
Abstract
Abstract
Background:
The World Health Organization (WHO)/UNICEF Baby-Friendly Hospital Initiative (BFHI) was developed to support the implementation of the Ten Steps for Successful Breastfeeding. The purpose of this study is to assess trends in the numbers facilities ever-designated “Baby-Friendly,” to consider uptake of the new WHO/UNICEF BFHI materials, and to consider implications for future breastfeeding support.
Materials and Methods:
The national contacts from the 2006–2007 UNICEF BFHI update were recontacted, as were WHO and UNICEF officers worldwide, to ascertain the number of hospitals ever-designated “Baby-Friendly,” presence of a government breastfeeding oversight committee, use of the new BFHI materials and, if yes, use of the new maternity or human immunodeficiency virus (HIV) materials.
Results:
Seventy countries reporting in 2010–2011 and the updates from an additional 61 reporting in 2006–2007 (n=131, or 66% of the 198 countries) confirm that there are at least 21,328 ever-designated facilities. This is 27.5% of maternities worldwide: 8.5% of those in industrialized countries and 31% in less developed settings. In 2010, government committees were reported by 18 countries, and 34 reported using the new BFHI materials: 14 reported using the maternity care and 11 reported using the HIV materials.
Conclusions:
Rates of increase in the number of ever-certified “Baby-Friendly” hospitals vary by region and show some chronological correlation with trends in breastfeeding rates. Although it is not possible to attribute this increase to the BFHI alone, there is ongoing interest in Ten Steps implementation and in BFHI. The continued growth may reflect the dedication of ministries of health and national BFHI groups, as well as increasing recognition that the Ten Steps are effective quality improvement practices that increase breastfeeding and synergize with community interventions and other program efforts. With renewed interest in maternal/neonatal health, revitalization of support for Ten Steps and their effective institutionalization in maternity practices should be considered. Future updates are planned to assess ongoing progress and impact, and ongoing updates from national committees are welcome.
Background
The BFHI was designed to encourage and monitor global progress on the Ten Steps by offering more than the Ten Steps alone; BFHI materials include guidance for planning national programs, training of hospital clinical staff and administrators, self-appraisal forms, and facility designation in recognition of the facility's implementation of the Ten Steps among other additional materials. To receive this designation, internal and external review and assessment processes must reflect a defined minimal level of achievement. UNICEF has monitored the number of the BFHI-designated hospitals over the years 2 and more recently as part of a broader effort to assess the scope and scale of all infant and young child feeding interventions in developing countries. 3
The positive health and emotional sequelae of breastfeeding for the mother as well as the child are better understood today. In addition to child health and survival, these include improved recovery following delivery, decreased blood loss postpartum, delayed return to fertility, and decreased risk of breast and ovarian cancers. The “Baby-Friendly” approach supports immediate postpartum breastfeeding, helping the bonding between mother and child as well as conveying all the known benefits of breastfeeding, including a reduction in cases of abandoned babies. 4
Therefore, the Ten Steps and BFHI would seem to remain as relevant in the new millennium as when they were first considered, given the increasing emphases on safe motherhood, maternal/newborn health, and comprehensive approaches including the community. In fact, the 2005 Innocenti+15 meeting, co-sponsored by UNICEF, WHO, World Alliance for Breastfeeding Action (WABA), and others, reviewed progress since 1990 and called for revitalization of the Ten Steps and for expansion beyond the hospital setting. 2 Innocenti+15 concluded, “Exclusive breastfeeding increased in many regions, even in the face of continued advertising of commercial infant foods and increasing HIV [human immunodeficiency virus] prevalence, possibly due to the BFHI alone or in combination with other efforts.” 2 According to the WABA, “The BFHI was clearly the right initiative at the right time. It galvanized numerous resources available globally and provided a focus and facilitated political will at the highest levels as never before.” 5
The challenges identified at Innocenti+152 included the following:
1. Commitment. Staff turnovers, the departure of BFHI supporters, or competing issues result in declining BFHI practices in some of the designated facilities.
2. Insufficient ownership by governments. The initiative was often seen as a UNICEF/WHO endeavor, rather than a national priority.
3. Compliance and quality control. Incorporation of BFHI criteria into general quality control and accreditation systems may be needed for sustainability.
4. Cost. There are some capital costs to change training and systems.
5. Community outreach. Step 10—community outreach—has not been actively implemented or maintained in many countries.
6. Confusion and concerns regarding HIV. The HIV/acquired immunodeficiency syndrome pandemic has been associated with confusion and concerns about breastfeeding and related “Baby-Friendly” activities.
7. Extending the continuum of care. Additional attention to maternity care and intrapartum care is needed.
8. Mainstreaming/integration. The principles of “Mother-“ and “Baby-Friendly” may also be integrated with other initiatives. To support the sustainability of Baby-Friendly Hospital practices, full integration of these practices into all ongoing activities in support of Millennium Development Goals 1 (Eradicate extreme poverty and hunger), 4 (Reduce child mortality), and 5 (Improve maternal health) is a way to ensure the maternal–newborn–child health continuum. Hence, all Ten Steps of BFHI are part of quality care of the newborn.
Notwithstanding these challenges, BFHI continued to be a central component of strengthening breastfeeding support and early initiation, as well as health-worker training. As suggested by the Innocenti+15 outcomes, UNICEF and WHO updated and revised the BFHI documents and commenced country piloting; The Baby-Friendly Hospital Initiative: Revised, Updated and Expanded for Integrated Care 6 was published in 2009. 7
The impact of the Ten Steps has been shown at the hospital level in many studies in recent years,8,9 and national-level impact has also been noted. 10 One analysis of global impact found a clear point of increase in exclusive breastfeeding with the implementation of the Ten Steps through BFHI. This analysis included only those countries for which multiple Demographic and Health Survey/Multiple Indicator Cluster Survey survey data are available and then adjusted all data to the year that the BFHI was initiated in each country. 11
The lines in Figure 1 indicate the rate of increase in exclusive breastfeeding (EBF) in infants <2 months and the rate for 0–6 months. There is an association between the increased rate of exclusive breastfeeding following implementation of BFHI, as indicated by the first report of a hospital achieving and being designated as fully practicing the Ten Steps. For the countries in this study, if the rate of increase in exclusive breastfeeding had continued to grow at the pre-BFHI rates, the percentage of exclusive breastfeeding would have been nearly 15% lower, closer to 25% rather than the 42% seen in these countries. 11

Impact of the initiation of the Baby-Friendly Hospital Initiative (BFHI) on the rate of increase in exclusive breastfeeding (EBF) in countries where both BFHI information and exclusive breastfeeding trend data are available. (With permission, from International Breastfeeding Journal). 11
The purpose of the current study is to update data on the number of facilities ever-designated “Baby-Friendly,” assess trends, explore the implementation of the revised and expanded BFHI worldwide, examine the relationship of this effort with global trends in exclusive breastfeeding, consider whether the acceptance of the new materials has influenced forward momentum, and discuss possible synergy with other programming.
Materials and Methods
UNICEF monitored the status of the BFHI, including recertification, from the early 1990s. At the request of the WABA and with UNICEF agreement and offering of contact information, the author e-mailed all available national BFHI contacts from the 2006–2007 UNICEF update, as well as current UNICEF regional officers and many country officers, and many personal contacts. Informants were asked to complete a brief survey that included number of hospitals ever-designated, presence of a government breastfeeding oversight committee, use of the new BFHI materials, and, if in use, whether the new maternity or HIV materials were in use. It is important to note that the status of “ever-designated” is not necessarily reflective of current practices; many hospitals do not maintain all practices, and some have reverted to earlier practices over the many years since the original designation. However, during the period of rapid increase, it is reasonable to assume that following the process of designation that the practices remained in place for a period of years.
All data from this survey were entered onto an Excel (Microsoft) spreadsheet, along with data gathered by UNICEF since the 1990s, in 1–4-year intervals. The data are reflective of the level of dedication to accurate reporting and are expected to have some unreported activity. Although not all countries reported on all data requested, for the purposes of global reporting, the data submitted are assumed to be reasonably accurate (see Discussion). Excel software was used to generate descriptive and trend data and graphs.
Additional data sources for breastfeeding rates and program activities used in analysis are cited in the text.
Ethical consideration: This study is considered exempt as it includes only program data with no personal identifiers. UNICEF personnel supported this effort with their time and review of early and final drafts of this paper; however, the author alone is responsible for the views expressed in this publication, and these views do not necessarily represent the opinion or policies of UNICEF, WHO, or any other organization.
Findings
Number of hospitals ever-designated
Updates were received from 70 countries in 2010–2011, and an additional 61 were updated in 2006, for a total of 131, or 66% of countries worldwide. In addition to updates, nearly all countries reported at some point during this period, with the remainder generally reporting no change. Table 1 shows the number and percent of respondents by region, development status, and total.
Percents may not add to totals due to rounding.
CEE/CIS, Central and Eastern Europe and the Commonwealth of Independent States; EAPRO, East Asia and the Pacific Region; ESARO, Eastern and Southern Africa; MENA, Middle East/North Africa; WCARO, West and Central Africa.
The number of hospitals ever-designated has increased; according to the most recent data, there are a reported 21,328 hospitals worldwide that have ever been designated. This represents about 27.5% of all maternities worldwide: about 8.5% of facilities in industrialized countries and about 31% in less developed settings.
Trends in reporting
The rates of response to the surveys have shifted over the years (Table 1). The rate of response from industrialized countries is higher (84% vs. 62% of developing countries). Central and Eastern Europe and the Commonwealth of Independent States—the newly independent states—and East Asia and the Pacific countries continue to have higher rates of response, whereas West and Central Africa, the South American/Caribbean nations, and the Middle East/North Africa region countries have declined to 39%, 46%, and 50%, respectively.
Government authority/committee and uptake of new materials
Only 18 of the 70 respondents in 2010–2011 reported an active government committee, and about half of all reporting (n=34) are beginning to use the new BFHI materials (Table 2). Of these, 14 reported using the new materials for maternity care, and 11—all in less developed settings—reported using the new HIV module (Table 2).
BFHI, Baby-Friendly Hospital Initiative; CEE/CIS, Central and Eastern Europe and the Commonwealth of Independent States; EAPRO, East Asia and the Pacific Region; ESARO, Eastern and Southern Africa; HIV, human immunodeficiency virus; MENA, Middle East/North Africa; WCARO, West and Central Africa.
Numbers, rates, and trends in BFHI and facilities ever-designated
The number of countries that have ever implemented BFHI has increased over the years. About 160 countries around the world have initiated BFHI, using the indicator as ever having designated a hospital; however, some of the 38 that have not as yet designated a hospital are, nonetheless, working towards this goal.
Table 3 includes the responses of UNICEF officers and country programs over the years as collected by UNICEF through 2006 and updated at the request of WABA for 2009–2011. The countries that responded in 2006 are bolded and those responding in 2010 are in italics.
Countries in bold reported in 2009–2010, and additional countries that reported in 2006–2007 are indicated by italics. Remainder of countries last reported changes in these data prior to 2006. Indonesia was an unofficial update in 2011 and hence is in bold italics.
CEE/CIS, Central and Eastern Europe and the Commonwealth of Independent States; MENA, Middle East/North Africa; OCT, Occupied Territory; WCARO, West and Central Africa.
Figure 2 shows the trend in total number of hospitals ever-designated. Please note this is not current status as many may have ceased compliance. There is an apparent slowing in the increase in the numbers ever-designated in about the year 2000. However, the rate appears to increase again within about 2–3 years. There is another apparent decline in the rate of increase in the last 3 years.

Total number of hospitals ever-designated “Baby-Friendly,” worldwide.
Figures 3 and 4 illustrate the percentages of hospitals ever-designated “Baby-friendly” for developing countries, industrialized countries, and total. The increase in the rate of designation appears to slow in many regions prior to and continuing after 2000, while the rate in industrialized countries picks up substantially a few years later, about 2004.
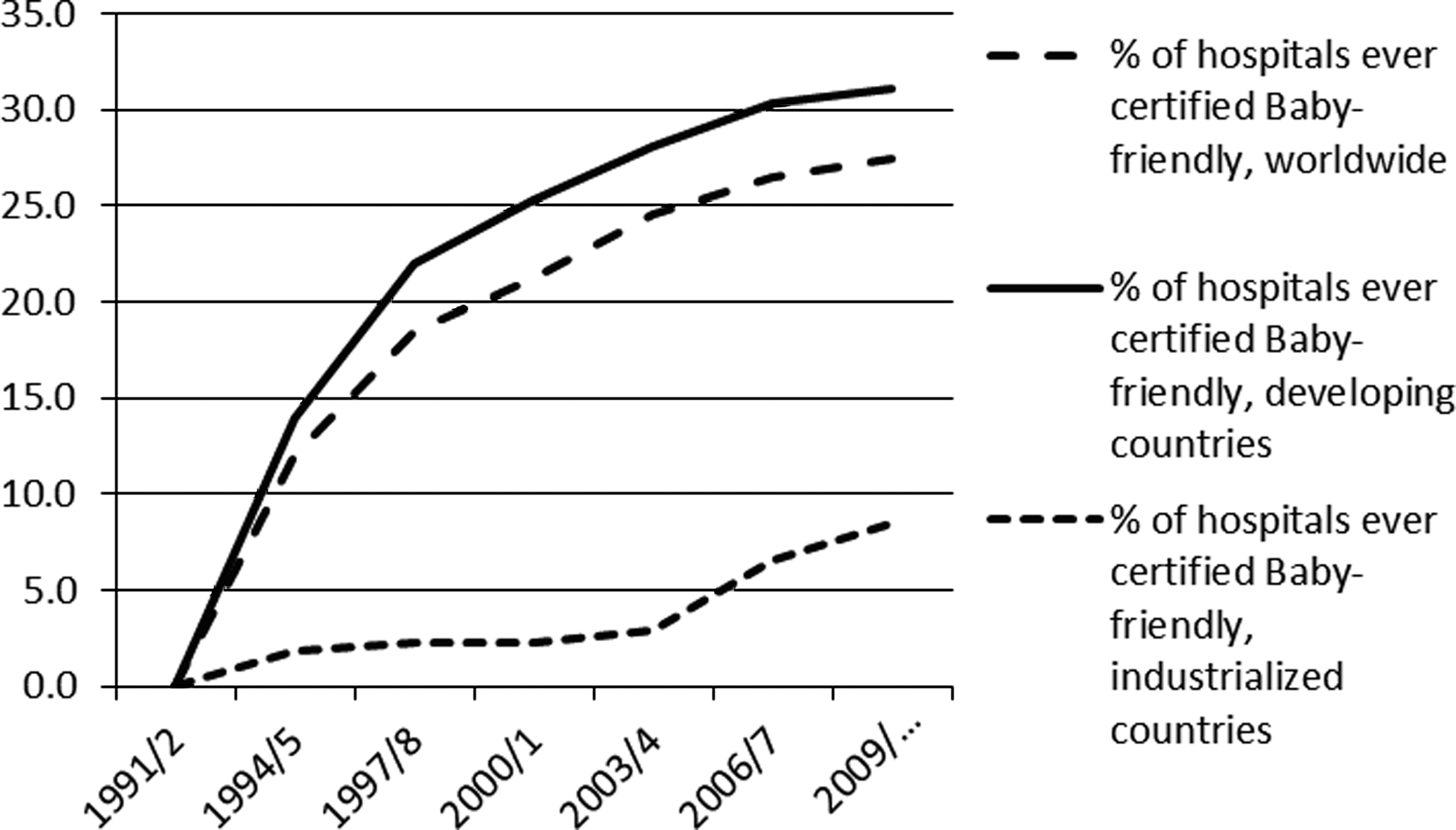
Percentage of hospitals ever-designated “Baby-Friendly,” by developing countries, industrialized countries, and worldwide.
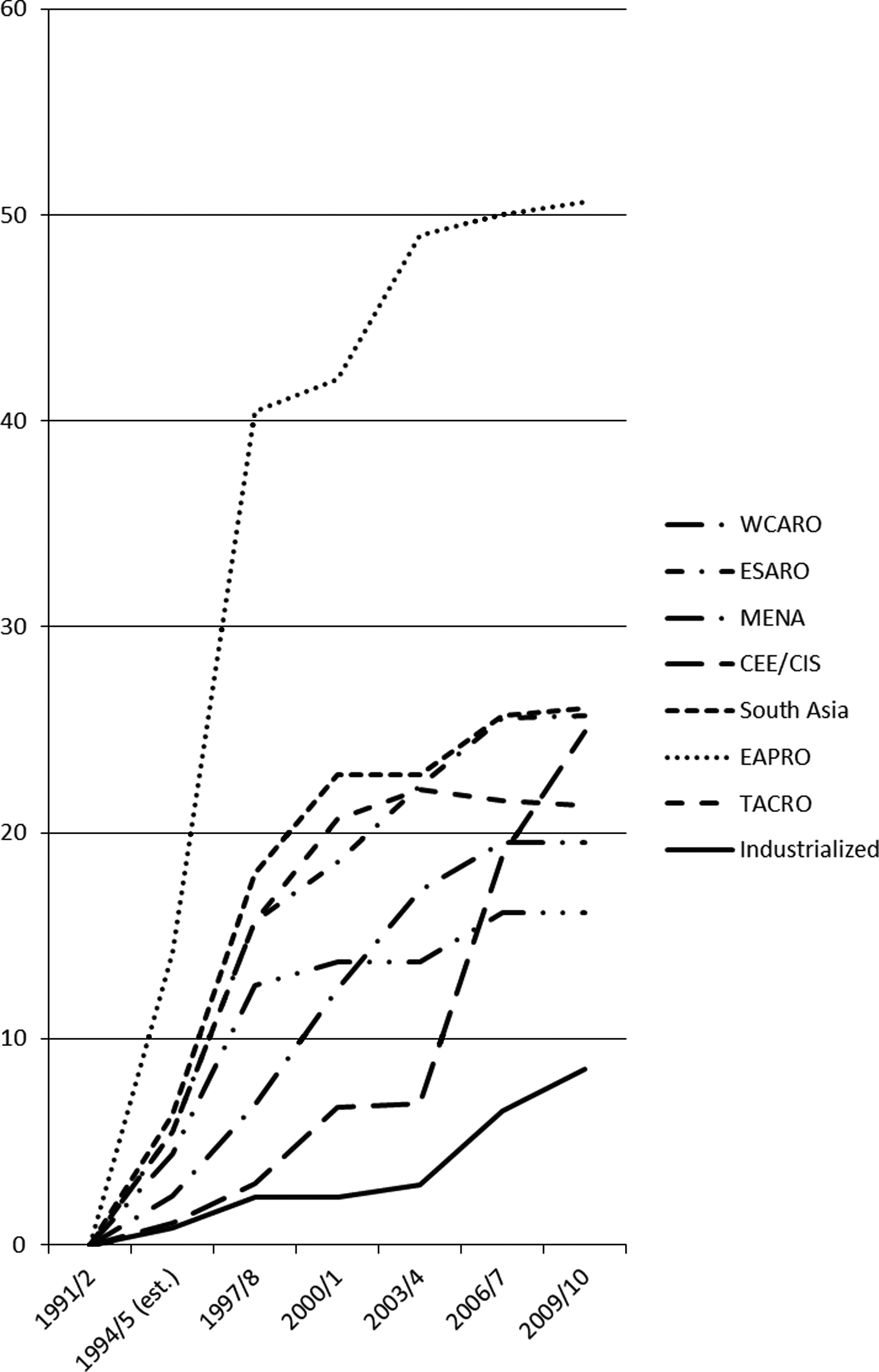
Percentage of hospitals ever-designated “Baby-Friendly” by region. Note that data for 1994–1995 were incomplete and were estimated. In the Americas and the Caribbean (TACRO), it appears that there is a decrease; this is due to the increase in total number of maternities reported in the region without a concomitant rate of increase in the number of hospital ever-designated as a Baby-Friendly Hospital. CEE/CIS, Central and Eastern Europe/Commonwealth of Independent States; EAPRO, East Asia and the Pacific; ESARO, Eastern and Southern Africa; MENA, Middle East/North Africa; WCARO, West and Central Africa.
Relationship with exclusive breastfeeding rates
The rates of exclusive breastfeeding appear to have increased worldwide since the Innocenti Declaration of 1990 (Figure 5, discussed below). The relationship between any single national program and measurable breastfeeding behavior change is difficult to measure because of the many other programs and social factors that may also influence exclusive breastfeeding rates. In order explore this general relationship, chronological association may provide some insights. The trends in percent of facilities ever-designated in each of the UNICEF regions are illustrated in Figure 4. As may be seen, not all regions have proceeded in parallel; some started up rapidly but then became relatively quiescent, whereas other exhibited later surges. It is notable that BFHI in industrialized settings and in the Central and Eastern Europe and the Commonwealth of Independent States seems to have taken off within the last 7 years or so.
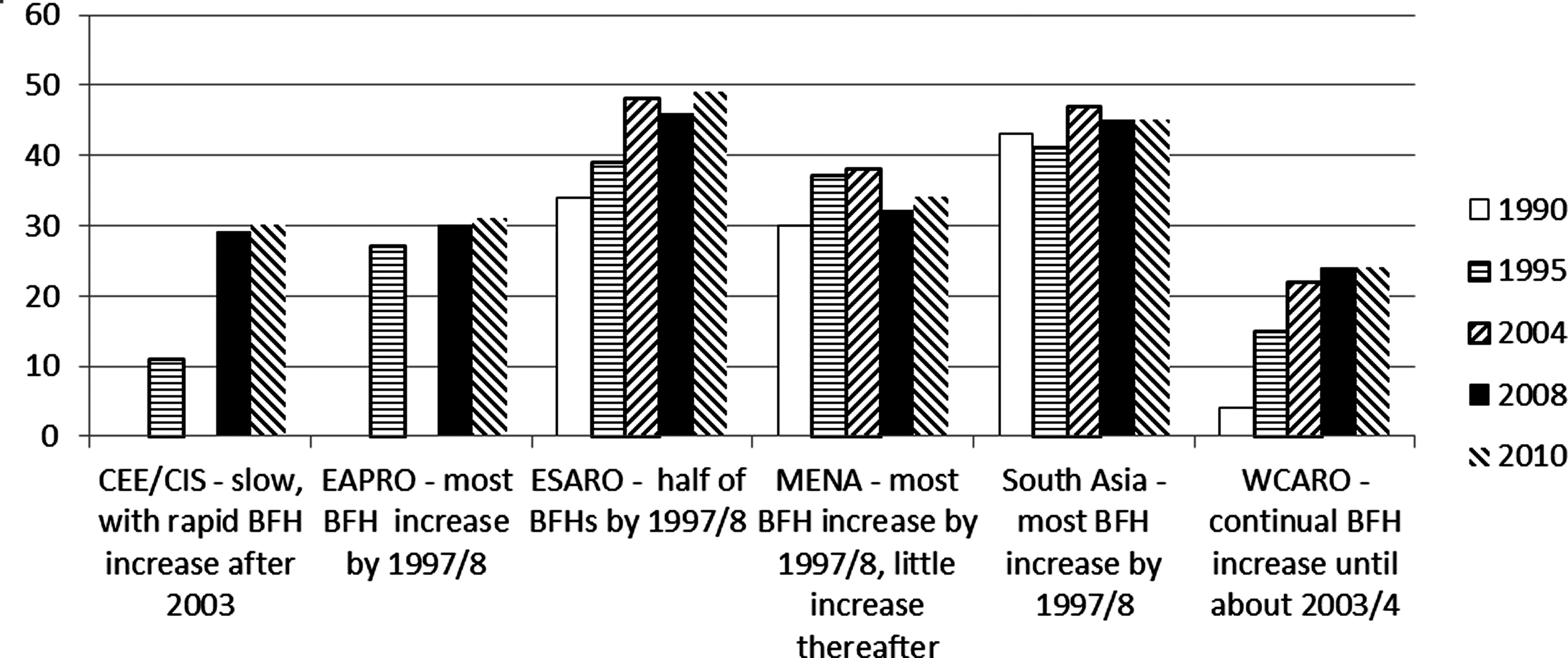
Percent of infants at all ages, from birth to 6 months of age, exclusively breastfeeding, from cross-sectional surveys. Labels summarize the pattern of BFHI growth, as seen in Figure 4. Note: The 1990 and 2004 estimates are not directly comparable with the 1995 and 2008 data nor the 2010 data as each published study (see sources below) included different subsets of countries (excludes China). In sum, these are point-in-time estimates that may not be entirely comparable, but may reflect trends. 1990, 2004: This Trend Analysis is based on a subset of 37 countries, covering 60% of the developing world's population.
Figure 5 presents available data on the percentage of exclusive breastfeeding among all infants 0–6 months of age, taken from several UNICEF-published and Childinfo.org available analyses. These analyses were not designed to be fully comparable and are presented for the purpose of general visualization of the relationship between timing of increases in BFHI programming and timing of surges in exclusive breastfeeding rates. For some regions, there appears to be chronological association. Eastern and Southern Africa and West and Central Africa exhibited a steady and continuing increase in Baby-Friendly Hospitals until about 2006, and the exclusive breastfeeding rates increased and then leveled, in parallel. Middle East/North Africa surged early in terms of increasing rates of BFHI, slowing rapidly after 1997; exclusive breastfeeding rates seem to have flattened or slowed.
Comparable breastfeeding data for exclusive breastfeeding rates over this two-decade time period are not available for industrialized countries, the Americas and Caribbean, or Central and Eastern Europe and the Commonwealth of Independent States.
Discussion
The continued growth in the number of facilities ever-designated as Baby-Friendly is testimony to the recognition that implementation of the Ten Steps is an effective quality improvement activity to increase breastfeeding and to the dedication of ministries of health and national breastfeeding. Although the rate of increase has declined in several regions, in some countries BFHI national committees and national programs, some with support from UNICEF and other partners, have preserved the effort. Regions have proceeded at different rates, which may be attributed, in part, to available funding and political will. From the data collected it would appear that the HIV module was not, as yet, being rapidly implemented globally. Revised WHO/UNICEF guidance may have call for updating; however, the maternity module would appear to have been implemented in many regions.
BFHI helped place breastfeeding on the health policy agenda of most countries worldwide. 2 Studies show the BFHI approach to be extremely effective. A review of the evidence for the Ten Steps conducted by WHO concluded that “the basic premise of the Baby-friendly Hospital Initiative, which requires all maternity facilities to implement the Ten Steps to Successful Breastfeeding, is valid” 12 and that exclusive breastfeeding will be most effectively increased and sustained when all the 10 Steps are pursued together. However, subsequent research has found that implementation of even some of the steps results in significantly improved exclusive breastfeeding outcomes.13,14 This new evidence may encourage consideration of Step-wise accreditation, so that all facilities, even those that do not wish to address all Ten Steps, may be stimulated to act.
Limitations and strengths
Program monitoring at the global scale can suffer from changing contacts, delayed responses, and reliance on volunteer reporting. As a result, it is recognized that the data provided are a reflection of the global status rather than an exact report. While the data herein are no exception to this, they are the only continuous global data available on this innovative initiative. A major limitation in this assessment of global status is the fact that reports of ever-designated facilities in the last decade are only available from 66% of countries, and this limits the conclusions on trends that can be made at the global level. In addition, the indicator of “ever-designated” does not reflect the current compliance of hospitals with the Ten Steps, so conclusions of impact cannot be inferred.
It is also important to note that this article only addresses the total of hospitals “ever” designated as Baby-Friendly, not the number currently practicing the Ten Steps. Therefore, it is important to emphasize the need for recertification and continuous monitoring of hospital practices. Unless hospitals are periodically recertified or, alternatively, that the Ten Steps are included in the standard quality assurance procedures for maternity facilities, the practices may gradually deteriorate, and, consequently, the support for optimal feeding may be reduced. In the current global situation, in which the marketing of breastmilk substitutes is so aggressive and reaches so many healthcare workers and hospitals, recertification remains a vital deterrent to interference with hospital practices.
Finally, to repeat, this article is not based on data collected for research purposes, nor can any definitive statement be made on statistical association. What is presented are chronological, ecological correlates, open to discussion and alternative interpretations.
The results in context
The published studies are consistent in the finding that implementation of the Ten Steps and the achievement of BFHI designation not only support the proper initiation of breastfeeding in the maternity setting, but also have continuing impact on duration of EBF. This may be due to impact on maternal physiology, but may also be due to synergy with community support. Where health professionals support breastfeeding, the possibility of disconnect with community efforts is reduced. For example, if even one child, having been hospitalized, returns to the village from the hospital having been taken off the breast, the message is effectively sent to all in that village that formula is what the health professionals consider better for health. Recent reviews of community programming support the positive results of this synergy. Two recently published reviews of community breastfeeding projects in developing county settings concluded that comprehensive programs that include both healthcare system and the community efforts are more effective than either alone.15,16 Considering the temporal relationship of these efforts, it is noted that the preexisting programs of health system support result in a noticeably greater impact when a community intervention is introduced. 16 An earlier study of the timing of introduction of BFHI and other breastfeeding support illustrated this temporal association as well. 17 This supports the contention that the preexistence of a supportive medical system, as is created by BFHI or other similar efforts, may be associated with increased impact of community efforts.
The purpose for and challenges to BFHI outlined at Innocenti+15 remain relevant. There is an ongoing need to develop and monitor provision of health worker education in breastfeeding support and skills, beyond that offered by the in-service BFHI course. However, given that many countries no longer report activities, there may be a need to address message fatigue 18 and create new innovative approaches. To this end, increased promulgation of the revised materials may help additional countries, their hospitals, and their associated training centers to consider and offer education in the skills necessary to implement the practices needed to support breastfeeding in a sustainable manner. Perhaps inclusion of the principles and tools of the BFHI into national standards for healthcare facility accreditation should be considered. This, in contrast with the previous vertical and, often, externally funded approach, may be essential for acceleration and sustainability of these important maternity care practices. With renewed interest in health systems strengthening maternal/neonatal health and community interventions, synergy with revitalization of support for Ten Steps changes in maternity practices should be considered and may receive renewed national political and fiscal support.
Conclusions
There is apparent ongoing interest in implementation of the Ten Steps and in BFHI, despite the possible reduction in BFHI-specific resource allocation; such reduction may be contributing to the reduced rates of reporting. Increased promulgation of the revised BFHI materials and the recognition that implementation of even some of the steps can have a positive impact may help additional countries, their hospitals, and their associated training centers to strive to attain these skills and practices in a sustainable manner. Revitalization and greater institutionalization into national standards should contribute to the renewed interest in maternal/neonatal health and community interventions and attract renewed and strengthened political and fiscal support. In sum, these practices have been shown to increase breastfeeding initiation and exclusive breastfeeding, with all of its maternal and child health and survival impact, and therefore the Ten Steps and BFHI have a vital role as we continue efforts to increase in the rates of exclusive breastfeeding worldwide.
Footnotes
Acknowledgments
I would like to start by noting that the BFHI monitoring data through the 2006 update in this paper were fully supported and collected by and for UNICEF purposes, and are presented here with permission of UNICEF. In addition, I would like to acknowledge the support and cooperation of UNICEF (www.unicef.org/nutrition/index_breastfeeding.html), especially Dr. Nune Mangasaryan and Christiane Rudert, and their facilitation of contacts with UNICEF Regional Nutrition Officers and the generosity of those UNICEF Officers in countries for giving their time to this purpose. I also would like to thank Sarah Amin and the World Alliance for Breastfeeding Action (![]() ) for her encouragement to undertake this latest update of the BFHI data and especially to thank all the BFHI committees and UNICEF Officers who responded to this request for updates. The preparation of this article was funded by the Carolina Global Breastfeeding Institute Endowment and Operating Funds, which also supported the 2010 BFHI data collection exercise, assisted by in-kind support from UNICEF and BFHI committees worldwide, and World Alliance for Breastfeeding Action.
) for her encouragement to undertake this latest update of the BFHI data and especially to thank all the BFHI committees and UNICEF Officers who responded to this request for updates. The preparation of this article was funded by the Carolina Global Breastfeeding Institute Endowment and Operating Funds, which also supported the 2010 BFHI data collection exercise, assisted by in-kind support from UNICEF and BFHI committees worldwide, and World Alliance for Breastfeeding Action.
Disclosure Statement
The author is the Director of the Carolina Global Breastfeeding Institute, which funded this update and analysis. No competing financial interests exist.