and of magnesium sulfate treatment, which included headaches, nausea, and altered sensorium, visitations were brief, and interaction was limited. Thus, for the majority of infants, extended interaction with their mothers was postponed until discontinuation of the magnesium sulfate treatment. Lactation consultants assisted all mothers who intended to breastfeed or who were undecided about their infant feeding preference. At the time of discharge from the hospital all mothers were provided with telephone access to a breastfeeding helpline available around the clock. Hard copies and electronic neonatal records were reviewed, and type, frequency, and amount of each feeding were recorded. Considering that women who only breastfeed one or two times per day are likely to stop breastfeeding soon after delivery, 17 we defined breastfeeding initiation as successful if at the time of discharge from the hospital ≥50% of the feedings were direct from the breast or by expressed breastmilk. Excessive weight loss (EWL) was characterized by a ≥10 % decrease in weight from birth. 18 Acknowledging that maternal separation as well as concerns regarding the well-being of their babies could influence the intention to breastfeed, a comparison was made between stable infants admitted to the WBN and those infants admitted to the NICU. Because of the study design, there was no follow-up information on feeding practices beyond hospital discharge.
Statistical analysis
Comparison between the groups and subgroups were made with Student's t test for continuous and χ2 or Fisher's exact test for categorical variables. Depending on normality, continuous data were compared using one-way analysis of variance or nonparametric Kruskal–Wallis test. Multivariate analyses were conducted to further determine the effect of the intention to breastfeed and other variables on breastfeeding initiation. Demographic and clinical confounding variables were considered, and those with univariate association were entered as a block into a logistic regression equation.
Results
Our study population consisted of 281 women and their infants; 62% were white, 27% African American, 6% Hispanic, and 5% African or Asian. Their educational level was ≤11th grade (15%), high school (62%), and college or postgraduate (23%) (Table 1). Two hundred seventy-seven of the women had SP, while four had chronic hypertension with superimposed preeclampsia. Other co-morbidities included 35 patients with pregestational and 27 with gestational diabetes mellitus. Thirty-five percent of the mothers were obese, and 15% were morbidly obese. The majority of the pregnancies involved singletons. Twenty-three of the 24 twin pregnancies were dichorionic diamniotic, whereas one was a monochorionic diamniotic gestation. There were 140 cesarean deliveries, 40 of which were repeat. The most common indications for primary cesarean delivery included worsening maternal condition, failure of labor to progress, breech presentation, and HELLP syndrome. 4 All mothers and their infants, including twins, survived.
p<0.01.
BMI, body mass index.
Intention to breastfeed
On arrival to labor and delivery, 149 of 281 (53%) women intended to breastfeed, 73 (26%) intended to feed formula, while the remaining 59 (21%) were undecided (Table 1). All three groups of women were similar in the number of twin pregnancies, gestational age, and the incidence of gestational and pregestational diabetes mellitus. Women who intended to breastfeed were slightly older, white, primiparous, and more educated (attended college or postgraduate school). Conversely, African American race, obesity, smoking, and multiparity characterized women who intended not to breastfeed. Women with undecided feeding preferences were similar to those who intended not to breastfeed but included three times more Hispanic and African or Asian women (13 of 59 compared with four of 73, respectively). Intention to breastfeed was similar between women who delivered late-preterm and those delivering at term (52% and 54%, respectively).
Breastfeeding initiation
Demographic and clinical correlates with successful breastfeeding initiation are presented in Table 2. Of 281 mothers, 144 (51%) successfully initiated breastfeeding. The strongest predictor of breastfeeding initiation was the intention to breastfeed (p<0.0001; odds ratio [OR] 18.6; 95% confidence interval [CI] 9.45, 36.69), followed by higher education (p<0.0001; OR 5.88; 95% CI 1.58, 21.78). Conversely, women who did not breastfeed were more likely to be African American (p<0.0002; OR 0.39; 95% CI 0.19, 0.61), smokers (p<0.0001; OR 0.19; 95% CI 0.09, 0.40), or obese (p<0.01; OR 0.9; 95% CI 0.93, 0.99). Fifty-seven percent of white and 29% of African American women in our study successfully initiated breastfeeding.
p<0.01.
BMI, body mass index, CI, confidence interval; NICU, neonatal intensive care unit; NS, not significant; OR, odds ratio.
Nearly half (46%) of undecided women but only 5% of women who intended to feed their infants formula successfully initiated breastfeeding. Both groups of women were similar in demographic and clinical characteristics except those who still opted to feed formula were more likely African American (p<0.02; OR 0.229; 95% CI 0.06, 0.87).
Breastfeeding initiation was similar between 200 late-preterm infants and 81 term infants (51% and 52%, respectively). At discharge, well babies were younger in chronological age than NICU infants (4±1 days vs. 12±9 days, respectively) but were similar in postconceptional age. Discharge weights of the 137 formula-fed and 144 breastfed infants were similar, and EWL for infants discharged at ≤5 days was noted in 3% of 83 breastfed infants but not among 76 formula-fed infants. For infants discharged at ≥6 days, EWL was noted in 2% of 61 breastfed infants and in 3% of 61 formula-fed infants. Most infants in both groups discharged at or before 10 days had not regained birth weight (53% and 67%, respectively). Conversely, most infants discharged after 10 days had regained or exceeded birth weight (90% and 95%, respectively) (Fig. 1).
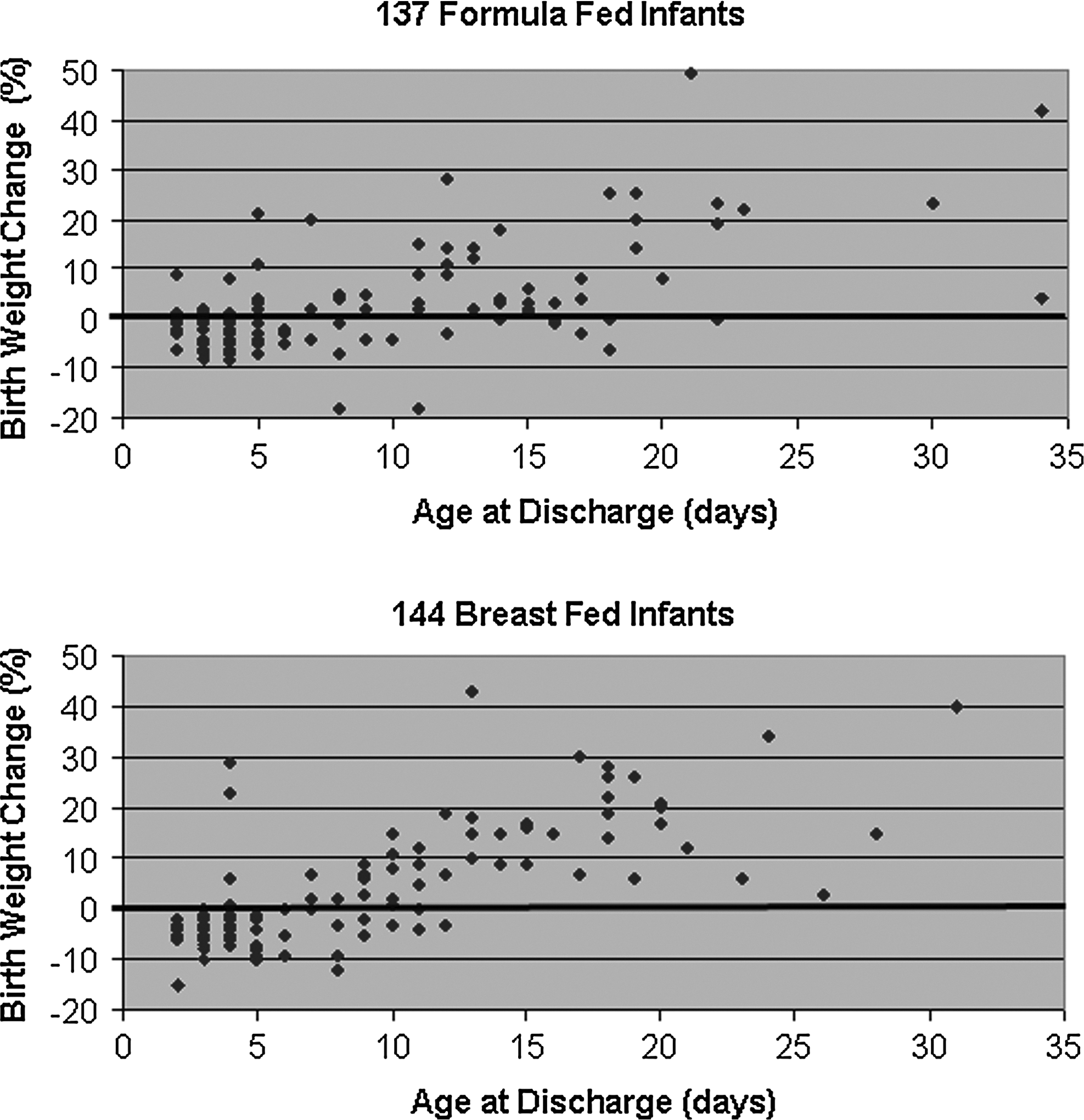
Weight change from birth to the time of discharge from the hospital:
WBN admissions
Two hundred of the 281 women (71%) delivered between 34 and 36 weeks gestational age. One hundred twenty-nine (46%) of the 281 infants were admitted to the WBN. This included 87 late-preterm and 42 term infants whose median length of hospital stay was 3 days (range, 2–6 days). During the first 24 hours postpartum, 100 of the 129 (78%) infants briefly visited their mothers. For the remaining 29 infants the first encounter occurred after 24 hours when their mothers were discharged from labor and delivery. Thirty-seven infants were breastfed at least once during the first day (11 of them continued breastfeeding exclusively, while the remaining 26 received formula intermittently). Twenty-three infants had their first breastfeeding during the second day and 10 during the third day or later. At the time of discharge from the hospital 42 (33%) infants were exclusively breastfed, 28 (22%) were breastfed with formula supplements, and the remaining 59 (45%) were taking formula exclusively.
NICU admissions
One hundred fifty-two (54%) of the 281 infants were admitted to the NICU. The most common admission diagnoses were prematurity (91%), respiratory distress (47%), prevention or treatment of hypoglycemia (28%), and miscellaneous. Twenty-two formula-fed and 32 breastfed infants required gavage feeding for a median duration of 5 days (range, 1–14 days). Most NICU patients had an uneventful hospital stay except for 20 infants who were noted to have visible blood in the stools between Days 2 and 12 of life. Sixteen of these patients were diagnosed with pneumatosis coli, two developed classic (medical) necrotizing enterocolitis, and the two remaining infants were diagnosed with benign isolated rectal bleeding. 19 Prior to the recognition of visible blood in the stools, seven of the 20 infants were breastfed, whereas 13 were taking formula. After a fasting period that ranged from 5 to 12 days, nine patients were discharged on breastfeeding, eight were taking Alimentum®, and the remaining three patients were taking Neosure® (both from Abbott Laboratories, Columbus, OH).
All infants admitted to the NICU (half of them born by cesarean section) were shown briefly to their mothers at the time of delivery. During the following 24 hours, only six infants had short visits with their mothers. For the remaining 146 infants the first encounter occurred after 24 hours, when their mothers were discharged from labor and delivery. Six infants received expressed breastmilk during the first day, 24 during the second day, and 44 during the third day or later. At the time of discharge from the hospital 39 (26%) infants were exclusively breastfed, 35 (23%) were breastfed with formula supplements, and the remaining 78 (51%) were taking formula exclusively.
Intention to breastfeed and breastfeeding initiation
Neonatal outcomes for WBN and NICU infants born to 149 mothers with SP who intended to breastfeed are shown in Table 3. Most demographic and clinical factors of these groups were similar, except for cesarean deliveries, late preterm infants, birth weight, need for gavage feeding, visitation with their mothers during the first postpartum day, length of hospital stay, and rate of breastfeeding initiation.
BMI, body mass index; NICU, neonatal intensive care unit; WBN, well-baby nursery.
Discussion
In 2000 the rate of breastfeeding initiation (70.9%) and breastfeeding continuation at 6 months (34.2%) in the United States among mothers discharged from U.S. hospitals was dismal. 20 The Goals for Healthy People 2010 included breastfeeding initiation for 75% of all newborns and continued breastfeeding for at least 50% of them at 6 months of age. 21 Multiple causative factors including hospital practices were identified, and efforts were made to correct them. 22 During the subsequent 10 years breastfeeding initiation rates for infants discharged from U.S. hospitals or birth centers increased from 70.9% to 75%, but breastfeeding continuation rates at 6 and 12 months (44.3% and 23.8%, respectively) remain lower than the Healthy People Objectives for the year 2020. 3 At the same time, remarkable progress was made in the use of human milk (own mother as well as donor) in very low birth weight babies.13,23 Although all these developments suggest a national, cultural and behavioral change, data pertaining to special populations such as that of women with SP remain elusive. Moreover, these reports are based on self-administered questionnaires completed months after birth.5–7
One of the unique issues pertinent to mothers with SP is the medications used for its treatment. 16 Antihypertensive drugs, although all capable of crossing the placenta, have not been reported to significantly impact lactogenesis when used cautiously. 24 The mainstay of treatment of SP in the United States remains intravenously administered magnesium sulfate. 16 Although it is well recognized that this medication readily crosses the placenta and may affect stage II lactogenesis, 25 clinical data suggest minimal or at least transient effects. 26
It has been reported that some infants whose mothers received magnesium sulfate may experience transient hypotonia and delayed feeding behavior. 27 Our data suggest that these effects if present are temporary and probably minimal at least for the more mature infants. After all, 129 infants (87% of them late-preterm) admitted to the WBN were discharged home during the first week of life. Data from infants admitted to the NICU suggest that the need for gavage feedings described above seemed related more to gestational age than to a pharmacological effect of magnesium sulfate.
Data pertaining to the intention to breastfeed are relevant because of its strong correlation with breastfeeding initiation and breastfeeding continuation at 2, 3, and 6 months.28–33 In Ohio, a retrospective survey showed that 53% of mothers intended to breastfeed, 16% were undecided, and 30% were not interested. 10 Recently, a study of 883 lower-income, ethnically diverse women who delivered healthy term infants showed that 45.9% intended breastfeed, 46.1% anticipated mixed feedings, and 8% wanted to feed formula. 31
It is estimated that intention to breastfeed is declared before pregnancy in 40%, during pregnancy in 30%, and after delivery for 30% of mothers. 23 It is also known that intention to breastfeed declared before pregnancy has a stronger predictive value for breastfeeding initiation than when declared later. 23 Because of our study design we were unable to ascertain how far in advance their intention to breastfeed was made.
According to the theory of planned behavior, demographic characteristics (such as age, education, marital status) may influence beliefs and attitudes toward infant feeding, which in turn affect breastfeeding intention, breastfeeding initiation, and finally breastfeeding duration. 34 The central premise of the theory is that the immediate antecedent of a behavior is the person's intention to perform it. 35 Intention in turn is a function of the attitude toward the act (i.e., positive or negative feelings toward the behavior of interest), the subjective norm that reflects social references (i.e., what others think about the behavior), and perceived behavioral control (i.e., do I know how to do it, do I have the available resources). 30 Our data, similar to those of others, showed that women who intend to breastfeed are somewhat older, mostly primiparous, highly educated, and white,28–31 whereas those who intended not to breastfeed were African American, obese, and smoked and had a lower level of education.12,32,36 Maternal knowledge about infant health benefits and comfort with breastfeeding in social settings are factors also related to the intention to exclusively breastfeed.12,31
In our investigation of 149 women with SP who intended to breastfeed, 76% successfully initiated breastfeeding. This is in contrast with data from a large population study based on self-administered questionnaires that included 364 women with preeclampsia from Switzerland and Germany. 5 Those investigators reported that of the 76.1% of women who intended to breastfeed, only 39.2% initiated breastfeeding compared with their healthy controls (86.8% intended to breastfeed, 48.9% initiated breastfeeding). 5 The main difference between the two studies is their inclusion of 103 infants who delivered before 32 weeks, whereas we studied only late-preterm (34–36 weeks gestational age) and term infants.
In our study the breastfeeding initiation rate for all infants regardless of maternal feeding preference admitted to the NICU was similar to that of stable infants who received traditional routine well-baby care (49% and 54%, respectively).
Infants' hospitalization,10,28 prematurity,5,13 cesarean delivery,5,9 and delayed maternal–infant interaction36–40 are factors known to deter breastfeeding. Our data showed that these factors indeed played a role, albeit not absolute, in the breastfeeding initiation rates among mothers who intended to breastfeed but did not succeed (Table 3).
The strength of the maternal commitment to lactation is demonstrated by the fact that breastfeeding initiation was successful even in mothers who did not breastfeed up to the third and fourth postpartum day and for those 32 mothers who provided expressed breastmilk for their gavage-fed infants.
The short- and long-term benefits of early prolonged mother–infant interaction have been widely reported.37–40 Extended skin-to-skin contact early in life (even if delayed until after the first week) between low birth weight infants and their mothers' increases oxytocin release and facilitates breastfeeding. 37 Even a 5–10-minute visit within the first 3 hours of life (sensitive period) helps to form the basis for a more secure attachment of the premature infant to his or her mothers. 40 However, the rate of breastfeeding between those who visited and those who did not visit were similar. 40 Recent studies also recognized the presence of an early sensitive period during which close contact of mothers with their term infants resulted in long-term benefits on mother–infant interactions but did not influence the duration of breastfeeding. 39 These findings are in contrast with that of a meta-analysis of 30 studies involving 1,925 mother and healthy full-term infant dyads that found significant benefits of skin-to-skin contact on the rate of breastfeeding at 1 and 4 months after birth. 37 Unfortunately, neither of these studies involved mothers with SP for whom even a short infant visitation during the first 24 hours could be a positive factor on breastfeeding initiation. More important is that the absence of skin-to-skin contact during the sensitive period did not deter breastfeeding initiation among mothers who intended to breastfeed but who because of their SP were separated from their babies for a prolonged time.
The majority of late-preterm and term infants regardless of feeding practice experience a 7–10% weight loss during the first 7–10 days of life. 41 Most investigators agree that a ≥10% change represents EWL and should prompt some intervention to prevent medical complications. 42 Delayed onset of lactation and suboptimal infant feeding behavior may lead to EWL with and without dehydration. 9 A recent study reports an alarming rate of EWL at 3 days of age among term infants exclusively breastfed (18%) or those who were breastfed but also received a minimal formula supplement (16%). 17 A similar rate (18%) of EWL was reported earlier among exclusively or partially breastfed near-term infants. 42 Poor intake, delayed lactogenesis, and an excessive maternal fluid administration could be potential causative factors.17,43 Our data showed that EWL was a rare occurrence at 5 and 10 days of age among breastfed or formula-fed infants. One plausible explanation is that because of maternal separation, 270 of the 281 infants received supplementation of formula during the first 24 hours of life, a factor that could prevent a high rate of EWL. 17 It is also possible that the fluid restriction, which is standard in the management of SP patients, has effectively minimized maternal fluid imbalance indirectly preventing EWL. 16
Limitations of our investigation are those inherent to retrospective designs and the lack of follow-up regarding breastfeeding after discharge. Our study of mothers with SP demonstrates that despite early maternal separation and medical therapy successful breastfeeding initiation is possible. The significant number of mothers who on arrival to labor and delivery were undecided about infant feeding preference and who later successfully initiated breastfeeding highlights an opportunity for intrapartum and postpartum education.
Footnotes
Disclosure Statement
No competing financial interests exist.