
Abstract
Abstract
Background:
Little is known about the effect of maternal age on human milk (HM) composition. This study was designed to study fat content, estimated by creamatocrit (CMT), in HM collected in the first 2 weeks of life in older (≥35 years) compared with younger (<35 years) mothers.
Study Design and Methods:
Ninety lactating mothers (48 older, 42 younger) of newborns were recruited within the first 3 days of delivery. CMTs were measured at 72 hours, 7 days, and 14 days after delivery for HM in a capillary tube after centrifugation at 5,366 g for 5 minutes.
Results:
The groups did not differ in terms of maternal height and diet, infant birth weight, gestational age (GA), or pregnancy weight gain. They differed significantly in terms of maternal age and parity. Mean colostrum CMT was significantly higher in the group of older mothers. Colostrum CMT correlated positively with maternal age (R2=0.11, p=0.006) and inversely with GA (R2=0.1, p=0.03) but did not relate with either maternal weight or body mass index. CMT at age 7 days and 2 weeks was not affected by maternal age or GA. In multivariate regression analysis colostrum CMT correlated significantly only with maternal age and GA (R2=0.3, p<0.001).
Conclusions:
Colostrum fat content of older mothers is much higher than that of younger mothers and inversely related with GA at delivery. This increase in colostrum fat content obtained from mothers with advanced age may be due to increased fat synthesis and excretion in milk, reduced water content of milk, or a combination of both.
Introduction
Older pregnant women have a higher rate of pregnancy complications such as hypertension, preeclampsia, and diabetes mellitus. 3 They may also be at a higher risk of delivering low birth weight infants (<2,500 g at birth) and macrosomic babies (>4,000 g at birth). Risk is higher for labor complications and cesarean deliveries. 4 In spite of all these above-mentioned outcomes, neonatal outcomes do not appear to be significantly affected. 3 The National Health and Nutrition Examination Surveys 1999–2006 reported that breastfeeding rates increase significantly with increasing maternal age. 5 However, the rates of breastfeeding in older primiparas were not separately reported in this survey. 5 Older mothers are prone to experience difficulty in establishing and maintaining lactation, as shown by Hytten, 6 who described a fall in the yield of milk with increasing maternal age.
Little is known about the effect of maternal age on human milk (HM) composition. Fat content provides an excellent estimate of caloric density of HM. 7 Fat content of HM expressed by older mothers has not been systematically analyzed. We therefore conducted this prospective study in a cohort of 72 breastfeeding mothers in order to compare the fat content of HM from older (≥35 years) versus that from younger (<35 years) women.
Subjects and Methods
Patients
We collected samples of expressed HM obtained from 90 mothers of newborn infants, with a gestational age (GA) at birth ranging from 25 to 41 weeks.
Forty-eight older (≥35 years) mothers were compared with 42 younger (<35 years) mothers. The older mothers were recruited from the delivery room of the Lis Maternity Hospital (Tel Aviv, Israel) and were consecutively approached. Those who intended to breastfeed were recruited after written informed consent was obtained. The study was approved by our local Institutional Review Board. We attempted to recruit the younger mothers group from those mothers <35 years of age who delivered after one specific older mother on the same day. We were able to recruit 42 such younger women. We excluded from both groups all major obstetrical and neonatal complications such as pregnancy-induced hypertension, maternal diabetes, asthma, plastic surgery of the breast, known dyslipidemia, and neonatal asphyxia and/or major neonatal complications. Preterm deliveries were not excluded, but GA at delivery was carefully determined, and prematurity was included in the analyses as a potential confounder.
Laboratory methods
After manual expression, each mother contributed three samples of HM: the first sample during the first 72 hours after labor (colostrum), the second after 7 days (transitional milk), and the third sample at 14 days postpartum (mature milk). Although the colostrum samples were obtained in the morning, the other twp samples were obtained from an evening expression (between 2100 and 2400 hours). All samples were mixed and stored at −20°C until analyzed.
The fat content was measured using the creamatocrit (CMT) method, as previously described.7–10 In brief, 75-μL aliquots were filled into glass capillary tubes, which were sealed at one end and spun in a hematocrit centrifuge for 5 minutes at 5,366 g. The CMT was read to the nearest 0.5 mm and expressed as a percentage of the length of the milk column in the tube. Each reading was performed in duplicate, and the average was calculated. This method is extremely precise and reproducible with a coefficient of variation of less than 1%. It highly correlates with total lipid biochemical measurements, 10 making it an “accurate inexpensive and useful technique for estimating lipid concentration” of expressed breastmilk. 10
Statistical analyses
The Minitab (State College, PA) Statistical Package version 16 was used for analyses. Variables were tested for normality, and Student's t tests or Kruskal–Wallis tests were used as appropriate to determine the differences between the two groups (maternal age ≥35 years and <35 years), whereas χ2 tests were used for categorical variables. Linear regression was used to determine the correlation between maternal age and the fat content in HM. Stepwise backward multiple regression was used to determine the effect of variables found to be significant statistically or clinically in univariate analysis of fat content. Results are expressed as mean±SD values or as median (range).
Results
Demographic and maternal characteristics of the participants in this study are presented in Table 1. The groups did not differ significantly in terms of maternal height and diet, infant birth weight, GA, maternal prepregnancy weight, pregnancy weight gain, body mass index, or mode of delivery, whereas they did differ significantly in terms of maternal age and parity (Table 1). The mean CMT levels in colostrum were significantly higher in the group of older mothers (Table 1). CMT in colostrum correlated positively with maternal age (R 2 =0.11, p=0.006) (Fig. 1) and inversely with GA (R 2 =0.1, p=0.03) (Fig. 2) but did not relate with either maternal weight or body mass index. CMT levels at ages 7 days and 2 weeks were not affected by maternal age.
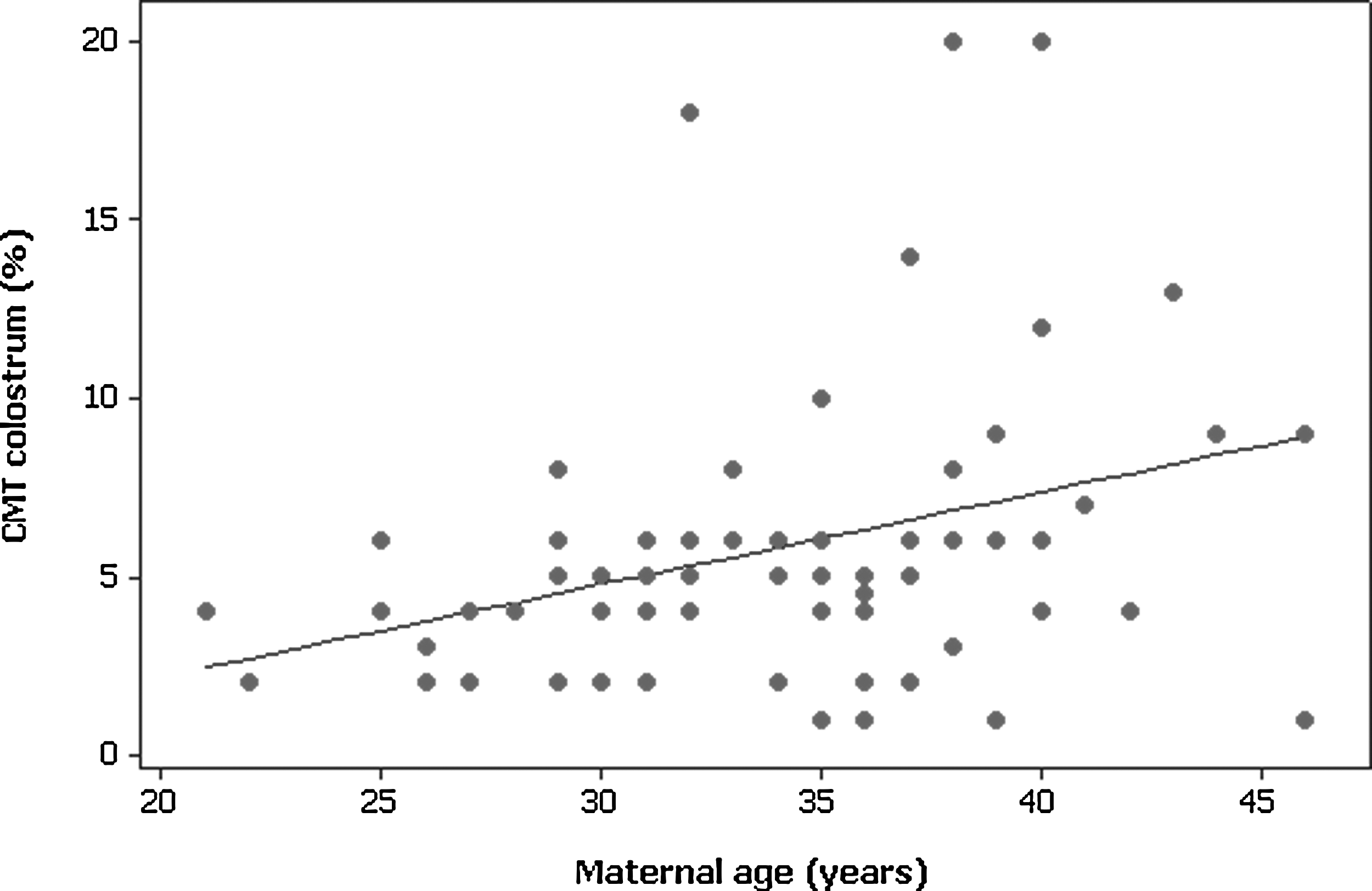
Correlation between creamatocrit (CMT) in colostrum (%) and maternal age (years). R2=0.11, p<0.006.
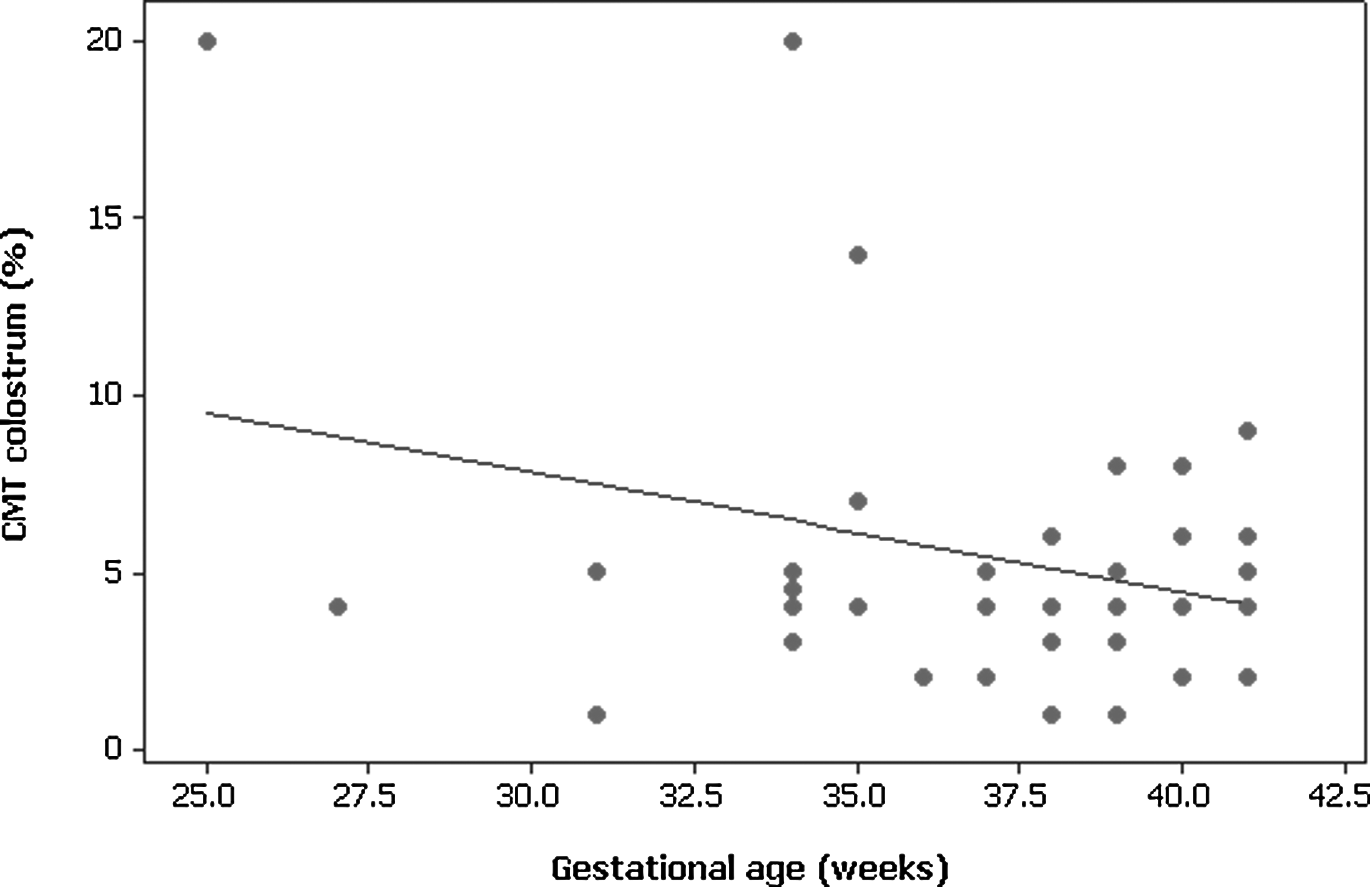
Correlation between creamatocrit (CMT) in colostrum (%) and gestational age (weeks). R2=0.1, p<0.03.
Data are mean±SD values except for parity, which is median (range).
BMI, body mass index; CMT, creamatocrit; NS, not significant.
We then conducted a multivariate regression analysis in order to determine the effect, if any of maternal age, GA, and parity (as independent variables) upon CMT in colostrum (dependent variable). Various models were used, depending upon the use of maternal age as a continuous or a dichotomous variable (below or above 35 years) and the use of GA as a continuous or a dichotomous variable (below or above 37 weeks). In all models, CMT in colostrum was correlated significantly only with maternal age and GA (R 2 =0.17 for the model, p<0.002) or maternal age and prematurity (R 2 =0.3 for the model, p<0.001).
Discussion
In this prospective study of fat content in HM during the first 2 weeks of lactation, we demonstrated that fat content of transitional or mature milk samples obtained from older (≥35 years) mothers was similar to that of samples obtained from younger (<35 years) mothers. Moreover, fat content, as expressed by the measurement of CMT, was affected neither by maternal age nor by GA at the time of delivery. In contrast, CMT values in colostrum were significantly affected by both maternal age and GA. In univariate analyses CMT correlated positively with maternal age and negatively with GA. These effects of maternal age and GA (or prematurity) upon CMT values remained significant in backward multiple regression analysis. In the latter analysis, variables such as maternal body mass index (which is by itself correlated with maternal age) or parity did not influence significantly colostrum CMT.
The reason why such CMT differences exist in colostrum alone but not in transitional or established mature milk is unclear. The biological significance of it is also unclear, and it is only possible to speculate whether the higher CMT in the colostrum of older mothers provide any selective advantage(s) to the infant.
As far as GA is concerned, many studies have examined the effect of preterm delivery upon HM composition.11–15 From these studies, it appears that daily HM output of mothers who deliver preterm infants is significantly lower compared with that of mothers who deliver at term. 15 The reasons for this apparent delay or deficiency in milk production are multiple: premature infants often are unable to breastfeed effectively for some time after delivery.14,15 Thus, mothers of premature infants may need to express their milk after delivery because of the inability of their infants to breastfeed. Milk expression with a mechanical breast pump may not be as efficient in removing milk and in creating sufficient nipple stimulation for effective milk production. 16 In addition, milk production decreases with lower GA, which may in part be due to incomplete mammary development because of the shortened pregnancy.12–14 For all these reasons lower volumes persist up to postpartum Day 10 in women who delivered before 28 weeks of gestation. 15 It is important that it appears that when milk volume is decreased, the concentrations of some nutrients appear to increase. For instance, the protein content is higher when milk volume is lower. 12 In our study, consistent with the findings of Anderson et al., 12 it appears also to be the case for fat content, which correlated inversely with GA. An obvious limitation to our speculation is that in this study daily milk volume was not measured in part because of practicality reasons and also because it is extremely difficult, in particular with small volumes of colostrum, to measure accurately the daily output.
As far as maternal age is concerned, we also can only speculate about our findings. We suggest that a similar explanation (i.e., low milk volume) might be valid. Older mothers are prone to experience difficulty in establishing and maintaining lactation, as shown by Hytten, 6 who found a fall in the yield of milk with increasing maternal age. This may be due to both a significant decrease in the density of milk glands with increasing age17,18 and possibly, as well, to a change in hormonal milieu with increasing age. For instance, there is a lifelong reduction in blood prolactin levels. 19 Thus, a reduction in volume of milk might also, by a similar mechanism, be linked to a relative increase in fat concentration. If this is the case, this might explain why, at 1 and 2 weeks, when milk production is better established, maternal age, as well as GA, is no longer influential upon fat content of milk.
We conclude that fat content of colostrum obtained from mothers of advanced age is elevated compared with that of younger mothers. We also showed that this increase is significant, even after taking into account prematurity, which also happens to have a similar effect on CMT. We speculate that the maternal age increase in CMT may be due to increased fat synthesis and excretion in milk, reduced water content of milk, or a combination of both. Further studies that will involve simultaneous measurement of milk and colostrum volume as well as of CMT may answer this question.
Footnotes
Disclosure Statement
No competing financial interests exist.