
Abstract
Abstract
Background:
Although late preterm infants (LPIs), at 340/7–366/7 weeks of gestation, are reported to have suboptimal rates of breastfeeding, there is a lack of quantitative evidence describing this trend. This study examined the prevalence of breastfeeding initiation and factors associated with breastfeeding non-initiation within a Pennsylvania population-based cohort of late preterm mother–infant dyads.
Subjects and Methods:
Descriptive statistics and odds ratios were used to assess and compare breastfeeding initiation rates in 2003–2009 among LPI mothers (n=62,451) and their infants (n=68,886) with moderately preterm (n=17,325) and term (n=870,034) infants. Binary logistic regression was used to determine the association of system/provider, sociodemographic, and medical factors with breastfeeding non-initiation in late preterm mother–infant dyads for the year 2009 (n=7,012).
Results:
Although LPI breastfeeding initiation in Pennsylvania increased significantly from 2003 (54%) to 2009 (61.8%) (p<0.001), the 2009 prevalence remained well below rates in term infant populations and national standards. The regression model indicated that interactions involving sociodemographic variables, including marital status, age, race/ethnicity, education, parity, Women, Infants and Children Program participation, and smoking status were among the most significant factors associated with LPI breastfeeding non-initiation (p<0.05). The univariate results were similar to those reported in preterm and term populations.
Conclusions:
Our data suggest that certain, unexpected demographic groups in the late preterm population be prioritized for further analysis and possibly greater breastfeeding support. More research is indicated to understand the effect of modifiable psychosocial factors on LPI breastfeeding initiation.
Introduction
Both trends and factors associated with subpar breastfeeding initiation within the late preterm population have not been adequately investigated. Because national and state-level breastfeeding prevalence data specific to LPIs are not reported, the scope of the breastfeeding issue in this population remains vague. Unrecognized infant physiological immaturities and related system factors have been implicated in poor rates of breastfeeding continuation and exclusivity in LPIs, but it is unclear what factors are associated with early or in-hospital breastfeeding in this group and how these compare with the general population. This article describes temporal trends (2003–2009) and a predictive model for LPI breastfeeding non-initiation in the state of Pennsylvania accounting for social, medical, and system-level variables.
Subjects and Methods
Study design
We examined early breastfeeding prevalence among LPI mothers (n=62,451) and their infants (n=68,886) in 2003–2009 and compared the latter with moderately preterm (301/7–336/7 weeks of gestation; n=17,325) and term (≥37 weeks of gestation; n=870,034) infants in the same time period. Logistic regression was used to determine the association of system/provider, infant, and maternal sociodemographic and medical factors with breastfeeding non-initiation in late preterm mother–infant dyads for the year 2009 (n=7,012). All data were obtained from a de-identified electronic birth certificate file prepared by the Bureau of Health Statistics and Research, Pennsylvania Department of Health (Harrisburg, PA) after institutional review board approval. SPSS versions 18 and 20 (SPSS, Inc., Chicago, IL) were used for all statistical analyses.
Twenty-five variables, based upon the literature and registry availability, were included in the initial screening procedure for the predictive model. Maternal variables examined included age, prepregnancy body mass index (BMI), birth country, smoking during pregnancy, marital status, level of education, Hispanic ethnicity, race, history of prematurity, history of infertility treatment, Medicaid status, parity, Special Supplemental Nutrition Program for Women, Infants and Children (WIC) status, and diabetic status (gestational and types 1 and 2). Infant variables examined included gender, birth weight, weeks of completed gestation, neonatal intensive care unit (NICU) admission, and plurality. System or obstetric practice variables included delivery attendant, receipt of first trimester prenatal care, use of anesthesia during labor, induction or augmentation of labor, and route of delivery. Because of excessive missing data or categorical outliers, eight variables of interest were retained for descriptive purposes only and were not included in the regression procedure (Table 1).
We were unable to compute an unadjusted odds ratio (uOR) for body mass index (BMI), as it violated assumption of linearity in the logit and was not amenable to transformation.
Variable not included in the regression model because of outliers or missing data.
Birth weight transformed to kilograms to achieve meaningful OR.
CI, confidence interval; CM, Certified Midwife; CNM, Certified Nurse Midwife; DO, Doctor of Osteopathy; MD, Medical Doctor; NA, not applicable; NC, not calculated (used for descriptive purposes only); NICU, neonatal intensive care unit; WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
Pennsylvania birth certificate data are compiled via electronic transfer from healthcare providers, whose procedures for data collection may vary, to the Bureau of Health Statistics and Research. Breastfeeding initiation is recorded post-delivery by medical staff on a worksheet that asks the question, “Is the newborn being breastfed?” Anectodally, this is often a verbal question posed to mothers, although it is intended to be based on the provider's observations. The timing of this assessment post-birth is also unstardardized (A. Farrell, Pennsylvania Department of Health, personal communication, 2011). 5 2003 was the first year in which breastfeeding was assessed as part of the Pennsylvania birth registry.
Gestational age is assessed by the birth attendant and defined as his or her final estimation of gestation, based on all perinatal factors and assessments, but not the neonatal examination, date of last menstrual period, or date of the infant's birth. Other variables included in this analysis are abstracted from the medical record post-delivery and are based upon either maternal self-report to the medical provider or the provider's observations (A. Farrell, Pennsylvania Department of Health, personal communication, 2011). At least one study suggests that birth record data are relatively reliable for variables pertaining to labor outcomes, obstetric and maternal history, and infant-related variables but less reliable for variables involving maternal co-morbidities and obstetric complications. 6
Because an LPI sample capable of receiving breastmilk feeds was desired, infants and mothers with significant morbidity or factors demonstrated to preclude or seriously hinder breastfeeding initiation were excluded from the predictive model (n=414). Mothers were excluded based on documentation of a ruptured uterus, unplanned hysterectomy, and/or maternal admission to the intensive care unit. Infants were excluded if any of the following conditions was documented: anencephaly, seizure or serious neurologic dysfunction, congenital heart disease, gastroschisis, omphalocele, congenital diaphragmatic hernia, Down's syndrome, chromosomal disorder, cleft lip and/or palate, adoption, 5-minute Apgar score <3, and assisted ventilation for >6 hours. Seven very low birth weight (<1,500 g) infants were part of the final regression sample; these infants' weights clustered around 1,500 g, and they had a breastfeeding rate of 62%, suggesting that they were capable of receiving breastmilk feeds. To ensure independence of observations in a de-identified dataset, only year 2009 data from singleton or first-born multiple infants were used. Cases with missing data on variables of interest were eliminated after a missing values analysis indicated that missingness occurred in a random pattern. To ensure a representative sample, a sensitivity analysis was conducted comparing logistic regression results with and without outliers. The final regression sample included 7,012 mothers of singleton, or first-born mutiple, LPIs. Note that breastfeeding prevalence/trend data were not similarly adjusted for maternal or infant morbidities.
Analysis
Annual proportions (2003–2009) of breastfeeding initiation were calculated for LPIs, moderately preterm infants, and term infants to permit comparisons by year and gestational age category. Proportions were further broken down for LPI mother–infant dyads by gestational week and plurality.
For the year 2009, descriptive statistics and unadjusted odds ratios (uORs) were compiled examining breastfeeding non-initiation in relation to the various predictor variables (Table 1). Variables with likelihood ratio χ2 and Wald statistic p values of ≤0.25 were included in multivariate modeling (n=13), which included an examination of the “full” or “saturated” model (univariately significant variables, “adjusted” for all other variables within the model; those with p values of ≤0.25 were retained for further analysis), exploration of all first-order interaction terms (i.e., interactions between two, single variables), analysis of competing models using an all-subsets regression approach, and examination of fit indices (e.g., residuals, Wald statistics, classification tables). In order to capture all potentially significant interaction terms, a liberal cutoff p value of 0.25 was used in the retention of variables from the saturated model. The maternal age variable violated the linearity in the logit assumption and was log base-10 transformed. The final model specifies adjusted odds ratios (aORs) and 95% confidence intervals (CIs) for the most significant predictor variables. A power analysis determined that the smallest detectable odds ratio for categorical and continuous variables predicting breastfeeding non-initiation was 1.22 and 1.10 (0.82 and 0.91 for negative associations with the outcome), respectively (1 – β=0.90; α two-tailed=0.05; n=7,012; R2=0.35; p0=0.618).
Results
Temporal trends
Rates of LPI breastfeeding initiation increased significantly each year from 2003 to 2009 (uORs>1, p<0.001), except in 2004 (uOR 1.05, 95% CI 0.99–1.11, p=0.13). Compared with mothers of 34-week infants, mothers of 35- and 36-week infants were slightly, but significantly, more likely to initiate breastfeeding in the years 2003–2009 (respectively: uOR 1.08, 95% CI 1.03–1.13, p<0.01; uOR 1.14, 95% CI 1.09–1.19, p<0.001). Compared with mothers of late preterm singletons, mothers of late preterm multiples were more likely to initiate breastfeeding in 2003–2009 (uOR 1.17, 95% CI 1.11–1.23, p<0.001). There were no interaction effects of plurality with birth year or gestational age (Table 2 and Fig. 1).
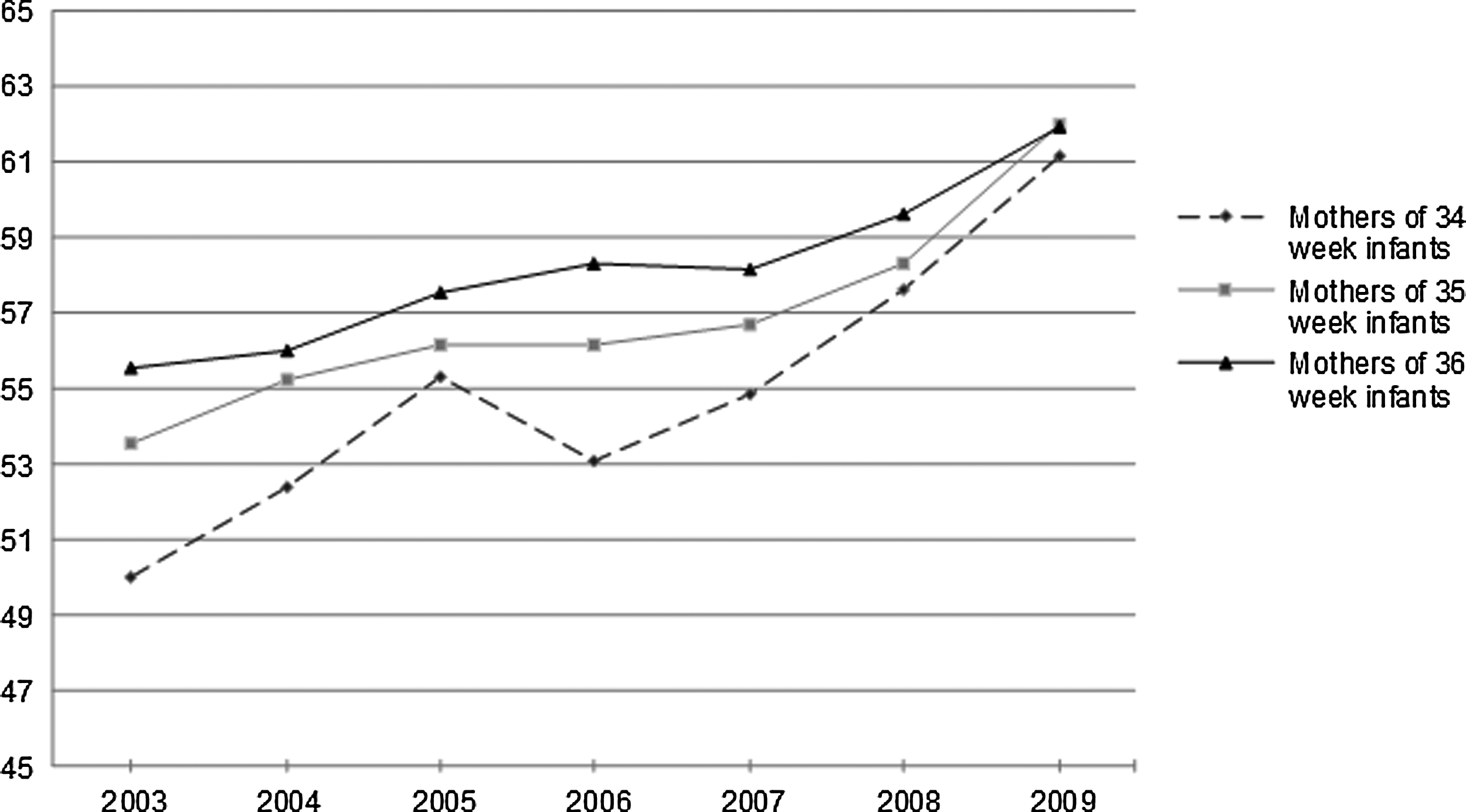
Percentages of mothers of late preterm infants (singletons and multiples) initiating breastfeeding in Pennsylvania by year and infant's gestational week. Percentages are adjusted for plurality but not maternal/infant morbidity. Mothers of 35- and 36-week infants were slightly, but significantly (p<0.01), more likely to initiate breastfeeding than mothers of 34-week infants in 2003–2009.
Rates are unadjusted infant/maternal morbidity.
GW, gestational week of infant; S, mothers of singleton infants; M, mothers of multiple infants; T, total number of mothers.
Breastfeeding initiation rates increased significantly among all gestational ages from 2003 to 2009 (p<0.001). Although rates increased most dramatically from 2003 to 2009 in moderately preterm infants (12.6%), compared with LPIs (7.7%) and term infants (7.4%), the difference was not significant (p>0.05). Compared with LPIs, breastfeeding initiation in cumulative years 2003–2009 was significantly greater among term infants (uOR 1.44, 95% CI 1.42–1.46, p<0.001) and significantly lower among moderately preterm infants (uOR 0.85, 95% C: 0.82–0.88, p<0.001) (Table 3). The 2009 rate of breastfeeding initiation among mothers of LPIs, adjusted for plurality, was 61.8±1.1%.
Rates are unadjusted for maternal/infant morbidity and plurality.
Breastfeeding initiation increased significantly among all gestational ages from 2003 to 2009 (p<0.001), but rates were significantly higher among term infants (p<0.001) and significantly lower among moderately preterm infants (p<0.001) compared with late preterm infants.
Predictive model
Characteristics of the predictive model sample are shown in Table 1. The majority of mothers were non-Hispanic white, U.S.-born, nonsmokers, with at least a high school diploma. A median maternal BMI of 24.4 kg/m2 approached the upper boundary of normal (normal BMI, 18.5–24.9 kg/m2). Median maternal age was significantly lower among those not initiating breastfeeding (27±5 years vs. 29±5 years, p<0.001). Most mothers had a vaginal delivery, a physician delivery attendant, prior live births, no history of prematurity or infertility treatment, no labor induction or augmentation, and no prepregnancy or gestational diabetes. Prenatal care data were missing for over 30% of cases, indicating a possible reliability issue with that variable. 36.9% of the sample were receiving Medicaid. Index infants were most often singletons and 36 weeks of gestation. Average birth weight was above the low birth weight criterion of 2,500 g and was significantly lower among infants whose mothers did not initiate breastfeeding (2,616.5±468.2 g vs. 2,667.5±467.9 g, p<0.001).
The uORs and 95% CIs for breastfeeding non-initiation relative to each predictor variable are also provided in Table 1. Variables with p values >0.25, and thus eliminated from multivariate modeling, included infant gender, route of delivery, labor induction or augmentation, and infant plurality. Unadjusted variables positively associated with breastfeeding non-initiation (i.e., “risk factors” for non-initiation) included being a WIC recipient, black race, smoking during pregnancy, having had prior live births, and a history of prematurity (p<0.001). Infant NICU admission also tended to be positively associated with the outcome variable (p=0.09). Unadjusted variables negatively associated with breastfeeding non-initiation (i.e., “protective” of initiation) included higher education, increasing maternal (log) age, higher birth weight, “other” racial classification (e.g., Asian), being married, and labor anesthesia (p<0.01). Being of Hispanic ethnicity and greater gestational age also tended to be negatively associated with the outcome variable (p=0.25).
The final “best fit” model included two main effect variables (i.e., variables not involved in any other significant interactions) and seven significant interaction terms (Table 4). For comparison purposes, results from the full/saturated model (model without interaction terms) are also provided in Table 4. A sensitivity analysis including multivariate outliers produced the same final model, although indices of fit (e.g., log likelihood, pseudo-R2) were slightly worse. The final model correctly classified more cases than any other model (69.4%) and better classified those breastfeeding (84%) than those not initiating breastfeeding (44.6%).
Interaction terms are not included in the full model. Significant terms for the final model are in bold type. Variables in the final model reaching univariate significance but involved in interactions are not in bold type (e.g., parity) because these variables should be interpreted solely through the interaction term. Three variables included in the full model (birth weight, gestational weeks, and previous preterm birth) were excluded from consideration in the final model because all had p values above a liberal cutoff of 0.25. These variables were deemed unlikely to gain univariate significance or be involved in significant interactions upon further modeling.
aOR, adjusted odds ratio; CI, confidence interval; NA, not applicable; NICU, neonatal intensive care unit; WIC, Special Supplemental Nutrition Program for Women, Infants and Children.
In the final model, labor anesthesia remained negatively associated with breastfeeding non-initiation (aOR 0.85, 95% CI 0.76–0.95, p<0.01), while smoking during pregnancy remained positively associated with breastfeeding non-initiation (aOR 1.74, 95% CI 1.52–1.99, p<0.001). WIC was involved in four of the seven significant interactions. A positive association with breastfeeding non-initiation was noted for WIC×married and WIC×increasing log age (aORs≥1.34, p≤0.04). WIC×Hispanic ethnicity and WIC×black race were both negatively associated with breastfeeding non-initiation (aORs≤0.73, p≤0.03).
Marital status was involved in three significant interactions, including WIC. Married×NICU admission and married×increasing educational level were both positively associated with breastfeeding non-initiation (aORs≥1.27, p≤0.04). Log age was involved in two significant interactions. Increasing log age and both WIC and parity were positively associated with breastfeeding non-initiation (aORs≥3.40, p≤0.04).
Discussion
To our knowledge, this analysis is the first to examine the impact of various sociodemographic and practice variables on LPI breastfeeding initiation, inclusive of multiple gestation infants, within a population-based sample. Sample characteristics, including infant gender, distribution of gestational age, ethnicity, education, age, parity, marital status, and Medicaid status, were very similar to those of another population-based analysis of LPIs without major medical issues, 7 although our sample had more black and U.S.-born mothers, and the 2009 rate of maternal LPI breastfeeding initiation in our sample (61.8±1.1%) was about 10% lower. This discrepancy may reflect the lower overall rates of breastfeeding initiation in Pennsylvania, which was 63.8% in 2007. 8 The majority of sample LPIs were also singletons, delivered vaginally without labor augmentation or induction. This is consistent with research that reports that nearly half of all LPIs are delivered as a result of spontaneous labor. 9 Together, these comparisons support the relative representativeness of this sample of LPIs within Pennsylvania and the United States.
As expected, because of physiological immaturity, breastfeeding initiation among LPIs was lower than among term infants within the sample, but higher with increasing gestational week and higher than among moderately preterm infants. It is interesting that some authors have reported lower rates of breastfeeding initiation and continuation among LPIs compared with earlier preterm infants, speculated to be due to extra vigilance and support of breastmilk feedings in the NICU, where early preterm infants outnumber LPIs.10,11 This likely indicates that NICU breastfeeding support varies among institutions and/or regions. The increasing trend in breastfeeding initiation among all gestational ages from 2003 to 2009 probably reflects several national breastfeeding movements that became prominent within the decade, for example, the Breastfeeding Friendly Hospital Initiative 12 and the Healthy People 2010 breastfeeding goals. 13
The higher rate of breastfeeding initiation observed among mothers of late preterm multiples compared with singletons is noteworthy. Few studies examining preterm breastfeeding include or differentiate among multiples, and there is some conflicting research regarding the effect of preterm plural births on breastfeeding.14–17 It has been suggested that higher rates of breastmilk pumping among mothers of multiples may contribute to increased breastfeeding rates. 14
The final model indicated that sociodemographic factors, including marital status, education, parity, race, age, WIC participation, and smoking status were among the most influential variables impacting LPI breastfeeding initiation. The importance of sociodemographic characteristics in early breastfeeding behavior is consistent with research in general and preterm infant populations.17,18 Although most of these unadjusted variables were associated with breastfeeding in the expected direction (e.g., black race, smoking, and WIC participation as risk factors for non-initiation; married and educated as protective), 19 the multivariate analysis revealed that these variables were involved in several significant, counterintuitive interactions. For example, univariately, being married and increasing education were both strongly protective against breastfeeding non-initiation, but their interaction reversed the direction of the association. Similarly, being a WIC recipient was a risk factor associated with breastfeeding non-initiation in the univariate analysis, but its interaction with another risk-associated variable (black race) was protective, and its interactions with breastfeeding-protective variables (log age, married) were associated with breastfeeding non-initiation. Reversal of the breastfeeding-protective univariate associations of both log age and married (uORs≤0.33, p<0.001) with parity and NICU admission, respectively, was also surprising. These findings suggest that early LPI, and probably general, breastfeeding behavior is a complex phenemenon, heavily influenced by non-modifiable sociodemographic factors in a non-additive manner. This complexity is supported by at least one study, which found a similar reversal in the effect of race on preterm and term infant breastfeeding initiation when comparing univariate and multivariate results. 20
Speculation on the causes of these interactions is somewhat futile without a basis for comparison in other populations and the likely influence of unmeasured, confounding variables. Variables such as marital status, parity, and WIC participation, for example, may be proxy factors for employment, income, and additional home/childcare responsibilities. Although the abstract nature of these interactions does not support specific breastfeeding interventions within the LPI population, they do indicate that practitioners should exercise caution in applying broad sociodemographic labels to interpret breastfeeding behavior and that certain “combination demographics” be considered in the design of future LPI breastfeeding promotion and support services and research with large sample sizes.
Anesthesia as a breastfeeding-protective factor in the final model (aOR 0.85, 95% CI 0.76–0.95) was somewhat unexpected. Research in general infant populations indicates no association21,22 or a risk association (due to mild infant sedation23,24) between labor anesthesia and early breastfeeding. Our finding must be interpreted with caution, however, as type and dose of anesthesia were not specified, and the effect size was small. The positive association of smoking with breastfeeding non-initiation (aOR 1.74, 95% CI 1.52–1.99) in the final model is consistent with findings in other infant populations reporting smoking as a risk factor for early and continued breastfeeding.25–27 Research suggests that smokers are often unsupported in their breastfeeding efforts and perceive significant infant health risks from smoking while nursing. For these reasons, mothers of LPIs should be counseled in ways to quit or reduce smoking but educated that the potential health benefits of breastfeeding, even while smoking, outweigh the associated risks. 28
It is interesting that many practice and infant-related variables, including cesarean births, labor induction/augmentation, earlier gestational age, prior premature birth, plurality, and lower birth weight, were not significant in the univariate and/or multivariate analyses. Research has suggested a negative association of all these factors with early breastfeeding.2,11,29–32 Yet, a similar study in a younger preterm population found many of the same factors to be nonsignificant in initial breastfeeding when considering sociodemographic factors. 17
A major strength of this analysis was the large, population-based sample, permitting control of multiple covariates and examination of interactions among variables. The analysis was also strengthened by differentiating between single and multiple gestation infants. A major limitation in the study design was noninclusion of more modifiable variables reported to be influential in breastfeeding (e.g., support systems, career/time conflicts). We were also unable to fully compare our model to research in other infant groups because of noninclusion of interaction terms in those studies. Despite this, we believe that the examination of interactions permits a more comprehensive understanding of breastfeeding behavior as a complex social and biologically influenced phenomenon.
Another limitation of this study is that the outcome variable—breastfeeding initiation—could not be verified as collected at a uniform point or in a standard manner (e.g., who observes breastfeeding and what constitutes “breastfeeding”) because of the generalized instructions part of the Pennsylvania birth registry. In addition, the outcome variable did not account for breastfeeding exclusivity, which is an arguably more important indicator of breastfeeding duration and success. To take advantage of a potentially very rich, population-based data source and to achieve more conclusive analyses, like others,5,33 we suggest that state birth registries streamline how breastfeeding initiation is assessed and expand to include in-hospital breastfeeding exclusivity data. We would also suggest that future late preterm breastfeeding research consider younger “term” infants (e.g., 37–38 gestational weeks). Research suggests that full neurological maturity and coordinated breastfeeding is not achieved until approximately 39–40 weeks of gestation, 34 predisposing early term infants to poorer rates of breastfeeding initiation and duration. 11
Conclusions
LPIs comprise the largest segment of preterm births in the United States and experience suboptimal breastfeeding rates, despite increased potential for benefit from breastfeeding compared with term infants. Identifying factors that influence early, in-hospital breastfeeding among late preterm mother–infant dyads serves as a starting point for targeted breastfeeding interventions and provides a basis for research investigating breastfeeding duration and exclusivity, modifiable barriers to breastfeeding, and confounding variables. With the caveat that additional research is warranted to confirm and expand upon these findings, our analysis suggests that efforts to increase early breastfeeding within the LPI population might begin with a focus on the following groups: (1) mothers who are married and educated; (2) married women with NICU-admitted infants; (4) non-traditional WIC recipients (non-minority, older, married); and (4) smokers.
Footnotes
Acknowledgments
These data were supplied by the Bureau of Health Statistics & Research, Pennsylvania Department of Health, Harrisburg, Pennsylvania. This work was funded by the National Institute of Nursing Research, Ruth F. Kirschstein National Research Service Award (F31NR0115 62).
Disclosure Statement
No competing financial interests exist.