
Abstract
Abstract
Despite the known health benefits for mother and infant, compliance with exclusive breastfeeding continues to challenge many healthcare providers. In an ongoing attempt to maintain the goals of the Healthy People 2010 initiative, our institution set out to identify patients with suboptimal breastfeeding rates in order to recognize potential barriers. Review of breastfeeding rates at the time of discharge noted significantly lower participation by clinic patients. In order to develop successful interventions, the aim of this study was to survey clinic patients to determine their intentions, attitudes, and obstacles to the practice of exclusive breastfeeding. In total, 188 surveys were completed during a 2-month time period. Respondents were primarily Hispanic (76.4% vs. 9.6% black and 8.4% white) and multiparous (57.5%) with a mean age of 25.7 years (range, 15–39 years old). Although 95.3% of respondents indicated that they believed breastmilk provided adequate nutrition, only 35.3% planned on exclusively breastfeeding. Access to free formula through the Special Supplemental Nutrition Program for Women, Infants and Children was the most common reason not to breastfeed (48.3%), followed by fear of pain and the need to return to work/school. Patients reported that the person with the greatest influence on their decision to breastfeed was their partner/spouse. Access to a lactation counselor was the most popular intervention requested, even among experienced multiparous patients (78.9% of whom had previously breastfed). In conclusion, the survey indicated that planned exclusive breastfeeding rates are low among this inner-city resident clinic and interventions should include involvement of the partners/spouses and access to lactational support.
Introduction
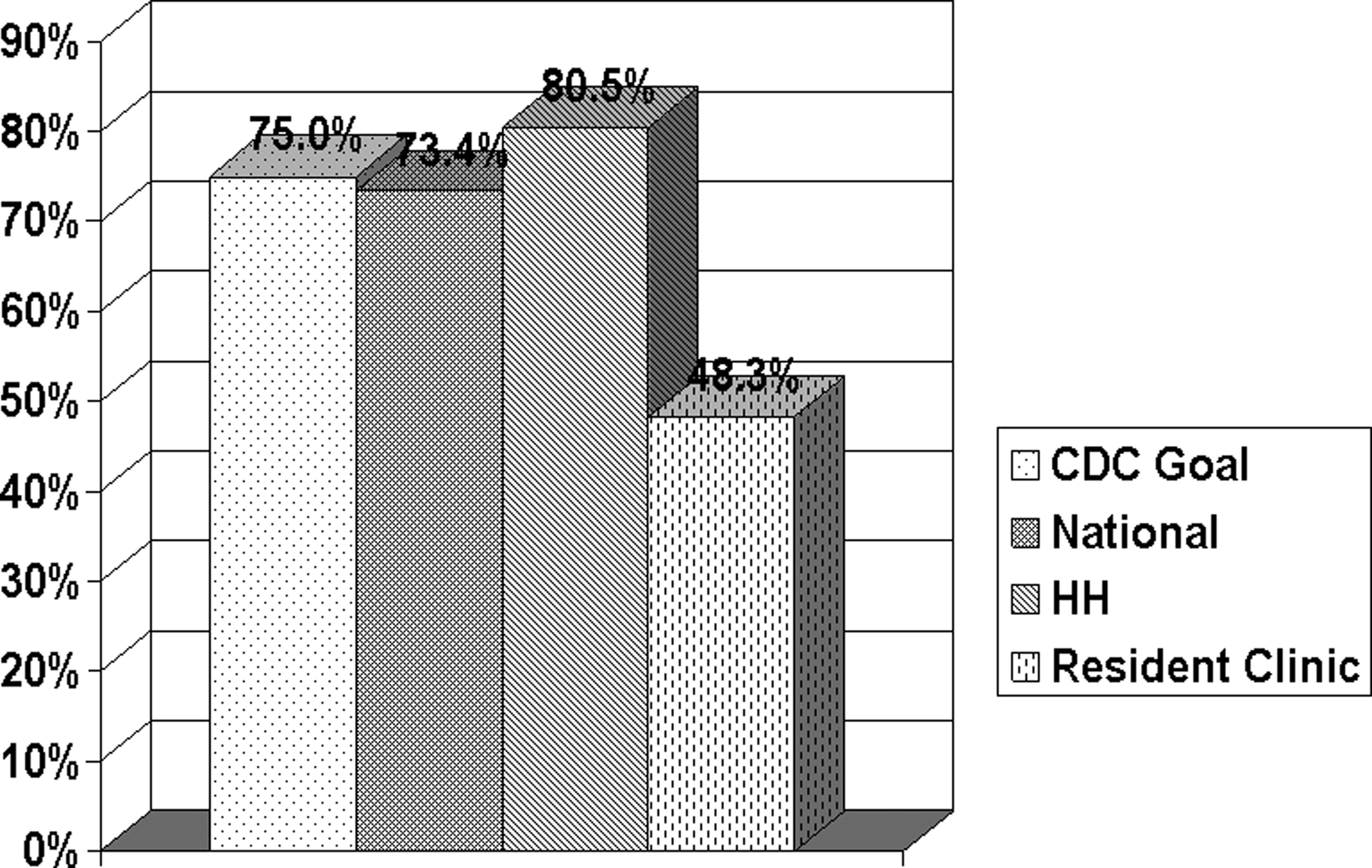
The Joint Commission 12 recently introduced exclusive breastfeeding (feeding only breastmilk) as a care practice for hospitals nationally. Consequently, hospitals are expected to measure and report their rates for exclusive breastfeeding. In a 2011 institutional analysis at Hartford Hospital (Hartford, CT), 80.5% of all postnatal women were breastfeeding at the time of discharge; however, patients of the resident clinic showed significantly lower rates, with only 48.3% breastfeeding at discharge and only 15.2% breastfeeding exclusively. Hospital and clinic rates of breastfeeding are compared with national rates and the Centers for Disease Control and Prevention's goals in Figure 1. Hartford Hospital's resident clinic serves a large inner-city Hispanic population. Providers at the clinic note that their patients trend toward formula feeding or supplementing breastfeeding with infant formula. Many of these patients are enrolled in the WIC program, which provides women, infants, and children with supplemental food packages that often include infant formula.
The goal of this study was to survey resident clinic obstetrical patients to determine their knowledge of the benefits of breastfeeding and to identify barriers that patients encounter to the beneficial practice of exclusive breastfeeding. The aim was to then use the survey results to design targeted educational practices to improve exclusive breastfeeding rates.
Subjects and Methods
An anonymous survey was developed by the authors and included input from physicians, a certified nurse midwife, and a lactation specialist. The study was approved by the Hartford Hospital Institutional Review Board. Obstetrical patients receiving care at the resident clinic were asked to complete the survey at the time of a visit. The survey was offered in both English and Spanish and was expected to take only 5 minutes to complete. Inclusion criteria were any pregnant women receiving prenatal care at the clinic. Exclusion criteria were those patients who were not pregnant, patients who were non–English- or non–Spanish-speaking, and those that had already completed the survey. The survey included questions concerning demographics, WIC enrollment, prior pregnancy history, and whether or not patients planned to breastfeed after delivery. Additionally, it surveyed women's knowledge of the benefits of breastmilk, potential influences on their decision to breastfeed, and reasoning behind plans for supplementation with formula. Finally, women were queried about their interest in potential educational or support services that could be offered by the clinic.
The data were collected over a 2-month time period. The surveys contained no patient identifiers and were stored in a secure location. The results were analyzed using SPSS software. Frequency distributions were used to assess patterns of breastfeeding behaviors, knowledge, and attitudes. The χ2 test was used to draw comparisons according to race and other demographic characteristics. A probability value of 0.05 was used to indicate statistical significance for all tests.
Results
In total, 188 surveys were completed over a 2-month time period (June–July 2011). The respondents were primarily Hispanic (76.4% vs. 9.6% black and 8.4% white) and multiparous (57.5% vs. 41.4% primiparous). The mean age was 25.7 years old, with a range of 15–39 years. In total, 88.4% of the respondents were enrolled in WIC. When asked about breastfeeding, the majority of patients (81.4%) were planning on breastfeeding. Of those patients planning to breastfeed, 66.7% had done so previously, while 33.3% had not. Only 35.3% of patients surveyed planned to breastfeed exclusively. When queried about long-term feeding plans, 58.3% of patients who planned to breastfeed were expecting to breastfeed for more than 6 months. Almost all (95.3%) of the respondents indicated that they believed breastmilk provided adequate nutrition.
Significant differences were noted when long-term breastfeeding plans were analyzed according to parity [χ2 (4)=9.58; p<0.05]. For respondents for whom the present child was their first child (71 women), 70.4% reported that they planned to breastfeed for 6 months or longer relative to only 50% of those who had previously had at least one child. For those for whom the present child was their first, the distribution of planned breastfeeding duration was as follows: 11.3% reported they were not breastfeeding, 2.8% endorsed 2 weeks, 7% endorsed 1 month, and 8.5% endorsed 3 months. In contrast, the respective endorsement rates for those for whom this was not their first child (103 women) were as follows: 22.3%, 1.9%, 6.8%, and 19.4%.
When breastfeeding plans were analyzed according to demographics, Hispanic and black patients had the lowest rates of planned non-exclusive breastfeeding as well as higher rates of enrollment in WIC. Higher rates of planned breastfeeding in white patients coincided with lower WIC enrollment (Fig. 2).
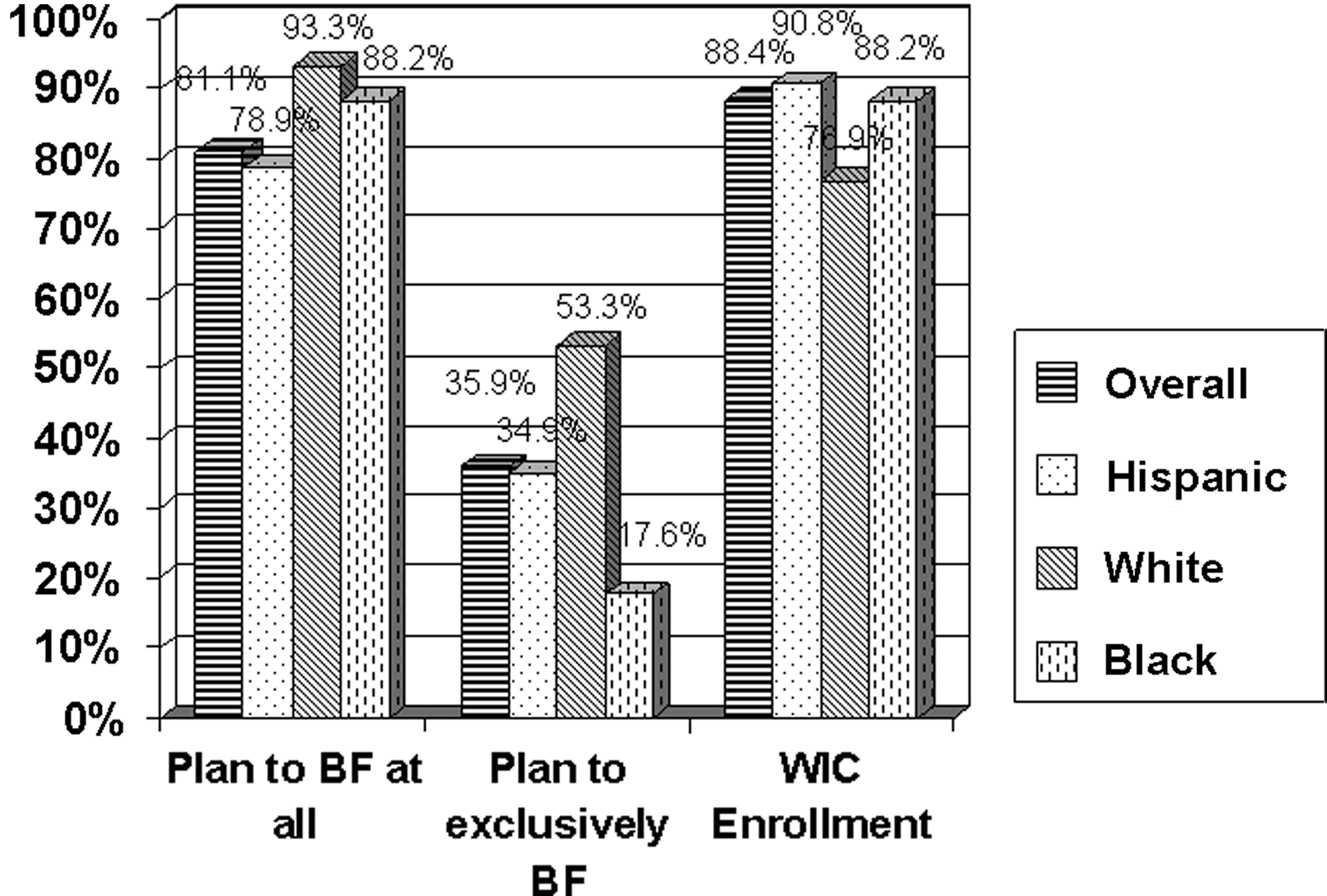
Infant breastfeeding (BF) plans and Special Supplemental Nutrition Program for Women, Infants and Children (WIC) enrollment among clinic patients by race.
Of those respondents who stated that they would not be breastfeeding, 85.7% acknowledged breastmilk provided adequate nutrition. When queried as to why they did not plan to breastfeed, 87.9% gave at least one reason. Receiving formula through WIC was cited as the most frequently endorsed reason not to breastfeed (48.3%; Table 1), closely followed by fear of pain (31%) and the need to return to work (24.1%). Similar trends were noted in women who planned to breastfeed and bottle feed (n=111). The exception was fear of pain: 9% versus 31% in those not planning on breastfeeding at all.
Note that multiple answers are possible.
WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
Patients were questioned as to why they were more likely to breastfeed their infant. The most common responses were the superior nutritional content of breastmilk (64.1%) and decreased rate of infections (48.6%). Patients were less concerned with the potential benefits of weight loss (14.28%) and the financial implications of breastfeeding (9.2%).
In an attempt to design more successful interventions to increase breastfeeding rates, the survey included questions about patient preferences and personal decision-making. The most influential person on the choice to breastfeed was the partner/spouse (45.2%), followed closely by the patient's mother (39.5%) and healthcare provider (24.2%).
When responses were analyzed by breastfeeding plans (Table 2), the only statistically significant difference was that those planning to exclusively breastfeed were more likely to endorse friends as the most influential person relative to those not planning to exclusively breastfeed (16.7% vs. 5.1%, respectively). The partner/spouse was endorsed as the most influential person most frequently by women not planning to breastfeed exclusively. However, in women planning exclusive breastfeeding, the mother was most often endorsed as the most influential person (50.0%), followed by the partner (40.5%). Healthcare providers were popular influences in both groups.
Numbers in parentheses represent the number of respondents endorsing each person as the one who influences them the most.
When asked about educational materials or modalities that they would be most interested in being provided, the most popular responses were access to a breastfeeding counselor (38.8%), parenting magazines (34.3%), and office videos (22.4%) (Fig. 3), while Facebook™ or Internet sites (16.4%), group classes (11.2%), and prenatal centering (9%) were less popular answers, although more then half of all participants reported regularly using services such as the Internet, Facebook, and texting.

Clinic patient interest in breastfeeding (BF) educational modalities. Note that multiple answers are possible.
Participants were also queried about their interest in breastfeeding products or accessories. Breast pumps were the most commonly considered product (48.3%), but several patients were also planning on using some sort of assistance device such as nursing bras (31.5%), nursing covers/blankets (27.3%), pillows (26.6%), and nipple shields (24.5%).
Discussion
The majority of the survey respondents were young Hispanic women. This finding is consistent with the clinic's patient demographics (68% Hispanic, 16% black, and 9% white). Intended breastfeeding rates were noted to vary among ethnic backgrounds. Hispanic women were less likely to plan on non-exclusive breastfeeding and had the highest rate of WIC enrollment. Although these differences were not statistically significant in this study, this supports results of prior studies, which have indicated cultural differences in breastfeeding rates and intentions. Such distinctions present unique challenges in patient education, as strong cultural and social traditions may heavily influence patient attitudes toward breastfeeding.
The survey confirmed low planned rates of exclusive breastfeeding among the Hartford Hospital Clinic population (35.3%). These results support recent institutional data showing that only 15% of clinic patients leave the hospital exclusively breastfeeding. Although variations occur in patient participation, the difference between the planned exclusive breastfeeding rates and the actual rates at the time of discharge raises the question of what happens between pregnancy and discharge to alter patient's plans. Interventions should be designed to not only increase the percentage of patients who plan to breastfeed exclusively, but also to support them in the immediate postpartum period so that they are not influenced to supplement infants with formula.
Belief in the nutritional adequacy of breastmilk (95.3%) and interest in the immunological benefits of breastfeeding for the infant (48.6%) was high among this population, although lower rates of planned and actual breastfeeding indicate compelling barriers to breastfeeding in clinic patients. Although such barriers may have complex cultural and sociological roots, the data gathered in our survey indicate the areas in which these barriers play a key role in influencing decisions surround breastfeeding.
An overwhelming number of respondents were enrolled in WIC (88.4%), which provides mothers with food and formula. Although programs such as WIC have numerous benefits to underserved patients, WIC enrollment was the most popular reason given for not breastfeeding. The degree to which the benefits of the WIC program outweigh this drawback is an intriguing area for further study. Although the clinic serves patients at or below the poverty level, only 9.2% of women cited the benefit of breastmilk being more economical, likely because the majority of patients receive formula for free. However, the economic need for the patient to quickly return to work outside the home may contribute to the addition of formula in the early postpartum period. The potential benefit of improved postpartum weight loss was also not a popular concern among those surveyed.
Conclusions
High WIC enrollment was associated with low breastfeeding rates when patients receive free formula. Interventions most likely to increase clinic patient breastfeeding rates include improved access to lactation counselors (either by phone or in person), informative parenting magazines, in-office video programming, and online social networking. These interventions should address the superiority of breastmilk for the infant and assist each mother in planning and maintaining a feeding regimen for her child after hospital discharge.
Footnotes
Acknowledgments
We thank Sarah Young.
Disclosure Statement
No competing financial interests exist.