
Abstract
Abstract
The selective serotonin reuptake inhibitor (SSRI) sertraline is widely used as an antidepressant agent during pregnancy and lactation because of its low placental transfer and low level of excretion into breastmilk. Symptoms such as neonatal abstinence syndrome and serotonergic overstimulation have been reported after in utero exposure to SSRIs. These symptoms are self-limiting and usually peak within the first 48 hours after birth. In our case, a preterm infant was exposed to sertraline and its main metabolite desmethylsertraline in utero and via breastmilk. Beyond the first 48 hours after birth, the infant developed increasing clinical signs of serotonergic overstimulation associated with substance intake via breastmilk, until breastfeeding was discontinued on postnatal Day 9. In spite of a low calculated daily substance intake via breastmilk, the serum substance levels of the preterm infant were within the therapeutic range of adults. The serotonergic overstimulation may be explained by the limited metabolic capacity of the infant and the immaturity of the blood–brain barrier.
Introduction
In association with nonpharmacological treatments such as psychotherapy, the selective serotonin reuptake inhibitor (SSRI) sertraline is a first-line antidepressant for treatment during pregnancy and lactation. This is due to its low placental transfer and its low degree of excretion into breastmilk.3,4 Here, we report serotonergic overstimulation associated with serum levels of sertraline after in utero exposure and increasing intake of sertraline via breastmilk in a preterm infant.
Case Report
Maternal history
The mother (37 years old, weighing 83 kg and 173 cm tall) fulfilled the Diagnostic and Statistical Manual of Mental Disorders criteria for a major depressive disorder. Following the birth of her first child, she was treated with sertraline for 5 years. Four months prior to her second pregnancy, sertraline monotherapy was discontinued to avoid in utero exposure. At 23 weeks of gestation, however, depression increased, and antidepressant treatment was re-initiated with sertraline and psychotherapy. Treatment with sertraline was initiated at 25 mg and increased over a 4-week period to 150 mg/day. With a daily dose of 150 mg of sertraline at the time of delivery, the mother's serum sertraline level was 47.7 μg/L, within the therapeutic range of 10–150 μg/L. 5 The serum level of desmethylsertraline (the primary metabolite of sertraline) was 127 μg/L, also within the therapeutic range of 7–185 μg/L. 6 Concentrations of sertraline and desmethylsertraline were determined using a liquid chromatography-tandem mass spectrometry assay. An in-house validated liquid chromatography-tandem mass spectrometry method for routine measurement of sertraline and desmethylsertraline in serum and plasma was used for the quantification of sertraline and desmethylsertraline in serum and breastmilk. The method was modified from that of Jain et al. 7 External quality controls are performed regularly. Because of the emulsion was not homogeneous, the breastmilk was vortex-mixed vigorously before pipetting. All calculations based on original and diluted breastmilk were performed in duplicate.
Newborn history
The eutrophic white male (birth weight, 2,490 g; length, 45 cm; head circumference, 32.5 cm) was delivered by primary cesarean section at a gestational age of 33 weeks because of premature rupture of the membranes. Apgar scores were 8, 8, and 9 after 1, 5, and 10 minutes, respectively. The preterm infant required ventilatory support by continuous positive airway pressure during the first hours of life because of mild respiratory distress syndrome. Soon after birth, the baby developed hyperthermia and muscle tone regulation disorders, including muscular hypertonia, shivering, myoclonus, and tremor, as well as irritability and high-pitched crying during the first 24 hours. On the fourth day of life increasing signs of clinical impairment became evident. The infant exhibited decreased sucking reflex and reactivity associated with muscular hypotonia, including intermittent shivering, tremor, and myoclonus, as well as high stool frequency and high-pitched crying during exclusive breastfeeding. Complete and differential blood counts and creatinine, glucose, calcium, sodium, potassium, chloride, and C-reactive protein levels were normal during repeated testing within the first days of life. In addition, there was no evidence of epileptic patterns on the electroencephalogram.
Breastfeeding and sertraline serum levels
Because sertraline is not contraindicated during lactation, the mother breastfed her newborn infant during the first days of life. Because of recurrent signs of clinical impairment, serum levels of sertraline and desmethylsertraline were measured on Day 5 in the preterm infant. Serum levels were 13.2 μg/L for sertraline and 52.1 μg/L for desmethylsertraline. At this time, the infant had been exposed to sertraline in utero for 10 weeks, and the total breastmilk intake was calculated as 785 mL. It appeared most likely that the clinical impairment was the result of neonatal abstinence syndrome (NAS) after sertraline exposure in utero, and breastfeeding was continued. On Day 9, nutrition was changed from breastmilk to formula as a result of further clinical impairment as described above. Total breastmilk intake up to that time was 2,110 mL. With formula feeding, serum levels of sertraline and desmethylsertraline decreased. The infant started to thrive and developed without any clinical impairment during the following months as confirmed by repeated neurological examination.
Discussion
Various symptoms have been reported in neonates after in utero exposure to SSRIs.3,8 These consist of muscle tone regulation disorders, including muscular hypertonia, tremor, myoclonus, and shivering, as well as irritability, excessive crying, sleep disturbances, tachypnoea, sweating, loose stools, and feeding problems.3,8 These clinical findings are similar to those seen in neonates with NAS 3 and are nearly indistinguishable from those reported from direct toxicity leading to overstimulation of the serotonergic system by SSRIs. 3 Although NAS and serotonergic overstimulation have many symptoms in common, NAS usually is characterized by muscular hypertonia and agitation rather than muscular hypotonia and decreased reactivity as exhibited in our patient beginning on the fourth day after birth. 8
In one study, 30% of neonates exposed in utero to SSRI developed NAS within the first 48 hours of life. 8 The clinical signs were comparable to those observed within the first 24 hours in the preterm infant in this study. Because no adverse effects have been previously reported in infants exposed to sertraline and desmethylsertraline via breastmilk, 9 the recurrent clinical impairment after Day 4, together with the measurable serum levels of sertraline and desmethylsertraline, was remarkable. Although therapeutic ranges for sertraline and desmethylsertraline have not yet been defined for infants, the observed concentrations were within the therapeutic ranges for adults.5,6 The recurrent clinical impairment associated with the measured serum levels of sertraline and desmethylsertraline and the absence of other indications of a severe disorder suggest the most reasonable explanation is that serotonergic toxicity leading to overstimulation of the serotonergic system was induced by substance intake via breastmilk.
In order to estimate the daily substance intake by the infant, we measured concentrations of sertraline and desmethylsertraline in the breastmilk on three different days at random times. Mean milk levels were 201.3 μg/L (range, 174–224 μg/L) for sertraline and 357.8 μg/L (range, 202–552 μg/L) for desmethylsertraline. Subsequently, the daily substance intake by the infant was calculated by multiplying the mean drug concentration in milk by the volume of milk intake assuming 100% absorption. 3 For sertraline, this result was 2 μg on the first day of breastfeeding and 78.5 μg on the last day; for desmethylsertraline the values were 3.6 μg and 139.5 μg, respectively (Fig. 1). The mean daily intake by the preterm infant was 47 μg for sertraline and 84 μg for desmethylsertraline. These values are far below the mean maximum calculated daily intake values for sertraline (670 μg) and desmethylsertraline (1,440 μg) in asymptomatic breastfed infants. 10 However, substance serum levels in the infant in this study may be explained by impaired metabolic capacity. Cytochrome P450 (CYP) isoenzymes involved in sertraline metabolism were assayed with microarray hybridization using an AmpliChip® CYP450 GeneChip® (Roche Molecular Systems, Pleasanton, CA). CYP2C19 and CYP3A4 (not determined) are primarily responsible for sertraline biotransformation to the less active metabolite desmethylsertraline, which is subsequently metabolized by CYP2D6 to didesmethylsertraline. 11 Results showed an intermediate metabolic status for both CYP2C19 and CYP2D6 isoenzymes, which may explain an extended elimination half-life of sertraline and desmethylsertraline. The average terminal elimination half-life is 26 hours for sertraline and about 78 hours for desmethylsertraline. 5 Eleven days after discontinuation of breastfeeding, the sertraline serum level in the baby was still 4.9 μg/L, and the desmethylsertraline level was 8.6 μg/L. These findings suggest a limited ability to excrete sertraline and desmethylsertraline and, in combination with the immaturity of the blood–brain barrier, may have caused the serotonergic overstimulation in the preterm infant.
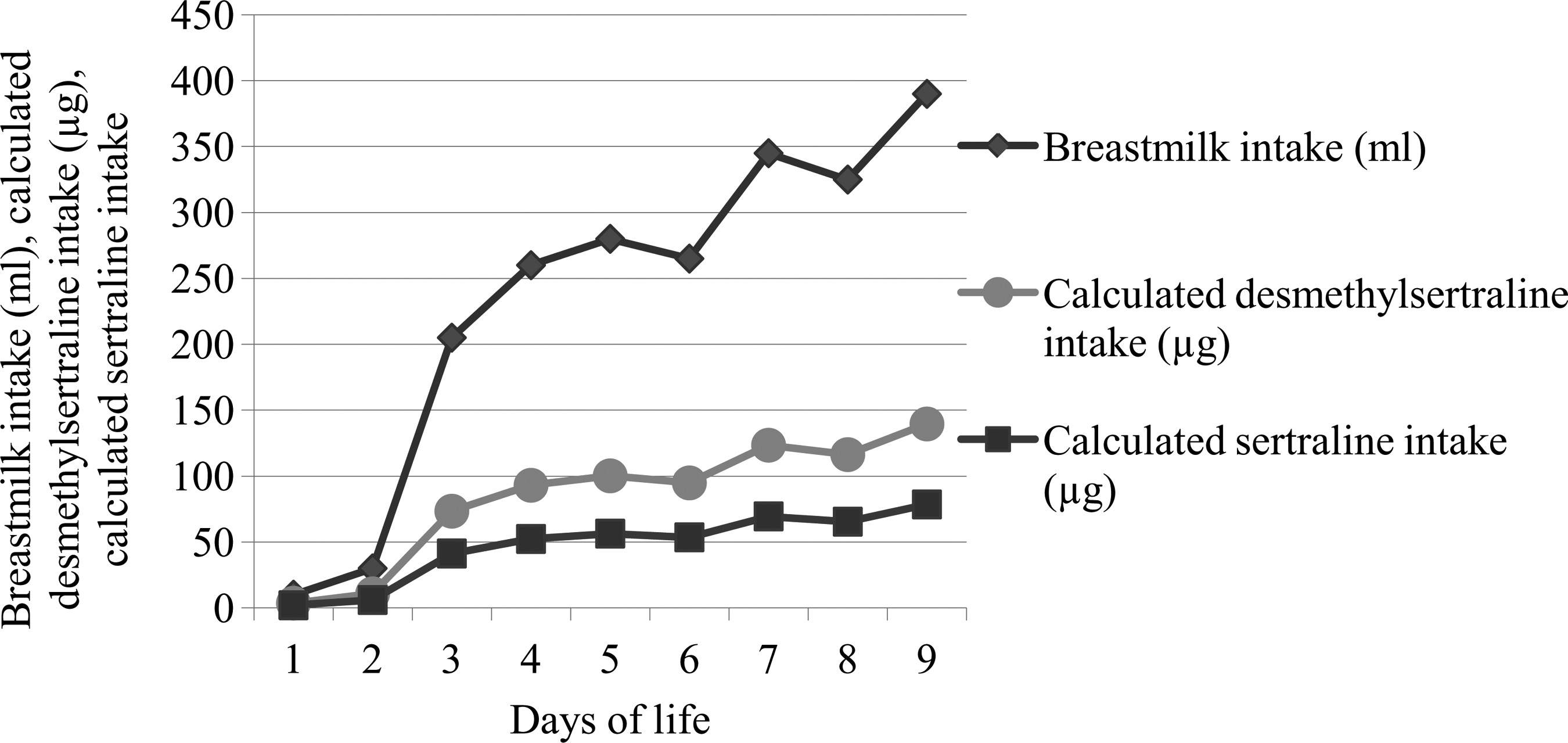
Daily breastmilk intake (in milliliters) and calculated daily intake (in micrograms) of desmethylsertraline and sertraline.
The drug transporter protein phosphoglycoprotein (P-gp) is localized at the luminal membranes of endothelial cells of the blood–brain barrier and seems to be an important factor limiting brain access by sertraline and desmethylsertraline. 12 In the fetal mouse blood–brain barrier, P-gp is increasingly expressed with increasing gestational age. 13 Therefore, it is possible that P-gp-mediated fetal neuroprotection increases in late gestation, 13 and both sertraline and desmethylsertraline may accumulate more easily in the preterm brain.
In conclusion, breastmilk from mothers receiving sertraline may lead to serotonergic overstimulation in preterm infants. Physicians should be aware of the signs of serotonergic overstimulation and stop breastfeeding in the event of serotonergic overstimulation.
Footnotes
Acknowledgments
Written informed consent for publication of this case report was obtained from the patient's parents.
Disclosure Statement
No competing financial interests exist.