
Abstract
Abstract
Background:
Women with a history of sexual assault are at increased risk for sleep difficulties and depression in their first year of motherhood. Breastfeeding improves sleep parameters and lowers risk of depression for women in general. However, it is unknown whether breastfeeding is related to maternal depression, sleep quality, and maternal well-being in sexual assault survivors. We examined the association between sexual assault and several indices of sleep, depression, and maternal well-being in a large sample of sexual assault survivors in the first year postpartum. We also explored whether feeding method was related to our outcome variables for both sexually assaulted and non-assaulted women.
Subjects and Methods:
A sample of 6,410 mothers of infants 0–12 months old participated in the online Survey of Mothers' Sleep and Fatigue; 994 women had a history of sexual assault.
Results:
As predicted, women with a history of sexual assault had a number of sleep difficulties, increased risk of depression, and overall poorer subjective well-being than their non-assaulted counterparts. However, sexual assault survivors who were breastfeeding were at lower risk on all of the sleep and depression parameters than sexual assault survivors who were mixed or formula feeding.
Conclusions:
Sexual assault has a pervasive negative effect on new mothers' sleep quality and risk of depression. However, these negative effects were less severe for the breastfeeding mothers than they were for the mixed- or formula-feeding mothers.
Introduction
Sleep problems in sexual assault survivors
One possible mechanism by which sexual assault might increase risk of depression is by compromising sleep quality. Several recent studies have found that both the number of hours that women report that they sleep and the number of minutes that it takes to get to sleep are related to risk of depression. A shorter number of reported hours of sleep and longer sleep latency (number of minutes it takes to get to sleep) are both related to increased risk of depression.4–6
Women with a history of sexual assault have a wide range of sleep difficulties. For example, Hulme 7 found that 52% of sexual abuse survivors in her primary-care sample reported that they could not sleep at night, 36% reported nightmares, and 53% reported intrusive thoughts. In a study of rape survivors, 8 80% had either sleep-breathing or sleep-movement disorders. Both of these disorders were linked to higher levels of depression and suicidality. Women who had both types of sleep disorders had the most severe depressive symptoms. The authors noted that for these women, fragmented sleep appeared to potentiate the symptoms they experienced after their assault, making coping with the aftermath of their sexual assault even more difficult. 8
Breastfeeding
There have been relatively few studies that have examined the impact of sexual assault on breastfeeding. Previous studies have focused on whether sexual assault decreases rates of breastfeeding. For example, Benedict et al. 9 studied 360 primiparous, predominantly African American women in Baltimore, MD. Of these women, 12% (n=43) were CSA survivors. Contrary to expectations, a higher percentage of sexual abuse survivors (54%) indicated an intention to breastfeed than their non-abused counterparts (41%).
Prentice et al. 10 recorded similar findings in a nationally representative sample of 1,220 mothers with children younger than 3 years of age. Of these women, 7% (n=85) indicated that they were CSA survivors. As with the previous study, women who had been sexually abused were more than twice as likely to initiate breastfeeding as their non-abused counterparts. More recently, Bowman et al. 11 found no difference in rates of breastfeeding among Mexican American teen mothers based on their CSA status. Their sample included 78 mothers, with 24 reporting a CSA history.
In all of these previous studies, the number of sexual assault survivors was relatively small. Furthermore, the data were mostly descriptive and limited to whether sexual abuse/assault survivors were more or less likely to breastfeed. These studies did not explore the relationship between breastfeeding and abuse sequelae, such as depression or sleep difficulties, and whether there was a difference among breastfeeding, mixed-feeding, and formula-feeding mothers. Breastfeeding may influence sexual assault sequelae because it down-regulates the stress response system.12,13 Breastfeeding specifically lowers levels of the stress hormones adrenocorticotropic hormone and cortisol 14 and of C-reactive protein.12,15 It also up-regulates oxytocin, which is protective of maternal mood. 12 When oxytocin is up-regulated, the stress response is down-regulated.
Breastfeeding's down-regulatory effect on the stress response is important for all new mothers. But, it may be especially important for mothers who have been sexually assaulted because trauma and previous depression both “prime” the stress response and make trauma survivors more vulnerable to subsequent life stress.16,17 Breastfeeding's down-regulatory effects can be seen in previous studies that have found that breastfeeding mothers have lower rates of depression.18,19 In addition, in a recent study using data from the same dataset as the present study, breastfeeding mothers had better sleep parameters (fewer minutes to go to sleep and more total hours of sleep) and overall higher scores of maternal well-being than mixed- or formula-feeding mothers. 18 In the present study, we also included four questions about mothers' self-reported well-being, including perception of overall physical health, daily energy, anger and irritability, and anxiety. The present study will allow us to explore the possible relationship between breastfeeding and sexual abuse sequelae, such as depression, sleep difficulties, and maternal well-being.
Based on previous studies, we hypothesized that new mothers with a history of sexual assault will have more sleep difficulties than non-assaulted women and as a result will report lowered daily energy and poorer physical well-being than new mothers without a history of sexual assault. We also hypothesized that women with a history of sexual assault will have higher risk of depression. In addition, the present sample provides opportunities to explore the relationship between breastfeeding and sequelae, including maternal sleep quality, depressive symptoms, and the other indices of maternal well-being in a large sample of postpartum sexual assault survivors.
Subjects and Methods
Sample recruitment
The sample was recruited via announcements and flyers distributed to Special Supplemental Nutrition Program for Women, Infants and Children breastfeeding coordinators, United States Breastfeeding Committee state breastfeeding coalition coordinators, lactation consultants, and La Leche League leaders in the United States, Canada, the United Kingdom, Australia, and New Zealand. The investigators described the study and asked for assistance in recruiting mothers. Flyers and cards were distributed electronically and via hard copy, with a Web link for the survey. This survey was open to all mothers with babies 0–12 months of age, regardless of feeding method.
Survey development and data collection
The data were derived from the 253-item Survey of Mothers' Sleep and Fatigue. The questions were predominantly close-ended in format and were developed for this study via open-ended interviews with mothers and feedback from mothers and healthcare professionals. Data were collected via an online survey that was available on the Texas Tech University Department of Pediatrics Web site. A screening question asked for the baby's age. If the response was 12 months or less, the mother was allowed to continue the survey. The survey and data collection procedure was reviewed and approved by the Texas Tech University School of Medicine Institutional Review Board.
Survey items for the present analyses
Feeding method was assessed with a series of questions about how and what babies were fed. For the present analysis, an overall summary question was used where mothers selected from one of three options: “Since your baby was born, did you breastfeed, formula feed, or both breast and formula feed?”
Mothers were asked to indicate how many hours they slept in an average night. They were also asked to rate their daily energy and overall physical wellbeing on a 5-point Likert scale. Mothers were also asked to rate their anger and irritability (“How often would you say that you are angry or irritable?”) and their anxiety (“How often would you say that you are really anxious, nervous, or afraid?”). Both of these items had 4-point responses: rarely or never, once or twice a week, or nearly every day.
Depression was assessed via the Patient Health Questionnaire-2 (PHQ-2), a two-item screening tool for depression that is used in primary-care settings. 20 Each symptom (depressed mood and anhedonia) was rated on a scale of 0 to 3. The combined score indicated risk of depression, with a higher score indicating greater risk. Means were reported for each of the three feeding groups. A previous article indicated that mothers who were breastfeeding only had significantly lower scores on the PHQ-2 and significantly higher scores on measures of maternal well-being than their mixed- or exclusively formula-feeding counterparts. 18 There was no significant difference between mixed and formula feeding on any of the measures. For the present analyses, the mixed- and formula-feeding groups were combined. In addition, we asked mothers, “How many times have you been depressed?”
The women were identified with a history of sexual assault if they answered “yes” to at least one of two questions: (1) As part of a series of questions on contact CSA, women were asked if they had experienced oral, vaginal, or anal penetration when they were under the age of 18 years with a partner at least 5 years older. (2) To ask about possible peer, partner, or stranger assault, women were asked: “Have you ever been raped or sexually assaulted as a teen or adult?” This question was part of a series about other types of psychological trauma women might have experienced. Both types of sexual assault could have occurred either inside or outside the women's families.
Data analysis
Data were analyzed using two-way analysis of variance using SPSS version 18.0 (SPSS, Inc., Chicago, IL), with feeding method and sexual assault history as the two main factors.
Results
Sample demographics
There were 6,410 women who participated in the Survey of Mothers' Sleep and Fatigue in 2008–2009, representing 59 countries (Table 1). 21 Demographic characteristics for the U.S. sample (n=4,789) are listed in Table 2. In total, 994 women indicated that they had been raped or sexually assaulted. Consistent with previous studies,9,10 sexual assault survivors were as likely to breastfeed (78.6%) as their non-assaulted counterparts (78.9%).
There were 4,774 mothers who indicated that they were breastfeeding only, 1,125 mothers who were both breastfeeding and formula feeding (mixed feeding), and 176 mothers who were exclusively formula feeding. Of the 6,410 women who participated in the study, 994 indicated that had been sexually assaulted. Two percent of the sample indicated that their CSA experiences including rape (vaginal, anal, or oral penetration), and 13% indicated that they had been raped or sexually assaulted as a teen or adult. Eight hundred fifty-seven of these women reported one type of sexual assault (either child or teen/adult), and 137 reported experiencing both types. The descriptive data on the outcome variables are listed on Table 3.
PHQ-2, Patient Health Questionnaire-2.
Sleep quality
Total hours of sleep
As predicted, women who were sexually assaulted reported fewer hours of sleep (mean=6.442, SD=1.320) than their non-assaulted counterparts (mean=6.591, SD=0.1230) (F1,5837=14.073, p<0.000, partial η 2 =0.002). The main effect for feeding method was also significant, where breastfeeding women reported more hours of sleep (mean=6.613, SD=1.247) than mixed- or formula-feeding women (mean=6.396, SD=1.232) (F1,5837=26.791, p<0.000, partial η 2 =0.005), regardless of sexual assault status. The interaction between feeding method and sexual assault was not significant (F1,5837=2.727, p=0.099) (Fig. 1).
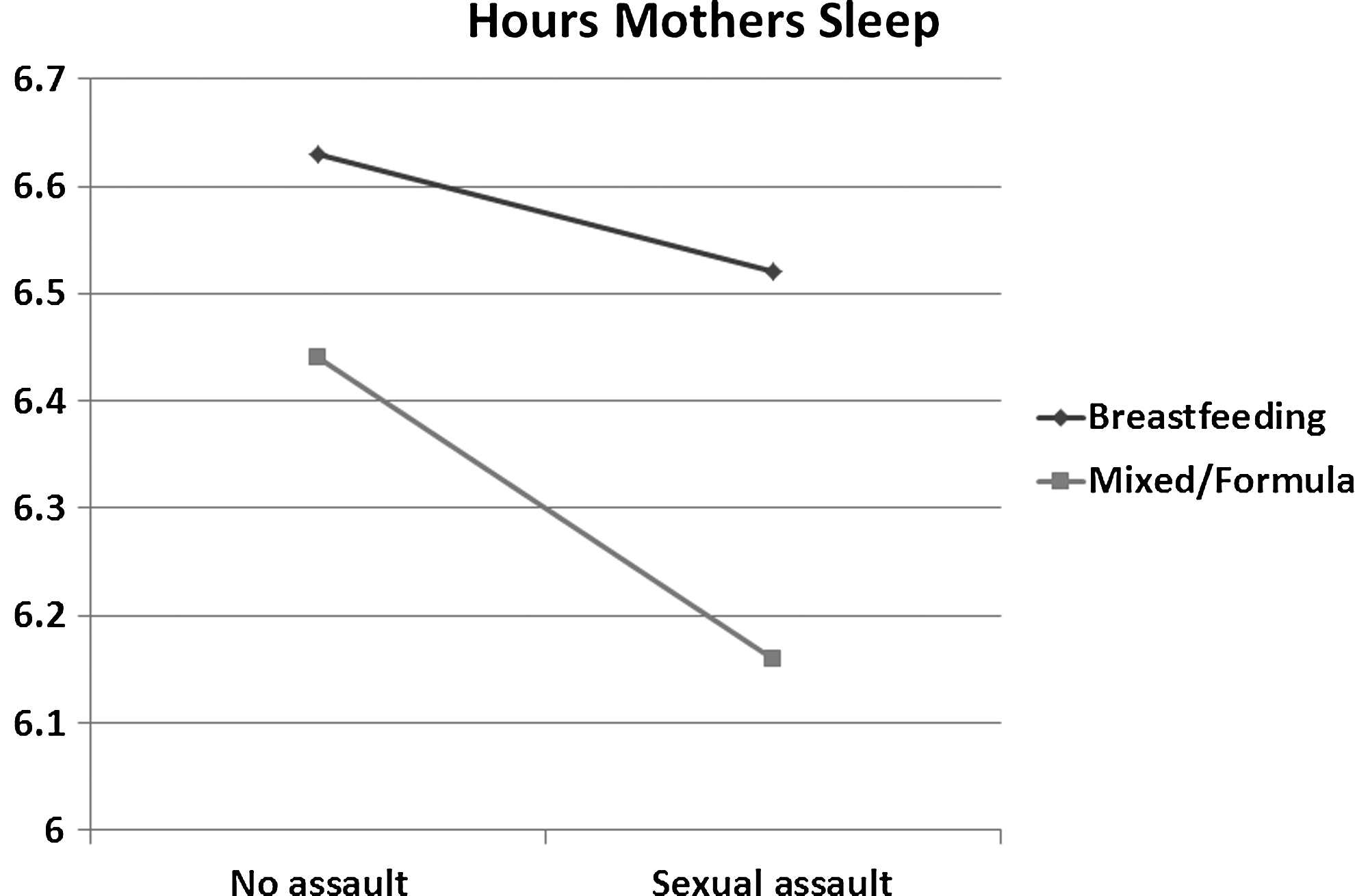
Total hours that mothers sleep.
Minutes to get to sleep
As predicted, women with a history of sexual assault reported significantly more minutes to get to sleep (mean=24.537, SD=19.976) than non-assaulted women (mean=19.441, SD=16.890) (F1,6020=46.600, p<0.000, partial η 2 =0.008). The main effect for feeding method was also significant, where breastfeeding women reported significantly fewer minutes to get to sleep (mean=19.575, SD=17.115) than mixed- or formula-feeding women (mean=22.875, SD=18.784) (F1,6020=19.234, p<0.000, partial η 2 =0.003), regardless of sexual assault history. The test for interaction was not significant (F1,6020=0.019, p=0.890) (Fig. 2).
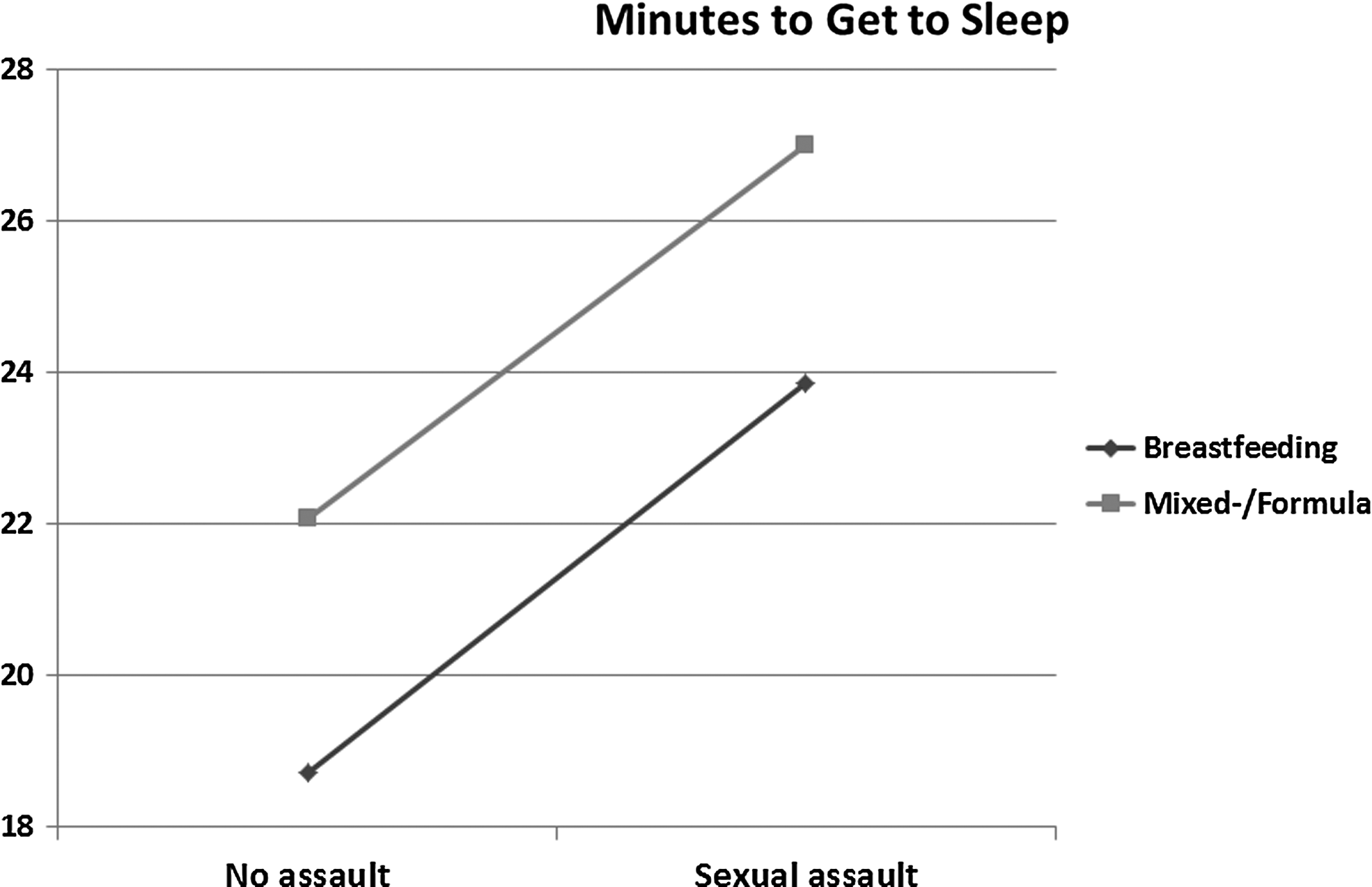
Mothers' reported minutes to get to sleep.
Maternal well-being
Self-reported physical health
The main effect for sexual assault history was significant (F1,6017=28.203, p<0.000, partial η 2 =0.005). Sexually assaulted women reported poorer overall physical health (mean=3.530, SD=0.878) than their non-assaulted counterparts (mean=3.706, SD=0.826). The main effect for feeding method was also significant (F1,6017=88.192, p<0.000, partial η 2 =0.014), where breastfeeding women reported better physical health (mean=3.745, SD=0.817) than mixed- or formula-feeding women (mean=3.427, SD=0.865), regardless of sexual assault status. The test for interaction was not significant (F1,6017=0.242, p=0.623) (Fig. 3).
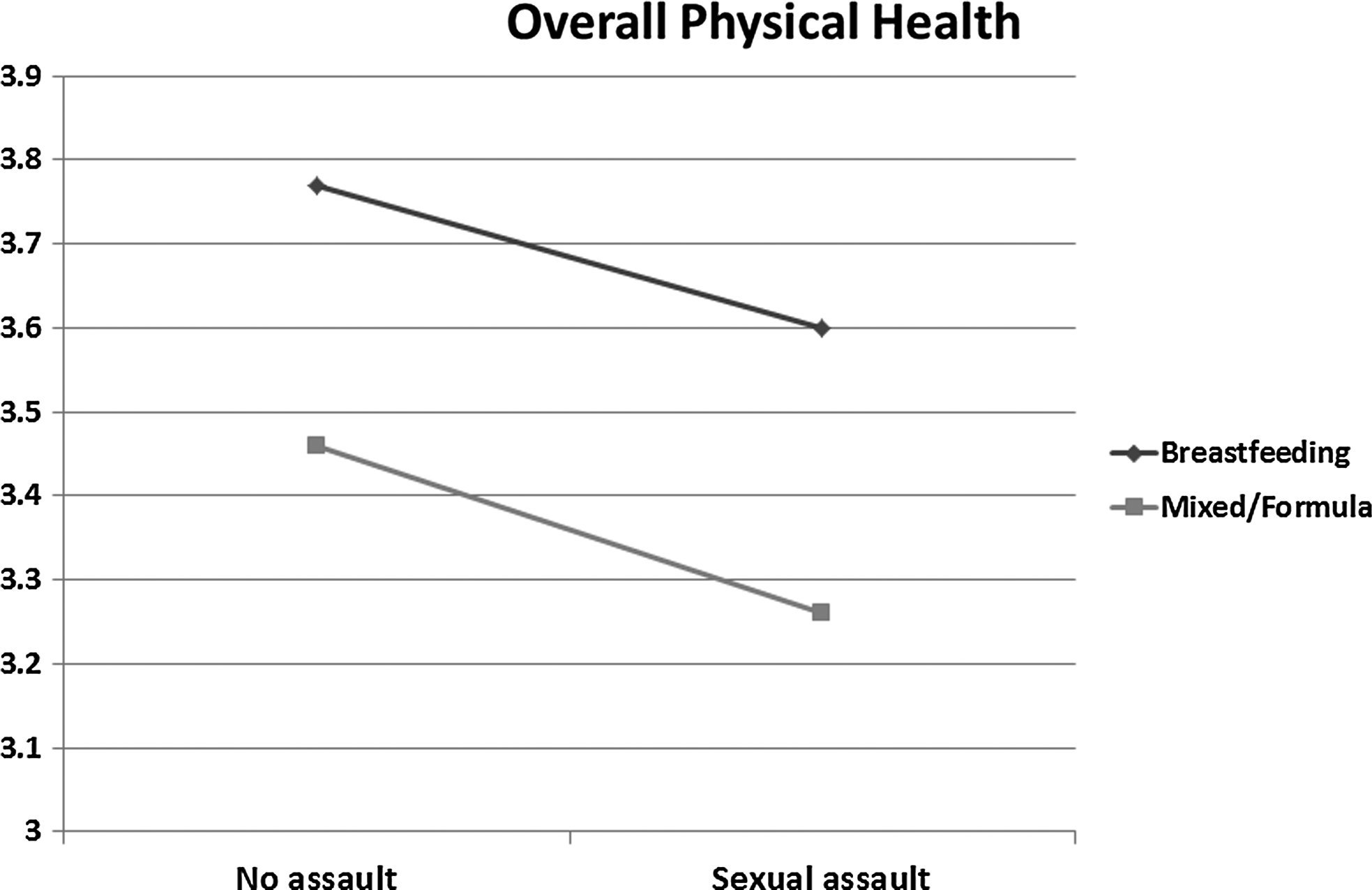
Mothers' self-reported overall physical health.
Daily energy
There was a significant main effect for sexual assault history (F1,6029=5.879, p=0.015, partial η 2 =0.001), where the energy level of sexually assaulted women (mean=2.919, SD=0.890) was somewhat lower than that of their non-assaulted counterparts (mean=2.993, SD=0.843). The main effect for feeding method was significant (F1,6029=56.176, p<0.000, partial η 2 =0.009), where breastfeeding women reported more daily energy (mean=3.036, SD=0.842) than mixed- or formula-feeding women (mean=2.781, SD=0.855) regardless of sexual assault status. The test for interaction was not significant (F1,6029=0.356, p=0.551) (Fig. 4).
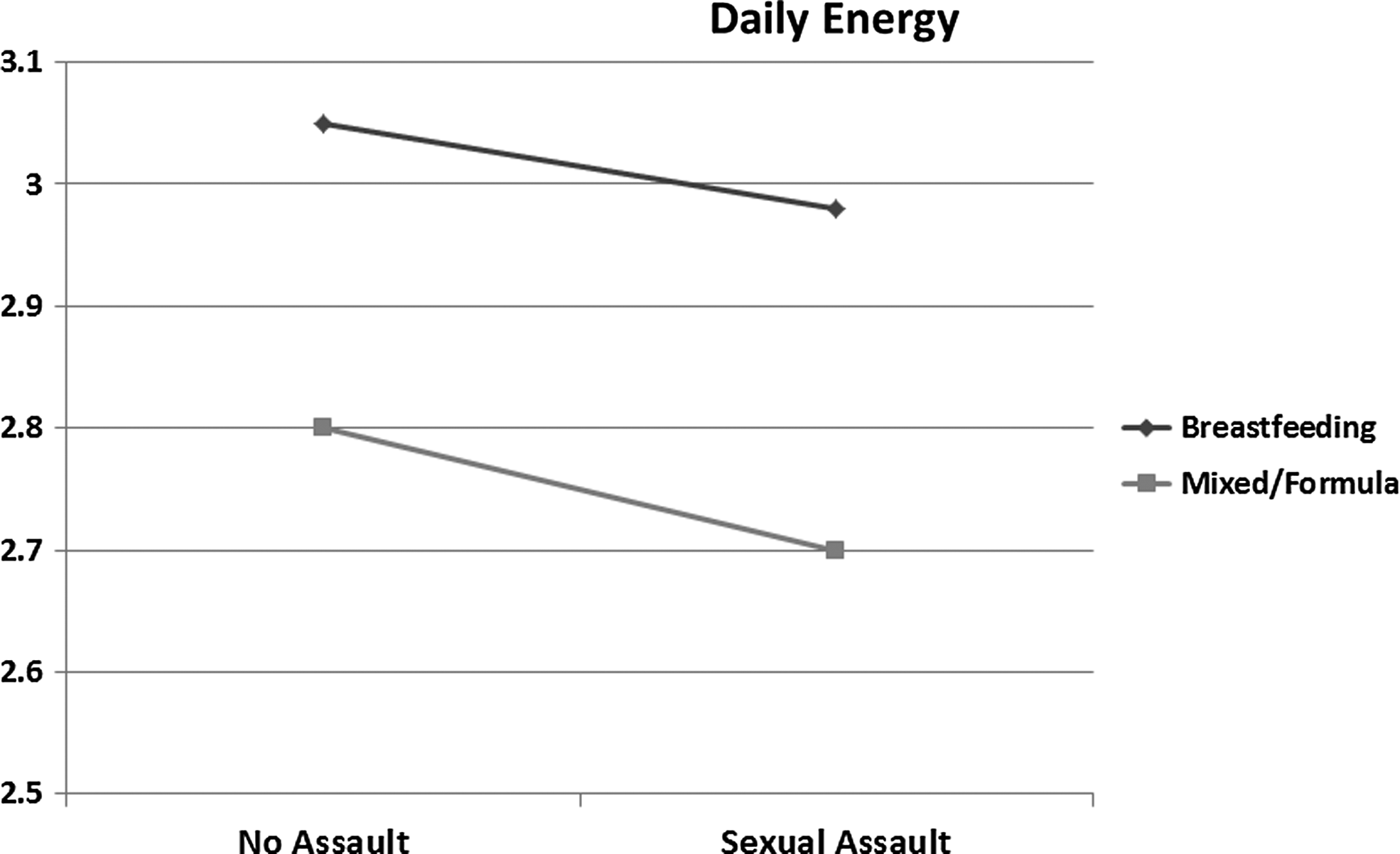
Mothers' reported daily energy.
Anger and irritability
The main effect for sexual assault was marginally significant (F1,6,022=5.406, p=0.073, partial η 2 =0.001); the sexually assaulted women reported that they are more often angry and irritable (mean=1.545, SD=0.955) than their non-assaulted counterparts (mean=1.494, SD=0.928), but not significantly so. The main effect for feeding method was significant (F1,6,022=7.793, p=0.005, partial η 2 =0.001), where breastfeeding women reported less anger and irritability (mean=1.489, SD=0.928) than mixed- or formula-feeding women (mean=1.552, SD=0.948), regardless of sexual assault history. The test for interaction was marginally significant (F1,6022=3.221, p=0.073) (Fig. 5).
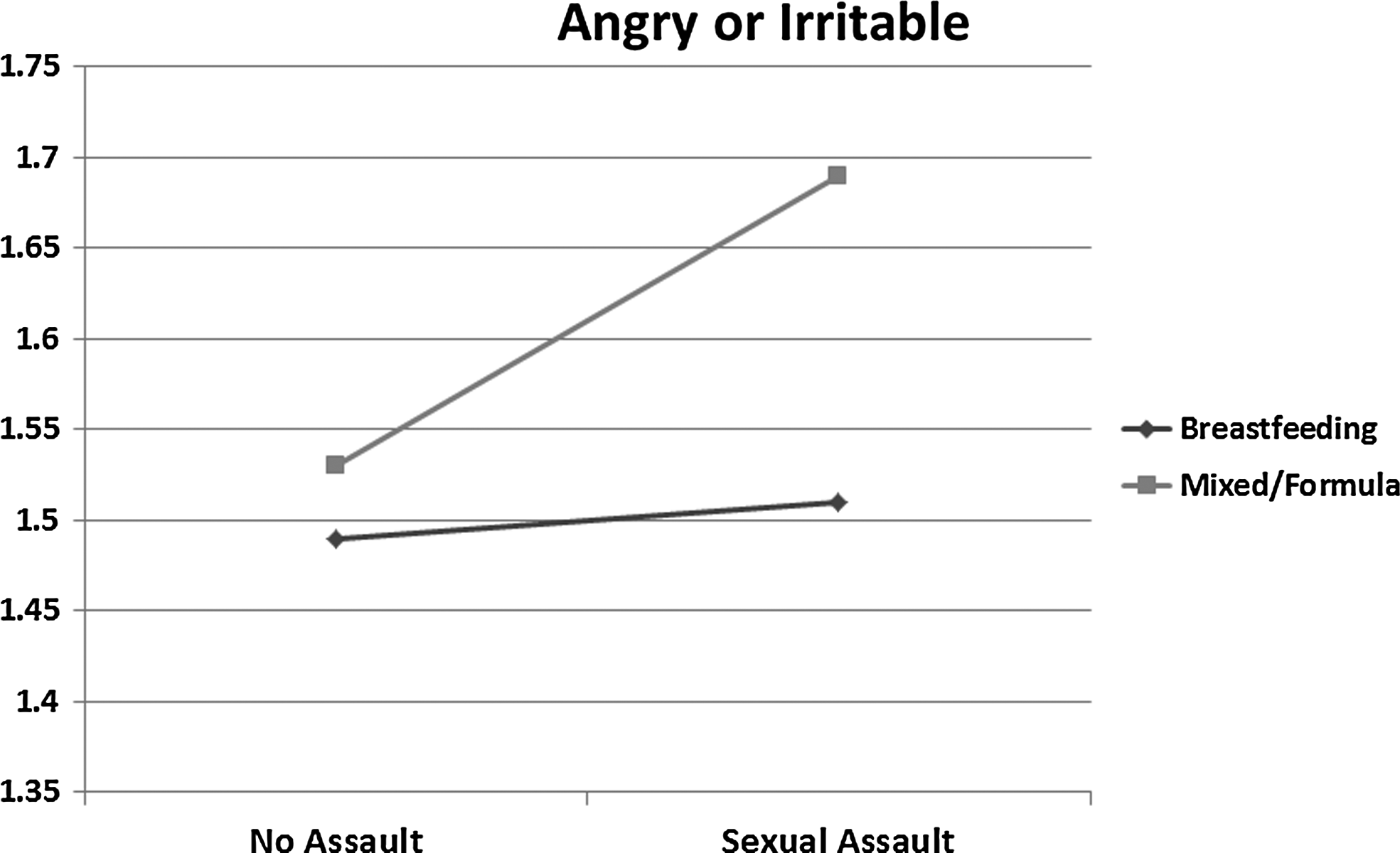
How often mothers report that they are angry or irritable.
Self-reported anxiety
The main effect for sexual assault history was significant (F1,6024=23.560, p<0.000, partial η 2 =0.004), where sexually assaulted women reported feeling anxious or afraid more often (mean=1.142, SD=1.057) than their non-assaulted counterparts (mean=0.958, SD=1.006). The main effect for feeding method was also significant (F1,6024=20.698, p<0.000, partial η 2 =0.003), where breastfeeding women reported feeling anxious or afraid less often (mean=1.489, SD=0.928) than mixed- or formula-feeding women (mean=1.552, SD=0.948), regardless of sexual assault history. The test for interaction was not significant (F1,6024=0.964, p=0.326) (Fig. 6).
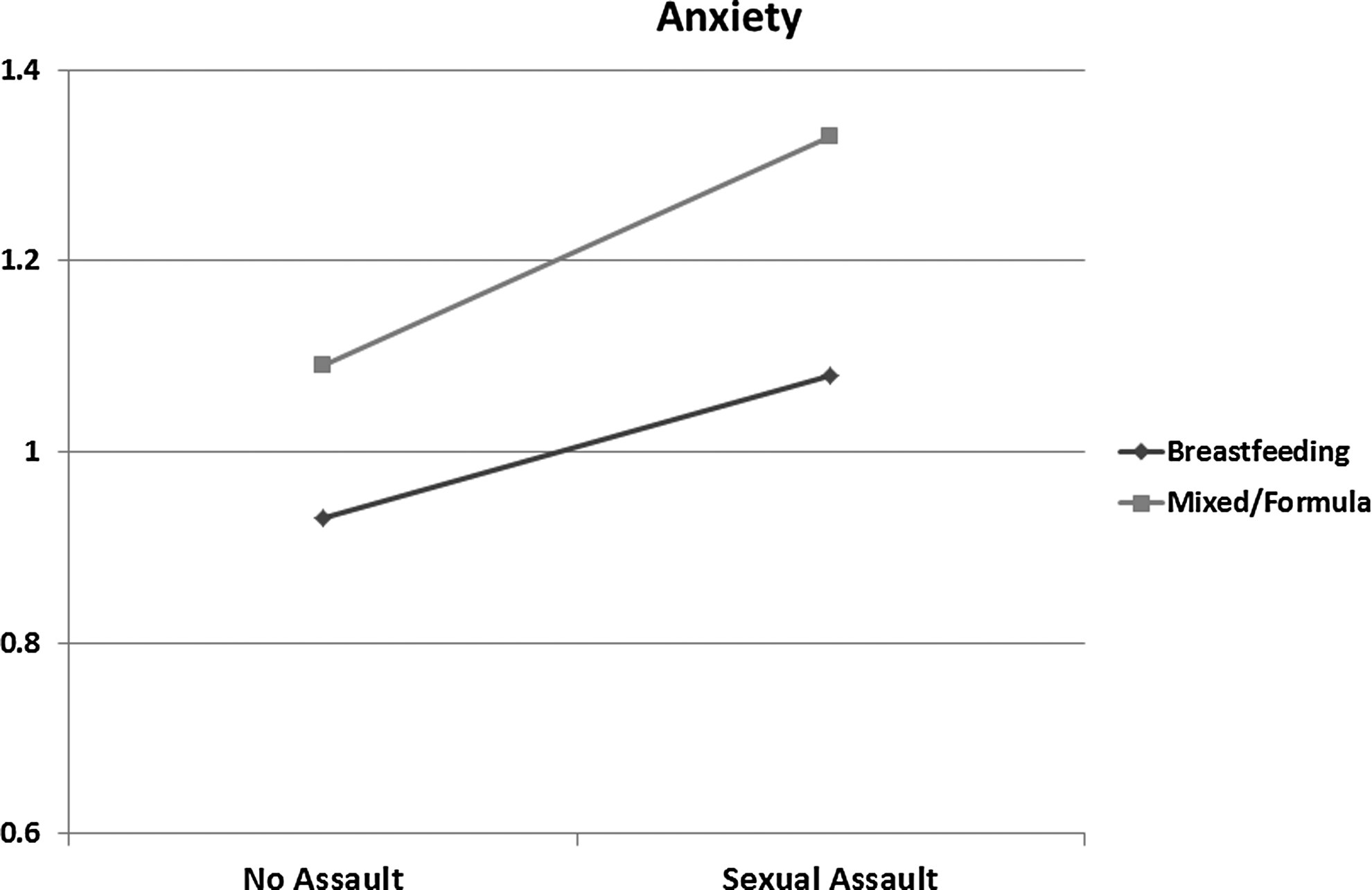
Mothers' report of how often they are really anxious or afraid.
Depression
The main effect for sexual assault history was significant (F1,5976=20.010, p<0.000, partial η 2 =0.003). Sexually assaulted women had a significantly higher score on the PHQ-2 (mean=1.113, SD=1.454) than their non-assaulted counterparts (mean=0.853, SD=1.266). The main effect for feeding method was also significant (F1,5976=14.060, p<0.000, partial η 2 =0.002), where breastfeeding women had significantly lower scores on the PHQ-2 (mean=0.849, SD=1.270) than mixed- or formula-feeding women (mean=1.070, SD=1.401). The test for interaction was not significant (F1,5976=0.164, p=0.689) (Fig. 7).
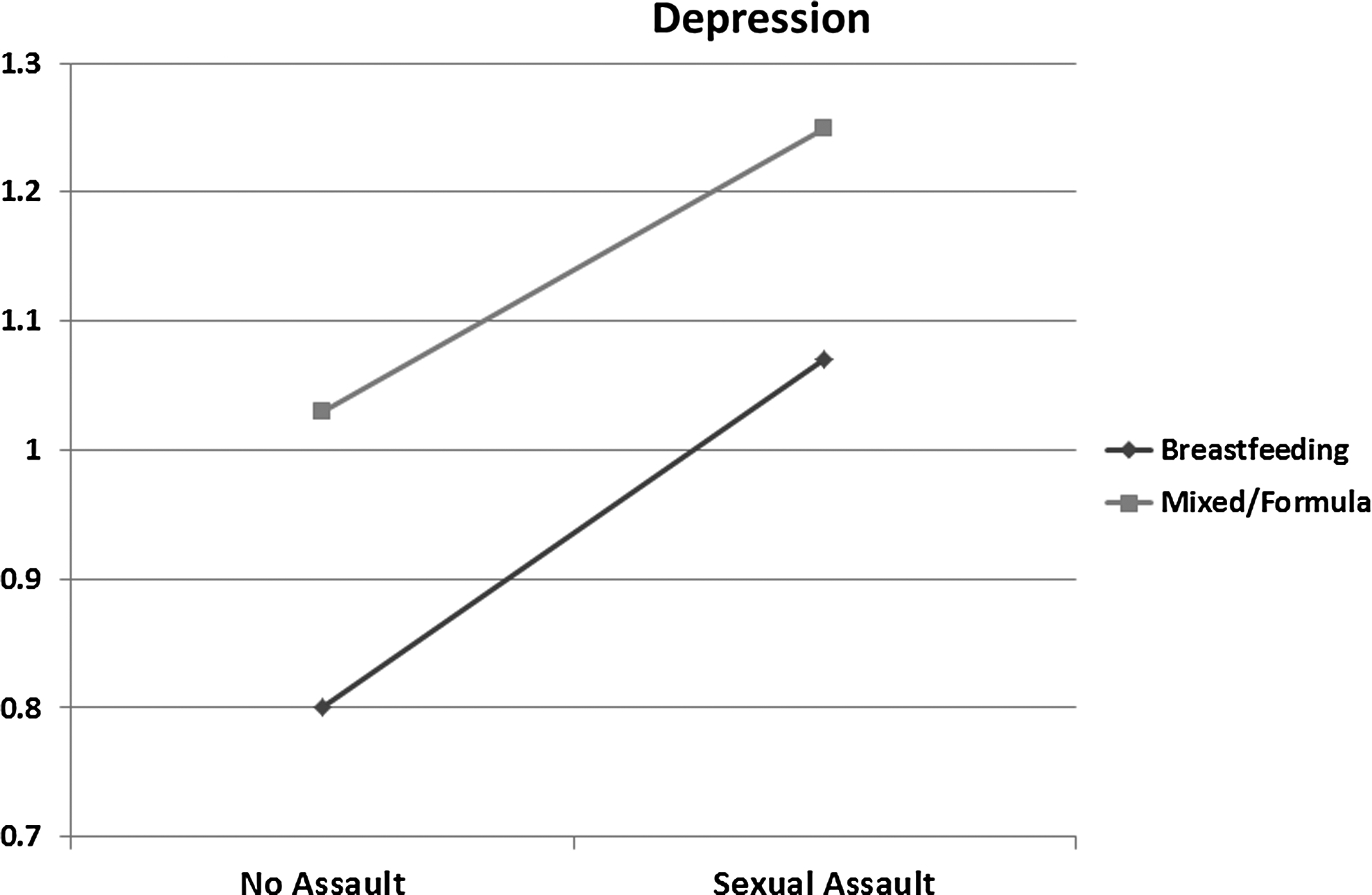
Mothers' depression score on the Patient Health Questionnaire-2.
For the additional measure of depression, how many times mothers had been depressed, the interaction was significant (F1,6022=7.222, p=0.007, partial η2=0.001). There was also a significant main effect of sexual assault history (F1,6022=151.908, p<0.000, partial η2=0.025), where women who had been sexually assaulted had more previous episodes of depression (mean=0.942, SD=0.847) than non-assaulted women (mean=0.582, SD=0.776). In addition, there was a main effect of feeding method (F1,6022=21.032, p<0.000, partial η 2 =0.003), where breastfeeding women reported fewer episodes of previous depression (mean=0.622, SD=0.788) than mixed- or formula-feeding women (mean=0.714, SD=0.833). Further analyses revealed that among breastfeeding women, those who had been sexually assaulted reported 0.322 more episodes of depression than non-assaulted women (t4736=10.569, p<0.000). Among mixed- or formula-feeding mothers, the sexually assaulted women reported 0.502 more episodes of depression than non-assaulted women (t1286=8.184, p<0.000). One possible interpretation is that the effects of sexual assault on breastfeeding mothers were less severe than those on mixed- or formula-feeding mothers. Another interpretation is that women who reported fewer lifetime episodes of depression were more likely to breastfeed (Fig. 8). This topic should be further addressed in future research.
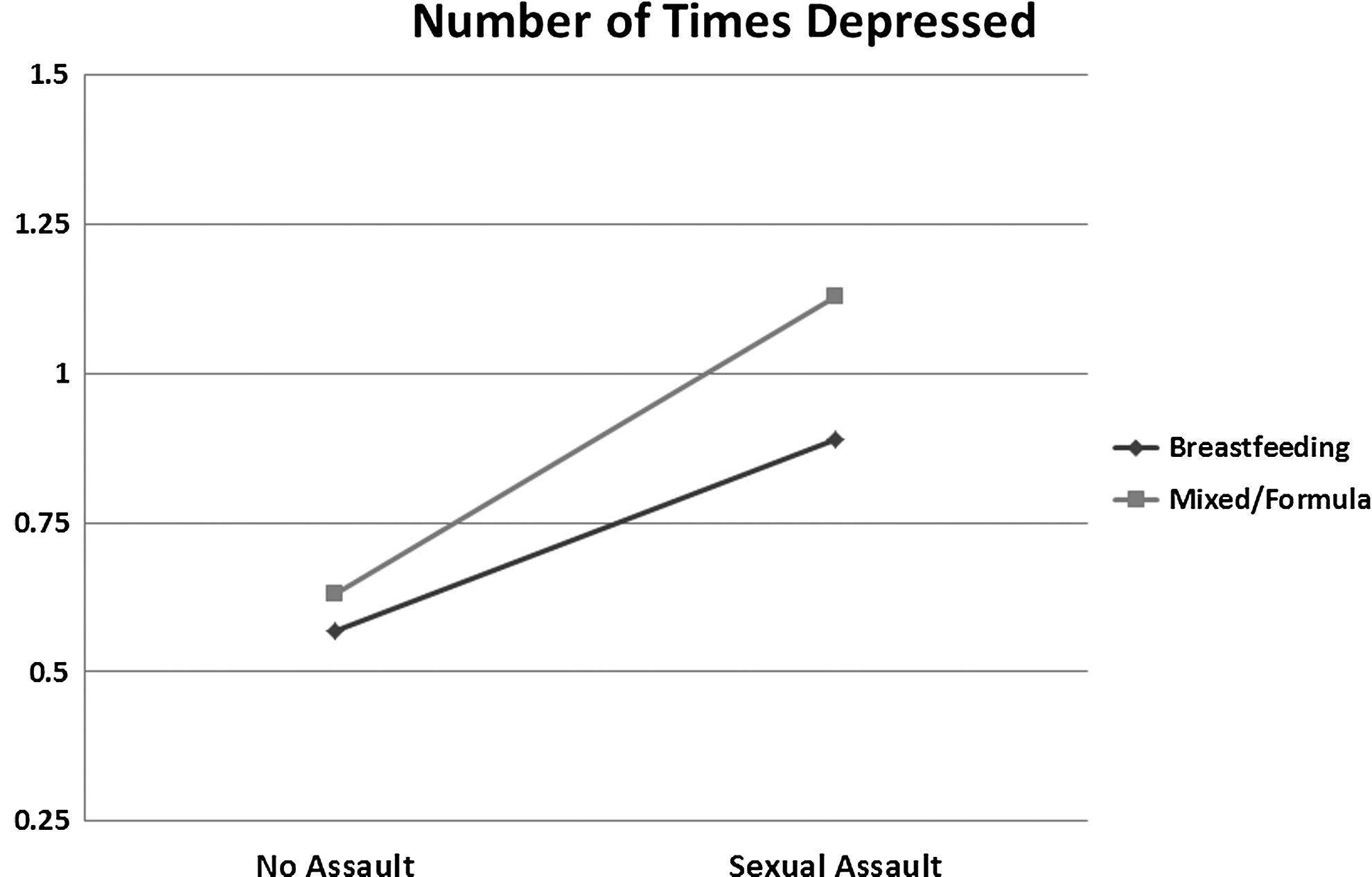
Number of times mothers have been depressed.
Discussion
As predicted, previous sexual assault did increase women's risk of depression by producing a negative impact on women's total sleep time and the number of minutes it took to fall asleep. Furthermore, women with a history of sexual assault had significantly higher depression scores on the PHQ-2 than their non-assaulted counterparts and reported more lifetime episodes of depression. Sexually assaulted women also reported lower ratings of their physical health and higher rates of self-reported anger and irritability and of anxiety. Sexual assault history was not related to women's self-reported daily energy. Feeding method also impacted the variables related to maternal well-being and risk of depression. Breastfeeding women reported more hours of sleep and fewer number of minutes to get to sleep than their mixed- or formula-feeding counterparts. Breastfeeding women reported better physical health, more daily energy, less anger and hostility, and less anxiety than mixed- or formula-feeding women. The breastfeeding rates were the same for sexually assaulted and non-assaulted women. Finally, breastfeeding women had lower depression scores on the PHQ-2 than mixed- or formula-feeding women.
For almost all the analyses, sexually assaulted women fared worse than their non-assaulted counterparts, indicating that this population is at high risk for depression and other postpartum adjustment issues. In contrast, the breastfeeding women fared better than their mixed- and formula-feeding counterparts on almost every measure, indicating that breastfeeding women are at lower risk for depression, also consistent with previous studies. Although only one interaction was significant, our results suggest that breastfeeding has important health effects for all women but may be particularly important for women who have a history of sexual assault because breastfeeding women showed less severe negative effects. Therefore, breastfeeding should be recommended to all women despite of their sexual assault history. Breastfeeding did not take away all of the negative effects of sexual assault. But, the breastfeeding sexual assault survivors had better scores on almost every variable than the mixed- or formula-feeding sexual assault survivors. However, for all but one variable, we did not find moderating effects of breastfeeding on our outcome variables. As described earlier, one possible explanation for why breastfeeding might impact sexual abuse sequelae is breastfeeding's down-regulatory impact on the stress response.12,13,22 This has been found in several studies. One study measured mood and stress in women who were both breastfeeding and bottle feeding. 23 The researchers found that breastfeeding increased positive mood and bottle feeding increased negative mood in the same women. In another study, suckling at the breast lowered levels of the stress hormones adrenocorticotropic hormone and cortisol more than simply holding the baby. 14 Furthermore, breastfeeding women were less responsive to a lab-induced stressor in the 30 minutes after they fed their babies at the breast than they were at other times. Breastfeeding's down-regulation of the stress response specifically decreases women's risk of depression. 22 Furthermore, breastfeeding's impact on sleep quality can also decrease women's fatigue and increase their overall well-being, which decreases their risk for depression.
One limitation of our study is the lack of standardized measures for anxiety or psychological trauma. The use of an additional measure of depression revealed the interaction effect between sexual assault history and feeding method on depression, which was not identified by using PHQ-2. But, a more detailed measure of depression, in addition to the PHQ-2, might have also been helpful.
Our question about rape/sexual assault as a teen or adult did not specify the behavior that the women experienced (i.e., oral, anal, or vaginal penetration), so it could have been interpreted more broadly. But, given the sequelae the women reported, we believe that the majority are interpreting the question to mean rape and not less serious types of sexual offenses. Under-reporting is always a possibility when attempting to measure rates of sexual assault; some sexual assault survivors in our sample may have chosen not to disclose on our survey. Our results are consistent with previous studies of non-perinatal samples. However, we recognize that we may not have captured the experiences of all sexual assault survivors in our sample.
Although we hypothesized that previous sexual assault and breastfeeding would affect mothers' well-being, we could not completely eliminate the possibility of a reverse causation. For example, mothers' previous history of depression may have made them less likely to initiate or continue breastfeeding. In addition, mothers with more severe sexual assault sequelae may have been less likely to breastfeed.
Another limitation is the small number of exclusively formula-feeding mothers, which may have also limited the generalizability of our findings. Moreover, sleep was also measured via self-report rather than objective measures, such as sleep actigraphy. However, two recent studies found that self-report measures were more predictive of depression than objective measures of sleep, including sleep actigraphs.4,5 Nevertheless, our findings suggest some areas to explore in future research.
In summary, the results of our study indicate that previous sexual assault is related to women's sleep difficulties, risk of depression, and overall impaired well-being in the postpartum period. Consistent with earlier studies—but contrary to what many assume—breastfeeding rates do not differ between women with a sexual assault history and their non-assaulted counterparts. Breastfeeding appears protective of all women but may be especially beneficial for women who have been sexually assaulted when depression, sleep, or maternal well-being is the outcome of concern. Therefore, sexually assaulted women who want to breastfeed should be strongly supported and encouraged to do so.
Footnotes
Disclosure Statement
No competing financial interests exist.