
Abstract
Abstract
Background:
Breastfeeding within the first hour of life is a potential mechanism for health promotion and is considered to be an indicator of excellence of breastfeeding. This study was conducted to evaluate the knowledge, attitude, and practice regarding early breastfeeding initiation within the first hour of life in both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital, Minia, Egypt.
Subjects and Methods:
A study was conducted on four groups of participants from both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital, each of them consisting of 30 individuals, using a questionnaire to assess the knowledge, attitude, and practice regarding early breastfeeding initiation for each group.
Results:
Sixty percent of women delivered by spontaneous vaginal delivery and 16.7% of those delivered by cesarean section initiated breastfeeding within 30 minutes to 1 hour after birth. Forty percent of lactating women delivered by spontaneous vaginal delivery, 83.3% of lactating women delivered by cesarean section, and 36.7% of healthcare workers used prelacteal feed instead of early breastfeeding initiation. The most important factors affecting the breastfeeding initiation were maternal illness followed by immediate skin-to-skin contact.
Conclusions:
Although the majority of women participating in this study exhibited knowledge about early breastfeeding initiation, actual application of this practice was clearly deficient. In order to improve the rates of breastfeeding initiation within the first hour of life we should enhance vaginal delivery and prenatal classes and implement Baby-Friendly Hospital Initiative policies in both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital.
Introduction
Despite the inclusion of breastfeeding within 30 minutes to 1 hour of birth in international child feeding recommendations, 4 much of the focus of breastfeeding advocacy and research has been on exclusive breastfeeding rather than an early initiation The recent finding that early initiation could substantially reduce neonatal mortality5,6 should result in more comprehensive efforts to increase the number of infants breastfed within 30 minutes to 1 hour of birth.
The present study was designed to evaluate knowledge, attitude, and practice regarding early start of breastfeeding in both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital, Minia, Egypt.
Subjects and Methods
The present study, done between April and June 2011, was conducted on four groups of participants from both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital, with each group consisting of 30 individuals.
The study population was grouped as follows: antenatal group, including 30 women receiving antenatal care (Group I); vaginal delivery group, including 30 women shortly after normal labor (Group II); cesarean section group, including 30 women shortly after cesarean section (Group III); and health workers, including 30 women from our healthcare workers (15 nurses, 15 doctors), some of them from the Pediatrics Department and the rest from the Gynecology and Obstetrics Department (Group IV).
Knowledge, attitude, and practice regarding early start of breastfeeding and use of prelacteal fluid were evaluated.
Sample size
The sample of the present study was 120 mothers attending, delivered, or working in Minia University Hospital who were selected by systematic random sampling.
Data were collected with the help of an interview schedule of knowledge, attitude, and practice questionnaires where the answers were filled by the investigator herself after an oral interview with the participants from April 2011 to June 2011. Approximately four subjects were interviewed per day (12 per week), with about 30 minutes spent with each participant.
Ethical consideration
The investigator personally introduced herself to the participants and explained the purpose of the study and ascertained their willingness to participate. The respondents were assured anonymity and confidentiality of the information they provided.
Criteria of data collection
The following criteria were set for selection of the sample. Inclusion criteria were as follows: (1) pregnant women who attended the antenatal clinic of the Gynecology and Obstetrics Department of Minia University Hospital during the data collection period and were willing to participate in the study; (2) lactating women delivered in the maternity ward of the Gynecology and Obstetrics Department of Minia University Hospital during the period of data collection and who were willing to participate in the study; and (3) female healthcare workers in both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital during the data collection period. Mothers who were not willing to participate in the study and not available during the period of data collection were excluded.
Description of the tool
Section I included items related to socioeconomic and demographic criteria of the participants.
Section II consisted of five items regarding Groups I–III but six items regarding Group IV; these items related to knowledge on early breastfeeding initiation. The total score possible was 11 in Groups I–III but 12 in Group IV.
Section III consisted of four items regarding Groups I–III but six items regarding Group IV. These items identified the attitude of participants toward early start of breastfeeding. This section used a 3-point Likert scale to assess attitude as strongly agree, agree, or don't agree. The total score possible was 8 in Groups I–III but 12 in Group IV.
Section IV consisted of four items regarding Group I, 7 in Groups II and III, but five items regarding Group IV. These items assessed practice related to early breastfeeding. The total score possible was 7 in Group I, 12 in Groups II and III, but 7 in Group IV.
In each section answers were scored in a range from 0 for wrong answers to 2 for correct ones.
Statistical analysis of data
The data obtained were entered after editing, coding, and grouping, tabulated, and transferred to a computer file. The data were analyzed according to the objective of the study by using the SPSS version 13 7 Windows program (SPSS, Inc., Chicago, IL), in which descriptive and inferential statistics had been done.
The χ2 test, Fisher's exact, t test, analysis of variance, and post hoc tests were used to find out the association between knowledge, attitude, and practice with selected variables. A value of p<0.05 was significant, and p<0.01 was highly significant.
Results
Sixty percent of women who initiated breastfeeding within 1 hour after labor were delivered by spontaneous vaginal delivery, while 50% of women delivered by cesarean section initiated breastfeeding within 2–6 hours after delivery (Table 1). Of women delivered by cesarean section, 83.3% used prelacteal feed in comparison with 40% of women delivered by spontaneous vaginal delivery (Fig. 1); this difference was statistically significant.
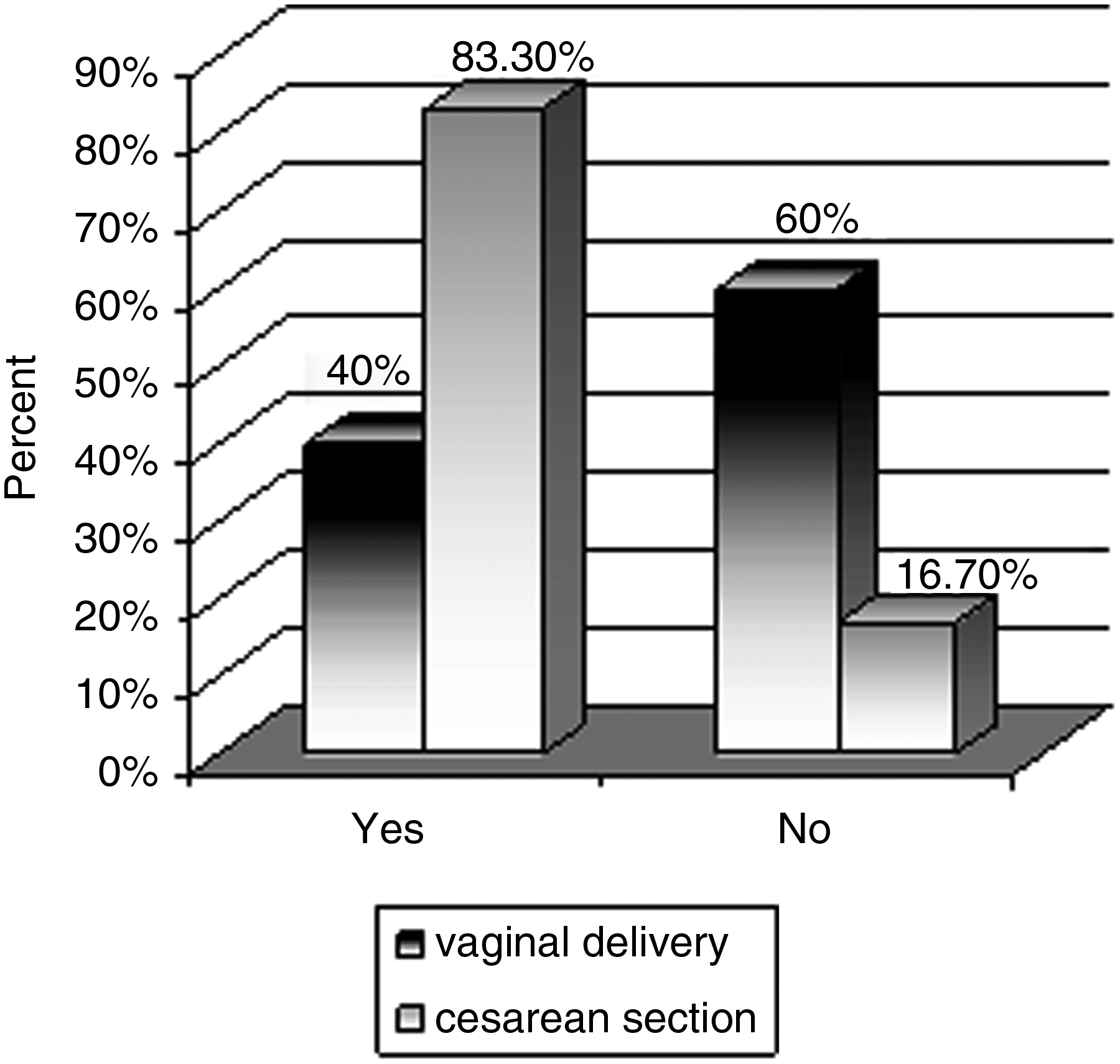
Use of prelacteal feed according to delivery type.
By χ2 test, χ2=13.6, p=0.001.
CS, cesarean section; SVD, spontaneous vaginal delivery.
There was a significant difference regarding practice and total score between women delivered by spontaneous vaginal delivery (Group I) and those delivered by cesarean section (Group II) (p=0.02 and p=0.04, respectively), but no significant statistical difference regarding knowledge and attitude (Fig. 2).
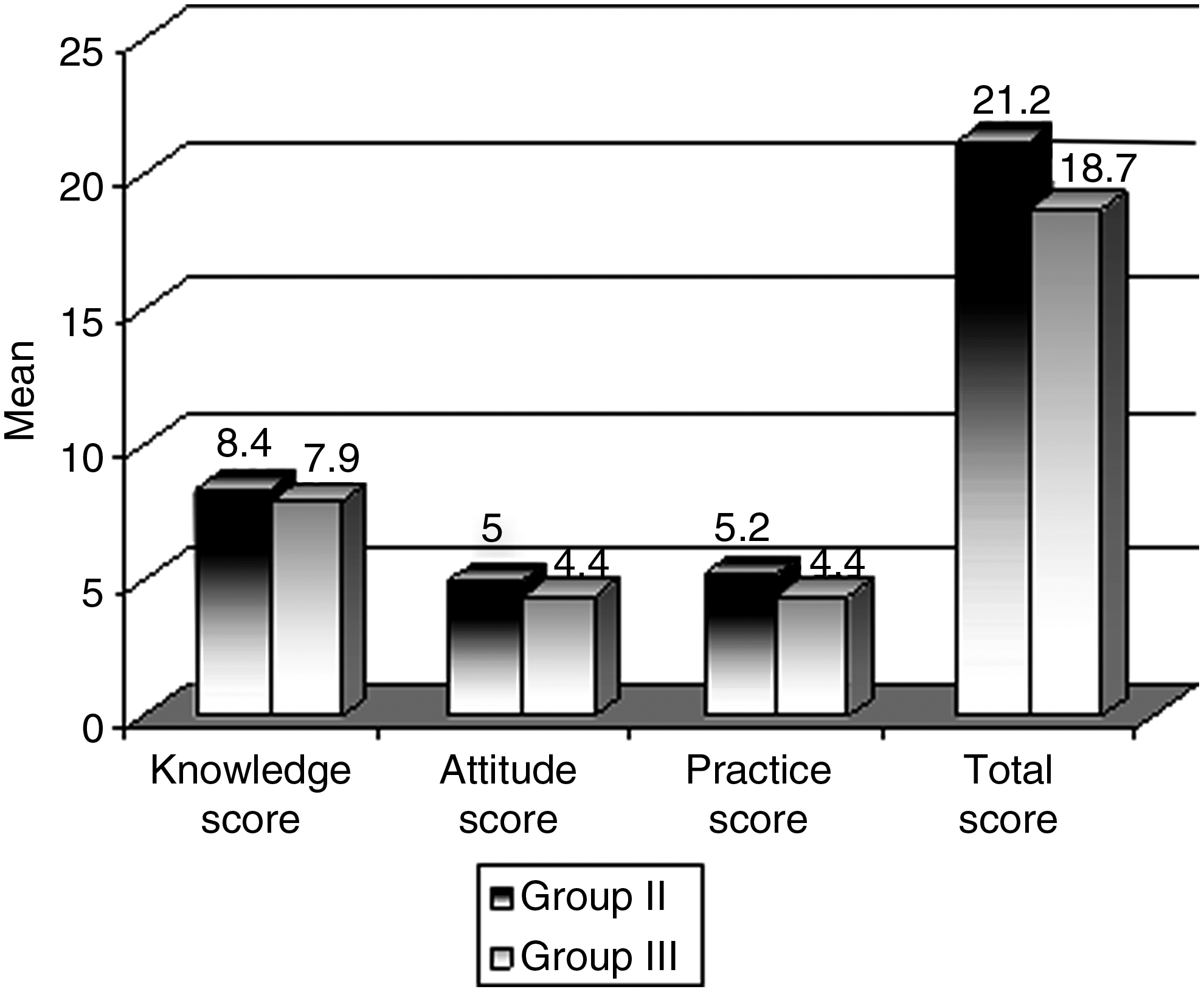
Comparison between Groups II and III regarding knowledge, attitude, and practice score.
The practice and total scores of nurses working in the Pediatrics Department were higher compared with nurses working in the Gynecology and Obstetrics Department (Table 2), and this difference was statistically significant (p=0.005).
Table 3 shows a statistically significant difference between Group I (pregnant women attending for antenatal care) and Group III (lactating women delivered by cesarean section) regarding knowledge score (p=0.0001). Also, the difference between Group I and Group IV (healthcare workers), that between Group II (lactating women delivered by spontaneous vaginal delivery) and Group IV, and that between Group III and Group IV regarding knowledge and attitude score were statistically significant.
Significance was calculated by post hoc test.
Table 4 shows that the most important factors affecting the start of breastfeeding were maternal illness, followed by early skin-to-skin contact (as 86.7% of women delivered spontaneously had early skin-to-skin contact, and 60% of the same group initiated breastfeeding within 1 hour, whereas 40% of women delivered by cesarean section had skin-to-skin contact with their babies, and as a result only 16.7% of them had early initiation of breastfeeding).
Dependent variable is the start of breastfeeding.
R2=0.6.
Discussion
Initiating breastfeeding within 1 hour of birth was one of the 10 Steps to Successful Breastfeeding on which the Baby-Friendly Hospital Initiative was based and launched in 1992. Step 4 was “Help mothers initiate breastfeeding within one half-hour of birth.” Its explanation, as provided by the World Health Organization, 8 is as follows:
Mothers in the maternity ward who have had normal vaginal deliveries should confirm that within a half-hour of birth they were given their babies to hold with skin contact, for at least 30 minutes, and offered help by a staff member to initiate breastfeeding.. At least 50% of mothers who have had caesarean deliveries should confirm that within a half-hour of being able to respond, they were given their babies to hold with skin contact.
In the present study it was found that 90% of pregnant women, 83.3% of the mothers delivered by vaginal delivery, and 93.3% of mothers delivered by cesarean section were aware of the importance of colostrum and breastfeeding. These findings were consistent with previous studies9–11 in which 76.7% of the mothers were aware of the importance of colostrum and breastfeeding.
Community strategies to promote the early initiation of breastfeeding should target not only mothers but also those who influence behavior such as grandmothers and other female relatives. In the present study 36.7% of pregnant women attending for antenatal care, 40% of women delivered by vaginal delivery, and 43.3% of those delivered by cesarean section received information about the early start of breastfeeding from their relatives. This consistent with a study conducted by Tawiah-Agyemong et al., 3 which reported that grandmothers and other female relatives were important influences as to advice to first-time mothers, because breastfeeding behaviors are learned from them and because these influencers often had control over the baby in the first few hours of life.
In the present study we found that 60% of those delivered by vaginal delivery initiated breastfeeding within an hour after delivery (World Health Organization rate of good). 12 This was consistent with the result obtained by Orün et al., 5 who demonstrated that the percentage of breastfeeding initiation in women delivered by vaginal delivery was 51.2% in the first hour but 81.4% in the second hour after delivery. In contrast, a study conducted by Boccolini et al. 13 in Rio de Janeiro between 1999 and 2001 found that only 22.4% of babies born through vaginal delivery were breastfed within the first hour after birth.
In the present study we found that one of the major factors for delaying the first breastfeed was delivery by cesarean section: only 16.7% of the mothers delivered by cesarean section initiated breastfeeding within 30 minutes to an hour after recovery from anesthesia, whereas 50% started to breastfeed their babies after 2–6 hours from delivery. This is near to the results obtained by Orün et al., 5 who reported that the percentage of breastfeeding initiation in women delivered by cesarean section was 18.9% in the first hour but 64% in the second hour after delivery. Several studies had confirmed that cesarean section is a significant barrier that inhibits breastfeeding within the first hour of life.13,14
In the present study we found a significant association between skin-to-skin contact and early breastfeeding initiation, and this is in agreement with a study conducted by Mikiel-Kostyra et al., 15 who stated that the first breastfeeding within 2 hours was significantly associated with skin-to-skin contact.
As expected, in the present study preterm newborns were less often breastfed within the first hour of life than those born at full term. This is consistent with a study in Japan conducted by Nakao et al. 16 and another in Massachusetts conducted by Merewood et al. 17 They reported that premature newborns were less likely to receive maternal milk.16,17 This result may be explained by coincident common problems, such as limited oral-motor skills, hypoglycemia, maternal adaptation to having a small infant, and delayed lactogenesis in premature infants. 18
According to the literature to date, several studies have investigated maternal age, educational level, and employment status for their impact on breastfeeding behavior.19–23 However, none of these factors was shown to influence early breastfeeding initiation in our study. Similarly, Orün et al. 5 revealed that there was no influence of maternal age, educational level, and work status on early breastfeeding initiation.
In the present study it was found that healthcare workers at Minia University Hospital had good knowledge about importance of early breastfeeding initiation, as 96.7% were aware of the benefits of colostrum and 93.3% of them had a positive attitude regarding early breastfeeding initiation being right for each baby. This was in consistent with a study conducted by Tawiah-Agyemong et al., 3 which demonstrated that despite the problem reported around the dissemination of breastfeeding information and materials and the focus of policy on exclusive breastfeeding, health workers' knowledge of the importance of early initiation was high.
Although Minia University Hospital was designated as a Baby-Friendly Hospital in the past, nowadays the Baby-Friendly Hospital Initiative policies are not actually activated, as 100% of healthcare workers in both the Pediatrics and Gynecology and Obstetrics Departments had a negative attitude about the role and encouragement of the Hospital regarding early initiation of breastfeeding. The most common reasons for this problem were attributed to a lack of communication between the Pediatrics and Gynecology and Obstetrics Departments and regular training programs about early breastfeeding initiation in the Hospital.
Conclusions and Recommendations
Although knowledge about early breastfeeding initiation was expressed by the majority of mothers participating in this study, actual application of this practice was clearly deficient.
In our study, the most important prenatal and postnatal factors associated with delayed breastfeeding initiation were determined to be maternal anemia, maternal illness during pregnancy, cesarean section delivery, and premature birth. Therefore, effective antenatal care to prevent and appropriately treat maternal anemia and illness and decrease cesarean section deliveries and premature birth will contribute to early breastfeeding initiation.
This study shows that there is a need for activating the Baby-Friendly Hospital Initiative policies in both the Pediatrics and Gynecology and Obstetrics Departments of Minia University Hospital and to ensure that all healthcare workers present at deliveries are skilled in supporting mothers in breastfeeding initiation and they have the materials they need.
In addition, we recommend the need to ensure sustainability of Baby-Friendly practices by periodic assessment and reassessments and by installation of monitoring systems inside the Hospital for checking and improving the Baby-Friendly policies. Finally, empowering parents and families to demand for their rights to Baby- and Mother-Friendly practices is core to changing hospital practices.
Footnotes
Acknowledgments
We would like to acknowledge all mothers who agreed to participate in our study and gave us their times and efforts to understand and answer our questions.
Disclosure Statement
No competing financial interests exist.