
Abstract
Abstract
The objectives of this study were to provide an economic assessment as well as a calculated projection of the costs that typical U.S. tertiary-care hospitals would incur through policy reconfiguration and implementation to achieve the UNICEF/World Health Organization Baby-Friendly® Hospital designation and to examine the associated challenges and benefits of becoming a Baby-Friendly Hospital. We analyzed hospital resource utilization, focusing on formula use and staffing profiles at one U.S. urban tertiary-care teaching hospital, as well as conducted an online survey and telephone interviews with a selection of Baby-Friendly Hospitals to obtain their perspective on costs, challenges, and benefits. Findings indicate that added costs for a new Baby-Friendly Hospital will approximate $148 per birth, but these costs sharply decrease over time as breastfeeding rates increase in a Baby-Friendly environment.
Introduction
The Baby-Friendly Hospital Initiative supports the International Code on the Marketing of Breast-milk Substitutes (“WHO Code”). The WHO Code stipulates that healthcare facilities and professionals neither accept nor offer free or low-cost substitutes for human milk. 8 Forgoing the acceptance of donated or heavily discounted formula and related supplies from manufacturers and vendors can create a significant impediment to becoming Baby-Friendly. Because these products are no longer free to the hospital pursuing a Baby-Friendly designation, they must be procured at wholesale costs. Despite being largely undefined, these costs are often cited as the greatest obstacle to implementing Baby-Friendly programs. 11 The costs of providing formula are particularly concerning for administrators of large urban academic medical center hospitals serving predominantly indigent and minority populations because exclusive breastfeeding rates among minorities and low-income families are significantly lower than those found among white women of higher socioeconomic status. 12 In addition, the Baby-Friendly designation necessitates multiple transition stages in order to become fully implemented, 11 requiring a hospital to invest or redirect limited resources, such as personnel time, information technology, and financial capital. No detailed information on costs of pursuing and achieving Baby-Friendly designation exists. An economic analysis of breastfeeding was recently reported that approached the issue through emphasis on the significant financial burden that suboptimal breastfeeding rates in the United States posed on society due to pediatric morbidity and mortality that would have been obviated by greater breastfeeding prevalence. 12 The published literature on the economics of pursuing Baby-Friendly designation in the United States comprises only a brief case study of one hospital's Baby-Friendly transition process and other limited and anecdotal evidence. 10 Sound economic data would provide another perspective for hospital administrators and financial officers as well as nursery service and obstetric care practitioners to view the direct and immediate economic impact of achieving the Baby-Friendly designation. The purpose of this study was to provide a financial analysis of the potential costs one index hospital would incur through undertaking the process to become a Baby-Friendly Hospital, as well as to document other challenges and benefits reported by extant Baby-Friendly Hospitals.
Materials and Methods
Cost analysis
Through survey and interview of key nursery management personnel at a single large, southwestern U.S., metropolitan health district and academically associated hospital that was not engaged in obtaining the Baby-Friendly designation, various data about neonatal feeding resources utilization were collected, and a cost analysis was conducted. This study was reviewed and approved by the University of Texas Institutional Review Board.
The index case hospital was selected by convenience of location and ability to serve as a proxy for similar-sized hospitals with about 2,800 births per year. The study involved quantifying and analyzing usage and costs of neonatal feeding supplies (e.g., infant formula, bottles, nipples) and associated staff labor. Initial Baby-Friendly implementation costs, such as programmatic application fees and staff training, as well as ongoing and recurring Baby-Friendly maintenance costs, including annual redesignation fees, material, supplies, training, additional staffing, and organizational changes, were included in the analysis. Costs were established for a range of peripartum case scenarios to account for potential variances in birth-related factors (e.g., term, cesarean, etc.), so that cost projections could be made. For each scenario, best case (A), moderate (B), and worst case (C) “economic cost vignettes” were projected. The approach used considered cost from the “provider perspective,” meaning it detailed the economic impact at only the organizational level and not the patient or society level. Supply costs were evaluated at average wholesale hospital pricing in order to represent standard group-purchasing discounts. Most large hospitals do not pay retail pricing because of large purchasing volume discounts. Typical wholesale or hospital discounts for hospital group purchasing organizations are between 15% and 30% for this size organization. These two discount end points (15% and 30%) were included in the model in order to reflect representative cost structures.
Underpinning our cost calculations were several key assumptions. First, we chose our index hospital with 2,800 deliveries annually and assumed its costs would be representative of similar U.S. hospitals. To calculate expected infant feeding supply and staffing costs, we used 5% as the average percentage of births expected to have complications that would entail greater feeding costs than would normal breastfeeding. We assumed that an additional 10% of babies would be preterm who may not be able to breastfeed exclusively and would require human milk fortifiers and possibly preterm formula. We then assumed that the remainder of births would be composed of normal term vaginal births (65%) and term births by cesarean section (20%). Based on these distributions, we projected that between 85% to 90% of babies born at any given time in our index hospital should be able to breastfeed.
To obtain cost for birth type (term and preterm), market-value supply costs of specific products as shown in Table 1 were collected from the hospital supply list. We estimated costs at wholesale value based on the average cost of formula(s), as well as at a full or 30% discounted value.
Three scenarios representing the hospital's total formula costs were created with the Case C or worst-case cost scenario depicting expenses if the hospital was to pay full wholesale formula prices. The “moderate” and “best” case scenarios (Case B and A, respectively) estimate formula costs if the hospital obtained a 15% or a 30% discount, respectively, from wholesale formula costs, which is common and based on the size of recurring bulk orders.
Survey
A brief 10-question survey instrument was designed and utilized with Baby-Friendly designated hospitals to obtain their perspective on costs incurred and benefits achieved. (The survey instrument is available upon request for the corresponding author.) From the group of 62 Baby-Friendly Hospitals listed on the Baby-Friendly USA Web site in 2009, a randomly selected sample of 40 U.S. Baby-Friendly hospitals was contacted by one of the study researchers, and 20 Baby-Friendly Hospitals (50%) agreed to participate in our e-mail survey. E-mail contact information for a key nursery service nurse administrator was obtained from these 20 Baby-Friendly sites, and the 10-item electronic Baby-Friendly survey instrument was sent to this designated contact at each site. Eighteen (90%) of the online surveys were completed. In addition, telephone interviews were conducted with these same administrators in order to maximize the richness of the qualitative description of the Baby-Friendly implementation process. (The telephone survey questions are also available by request from the corresponding author.) Of the 20 Baby-Friendly Hospital nursery administrators originally asked to participate in the online survey, 12 agreed to undergo the supplemental and more extensive telephone interview. All 12 were among those who had already completed the online survey. These semistructured interviews used scripted open-ended questions, designed to capture what administrative leadership personnel perceived to be the significant benefits and challenges of implementing a Baby-Friendly program. The survey was used to inform our cost estimation calculations.
Results and Rationale
Cost estimation of becoming Baby-Friendly
The five separate cost components analyzed were for the costs related to the (1) Baby-Friendly program application and certification process, (2) formula and related supplies, (3) organizational training, (4) personnel and staffing, and (5) the organizational structuring and process.
Baby-Friendly Hospital program application and start-up costs
To become a Baby-Friendly Hospital, hospitals must go through a four-step process, the 4Ds: Discovery, Development, Dissemination, and Designation. There is a $3,000 fee for each of the last three phases (or $2,200 for each phase for hospitals with fewer than 500 births per year). 13 Additional expenses of $1,500 were included in the total start-up costs to cover the travel, lodging, and per diem for two site assessors who conduct the Baby-Friendly final designation assessment procedures and certify that the Baby-Friendly Ten Steps requirements have been met. Once the Baby-Friendly designation has been obtained, there is an annual fee of $1,000 (U.S.) to maintain Baby-Friendly status. The Baby-Friendly Ten Steps include a requirement that hospitals devote time to developing and implementing policies and procedures for the new Baby-Friendly program (unless these policies are already in place) and provide education for patients regarding the importance of breastfeeding. These costs were estimated to be $1,700 for in-house development of educational materials, including brochure printing and distribution to patients. Policy and procedure development was estimated to include an indirect cost derived from 40 hours of development time at $25/hour of lactation consultant (LC) time, or $1,500. In total, initial Baby-Friendly programmatic expenses were calculated at $13,700 for hospitals with more than 500 births per year and $11,300 for hospitals with fewer than 500 births per year. Recurring programmatic costs were projected to be $2,700 annually, which include $1,000 in Baby-Friendly redesignation fees and $1,700 for patient-education brochures, posters, and promotional materials.
Costs of materials and supplies
This category includes standard prepackaged bottles of ready-to-feed infant formula, disposable bottle nipples, and standard prepackaged bottles of sterile water for infants, which is by far the largest direct cost associated with Baby-Friendly certification. Costs of materials and supplies will vary considerably based on the number of mothers who initiate breastfeeding and the negotiated discount rate for supplies. To estimate these costs, we extrapolated expenses associated with the overall supply/order list provided by our index hospital. This approach provided an institutional cost estimate of formula (and related items, such as nipples), which includes premature and sick babies admitted to the neonatal intensive care unit, and a term birth-specific cost, which excludes neonatal intensive care unit babies.
Year 0 is the base year at a hospital with a 25% exclusive breastfeeding rate and 1,700 babies delivered vaginally each year, reflecting the birth rate and breastfeeding rate of our index hospital. Year 1 is the projected first year of full Baby-Friendly implementation (i.e., starting after hospital assessment demonstrates it met the criteria and earned the Baby-Friendly Hospital status), so we assume that the hospital will have achieved a 40% exclusive breastfeeding rate. By Year 5, the assumption is that the institution will have achieved an 80% exclusive breastfeeding rate upon hospital discharge. Our assumptions are consistent with previous research that shows Baby-Friendly Hospitals achieve an average exclusive breastfeeding rate of 78% 5 ; however, individual hospitals contributing to this average may achieve lower or higher exclusive breastfeeding rates.
There is a broad mix of necessary supply types, sizes, and stock-keeping units. Using the institutional data provided by the index hospital, nearly 2,600 cases of formula (with 48 units of formula per case) were consumed in 12 months, which was augmented by numerous other supplies. The estimated price for each product was obtained from manufacturer price lists, and expenses were calculated at $367,311 for the entire institution. The portion of expenses related to the premature babies was estimated at $265,513, showing that 72% of total costs were consumed by 10% of the births. Premature infant supply costs were determined by aggregating consumption of specific product types only used by premature babies. Table 2 presents these three cost projections for total formula expenses to the hospital.
Formula and supply costs were then estimated at different breastfeeding rates achieved over time. It is assumed that as the BFHI is implemented and maintained, the hospital's exclusive breastfeeding rate will increase over time, and the formula and supply costs will correspondingly decrease. The largest drops in cost are seen as the exclusive breastfeeding rate increases from 25% to 60%. This is because the amount of supplies needed (such as formula and artificial nipples) will drop dramatically, as will the associated costs. Costs will still decline after achieving a 60% breastfeeding rate, just not in large increments, because there will continue to be some babies who cannot breastfeed. This perpetuates corresponding formula and supply costs, while costs to maintain Baby-Friendly status (personnel, training, materials, and program costs) also continue. This scenario, shown in Figure 1, depicts formula and supply estimates at wholesale price and at 15% and 30% discounts.
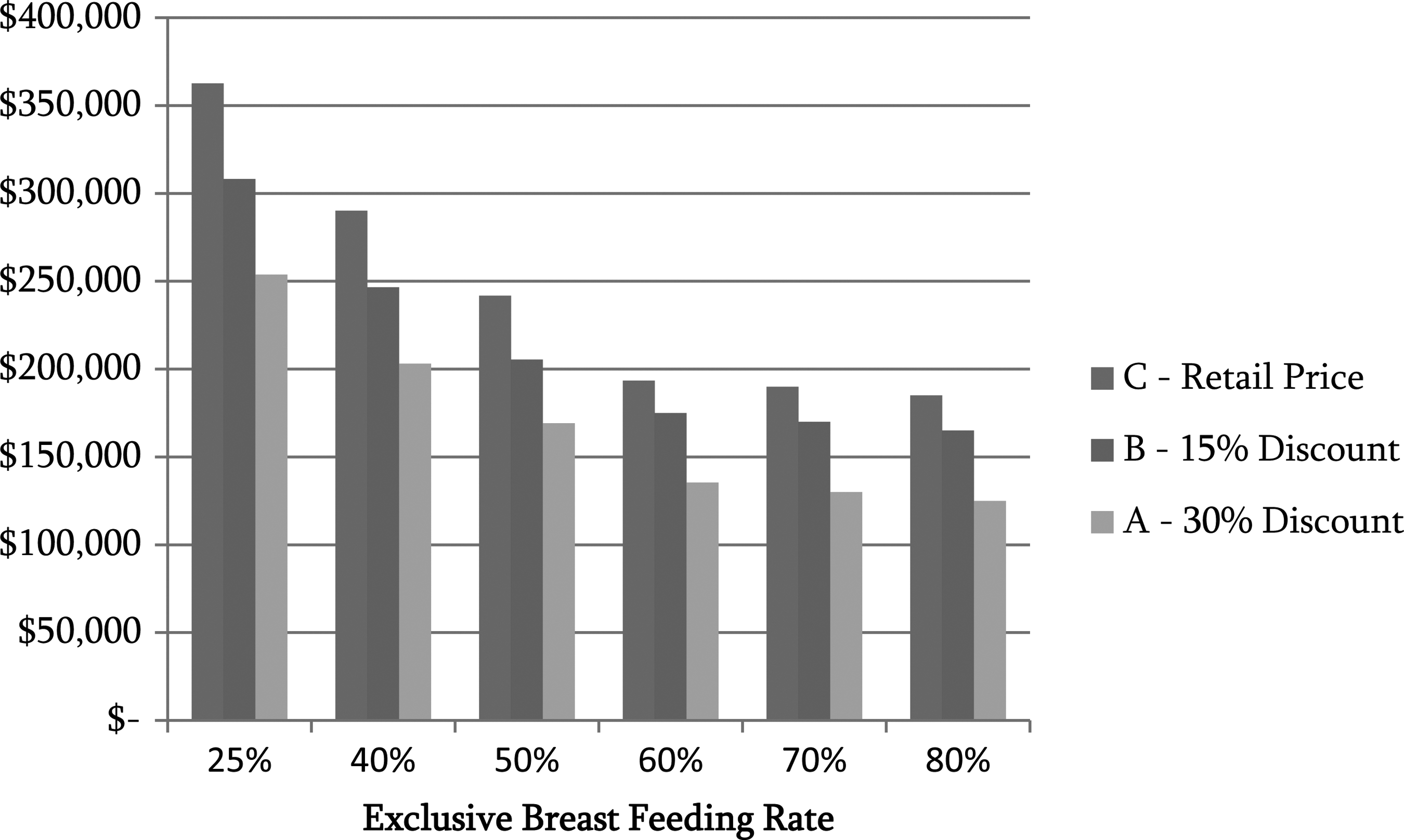
Average cost of formula and supplies decline as exclusive breastfeeding increases.
Organizational training costs
As part of becoming Baby-Friendly, nursing staff must be provided with 20 hours of training on the advantages and management of breastfeeding, inclusive of 5 hours of clinical competence verification. Our survey of several Baby-Friendly Hospitals revealed that there are a variety of training options at different costs. Most of the respondents reported that training was viewed as an indirect expense because nurses are already required to complete 24 hours of continuing education units per year. Several Baby-Friendly Hospitals reported shifting their continuing education units training to include Baby-Friendly training and requiring nurses to complete a free online Baby-Friendly training provided by the University of Virginia. Based on our interviews with Baby-Friendly Hospitals, the most common scenario for Baby-Friendly Hospitals was that they purchased some training supplies and materials from Baby-Friendly USA and required employees to be trained using these materials. However, if hospital practices, policies, and educational materials currently meet the BFHI guidelines, then hospitals will not need to redevelop them. An LC would most likely present the materials at two training sessions (about 2 hours), but the bulk of the training would be completed using the shared materials. In this scenario, the first year costs involve 20 hours of training and include one-time direct costs of $330 for the purchase of Baby-Friendly training materials (two DVDs, four books, and one teaching pack). The estimated annual indirect cost is as follows: ($25/hour of LC time×40 hours of training)+(25 nurses×$25/hour of nursing time×20 hours of training)=$13,500. Estimated per hour rates for LCs and nurses include salary plus benefits.
Physicians are required to complete a minimum of 3 hours of training, but these costs were not included in this analysis because physicians are generally not hospital employees and thus not generating hospital expense. Additionally, physicians can use the same education and training materials purchased for the nurses and LCs, so additional material costs were not included related to physician training.
Cost of personnel/staffing capacity increases
Currently our index hospital has 1.5 LCs for 2,800 births and an exclusive breastfeeding rate of 25%. The hospitals we surveyed were much smaller, having an average of 1,700 births per year, but all had one LC. This equates to a staffing ratio of 1.22 hours of LC resources per birth. Our index hospital has approximately 1.11 hours of LC resource per birth. Published research reports that a hospital with 1,500 births and an 85% breastfeeding rate needs about 2.5 full-time LCs (which equals a ratio of 4.67 hours/birth). 14 Although it will take time to reach a breastfeeding rate of 85%, our index hospital should anticipate increasing LC staffing to accommodate the increase in breastfeeding rates, training requirements, startup time, and number of births. Initially, an additional 0.5 full-time equivalent LC should be added because the index hospital is below the average staffing ratio (1.22 LC hours/birth) of the Baby-Friendly Hospitals interviewed, and having more LCs will promote expansion of the initial exclusive breastfeeding rate. This 0.5 full-time equivalent LC is estimated to cost $39,000 to cover $30,000 salary plus 30% fringe benefits. 15 As breastfeeding rates increase to 85%, the hospital should plan to add as many as five full-time LCs to provide a total of 6.5 LCs and a ratio of 4.67 hours/birth.
Organizational process change costs
The two main sources of organizational process change costs relate to structural facility or process changes and to organizational leadership resources invested to move the organization toward Baby-Friendly status. Our index hospital is currently not optimally designed for “rooming in” and is structured to create and maintain divisional lines between the nursery and peripartum personnel and routines. These two units are separated by a large space, as well as hierarchical authority structures. To implement a Baby-Friendly program successfully, the space should be reconfigured, facilities should be updated, and the hierarchical reporting structure should be revised to create a more cohesive unit and patient-centered experience. Nonetheless, assessment of the current index hospital's postpartum-nursery unit patient rooms provided evidence that even without needed reconfiguration, both mother and child could be accommodated comfortably. This indicates that hospitals, although needing to invest in facilities' modifications in the long term, may not need to do so as an initial expense.
There is a cost, albeit indirect, of “sponsoring” or championing the Baby-Friendly effort during the multiyear process. Although it might not require new personnel, existing management must be sufficiently committed to the Baby-Friendly project to invest time convincing the leadership about the benefits and potential while shepherding the process forward. It is anticipated that additional management time would be needed to manage the change process necessary to become and maintain designated Baby-Friendly. Based on labor market salary data, estimated costs were 10% effort for one middle/senior manager, at $75,000 annual salary and 30% benefits for 3 years. 16 This equates to $9,750/year of indirect expense for the first 3 years.
Table 3 lists a summary of all the estimated costs associated with becoming Baby-Friendly, assuming the index hospital receives a 15% discount from wholesale pricing of formula and supplies.
This number applies to hospitals with greater than 500 births per year. For hospitals with fewer than 500 births per year, one-time costs will be $2,400 less.
D, direct; FTE, full-time equivalent; I, indirect; LC, lactation consultant.
Limitations
There are several limitations inherent in this research. To estimate costs, we needed to make certain assumptions; however, it is unknown the extent to which these assumptions and costs can be generalized to other hospitals. Other hospitals may have more or less success achieving exclusive breastfeeding rates. Other hospitals may have existing policies, procedures, or personnel that would facilitate change and lower costs or pose barriers and greater costs. Additionally, Baby-Friendly USA recommends that facilities not tackle the purchasing of formula until the Ten Steps have been established. Our cost projections of formula-related expense may be high because we calculated costs based on amount of formula on hand prior to implementing the Ten Steps, which thus corresponds to peak formula use and related expense. Hospital patient populations may also vary tremendously, with some populations being more or even less receptive to exclusive breastfeeding. Additionally, we interviewed key nursery administrators at Baby-Friendly Hospitals to help inform this research, but we did not gather the opinions of hospital management about becoming Baby-Friendly. Although some hospital administrators may consider these costs minimal, other hospital administrators may consider these costs too high to pursue and maintain Baby-Friendly designation. Additionally, there is also the potential for selection bias in our survey because only 50% of the invited hospitals participated in the online survey. It is possible that non-respondent Baby-Friendly Hospitals had different costs or experiences with the Baby-Friendly designation process.
Discussion
Baby-Friendly implementation in a U.S. hospital may initially increase costs per birth, but this study demonstrates that these costs should be expected to decrease over time. Because the main factor driving increased costs is the quantity of infant formula and associated supplies that must be purchased, it follows that increasing rates of exclusive breastfeeding would correspondingly result in decreasing formula and supply expenditures and an overall decrement in the costs to maintain Baby-Friendly status. Following Baby-Friendly designation, supply costs were estimated to decrease across all birth types as higher exclusive breastfeeding rates are sustained. Although this study documents the incremental costs of becoming Baby-Friendly for one case study, hospitals considering implementing the Baby-Friendly Hospital program can use this structured costing approach to estimate their specific cost projections over time.
Our cost model did not include any organizational or structural line items related to gaining key leader “buy-in” or reorganizing departments, but these costs are real. Facility redesign, construction, or repurposing may also be necessary in order to accommodate expanded-purpose birthing/maternity rooms, rather than maintaining separate obstetric and nursing areas. In addition, programmatic costs and other hurdles must be budgeted, so that key institutional leaders and Baby-Friendly “champions” can guide and support the program through its birth and development into a complete and successful Baby-Friendly program and facility. U.S. hospitals should recognize that Baby-Friendly implementation is often most challenging for nurses because of the many organizational, cultural, and behavioral changes required of them in both the obstetric and neonatal care settings. Special attention, education, and communication should be targeted to optimizing nursing staff education and ongoing support in the labor and delivery areas as well as throughout all other related clinical units.
Becoming Baby-Friendly requires some amount of philosophical “culture” change on all levels of personnel, but particularly in key management personnel in order to pursue and sustain Baby-Friendly status. Overall, the phone interviews revealed a generally positive response about becoming a Baby-Friendly Hospital. Our fieldwork indicates that Baby-Friendly Hospitals are pleased with their decision, working to maintain Baby-Friendly status, and convinced that the improved outcomes offset any incremental costs. Because the managers interviewed did not have a detailed understanding of the costs involved, their positive opinion that the improved outcomes offset the incremental costs was not based on the actual economic detail.
It is well recognized that initiating and supporting breastfeeding in the immediate postpartum period is critical to success in breastfeeding initiation, continuation, and exclusivity. Feeding formula in the hospital or providing discharge packs with formula and commercially labeled related products to the mother while trying to establish breastfeeding is highly associated with lower rates of any breastfeeding and/or exclusive breastfeeding.17,18 Promoting exclusive breastfeeding while at the hospital or birthing facility is the major factor known to increase rates of both breastfeeding initiation and sustained breastfeeding. Successful breastfeeding of 90% of U.S. newborns could lead to an annual $13 billion in health savings and the potential prevention of over 911 deaths annually. 12 Despite the hospital-specific variability in costs of becoming Baby-Friendly, clinicians and other hospital or birthing center leadership considering Baby-Friendly implementation can utilize our study methods to build cost models applicable to their own facilities and thus understand and anticipate their own costs to achieve Baby-Friendly success.
Footnotes
Acknowledgments
This study was supported through contract funding from the Maternal and Child Health Services Division of the Texas Department of State Health Services.
Disclosure Statement
No competing financial interests exist.