
Abstract
Abstract
Background:
Breastfeeding benefits the health of babies and mothers, but returning to work is a significant barrier for mothers wishing to continue breastfeeding for the recommended 12 months. A resource training kit, The Business Case for Breastfeeding (BC4BF), developed by the Health Resources and Services Administration, U.S. Department of Health and Human Services, was implemented in Southeastern Virginia to assist businesses in developing lactation support programs (LSPs) and eliminating breastfeeding barriers.
Materials and Methods:
The primary goals of the 1-year project were to educate 20 businesses about breastfeeding support in the workplace, engage 10 businesses to implement the BC4BF, and assess sustainability via documented policy and environmental changes and integration of the LSP into the business infrastructure. The Transtheoretical Model of Behavior Change was adapted to assess stage of organizational change. A Centers for Disease Control and Prevention tool for measuring community-level policy, systems, and environmental change was adapted to assess worksite policy and environmental changes.
Evaluation Results:
Over 20 businesses were educated about the BC4BF. Seventeen engaged in the project. Fourteen significantly increased their stage of change, development of LSPs, written policies, and physical and social environment changes (p≤0.001). A brief follow-up study revealed that all 14 employers maintained their programs 8 months after the program ended, with increased stages of change, policy enforcement, and physical environment (p≤0.05).
Conclusions:
The BC4BF provided an effective approach to assisting employers in establishing and maintaining LSPs in the workplace across several cities.
Introduction
In 2011, Save the Children ranked the United States last of 36 countries on the Breastfeeding Policy scorecard. 8 It is also “the only economically advanced country”…“where employers are not required to provide any paid maternity leave after a woman gives birth.” 8 Expectant mothers in the United States can apply for leave under the Family and Medical Leave Act (FMLA), 9 providing mothers with 12 weeks of unpaid maternity leave, but not all women qualify for FMLA. For families facing financial hardships, unpaid leave is not a feasible choice. Ninety-eight countries give new mothers 14 weeks or more of paid maternity leave. 10 The United States is one of only four countries that do not provide paid maternity leave; the other three countries are Liberia, Papua New Guinea, and Swaziland. 10 Because of these challenges many women in the United States must return to the work force with young infants.
To help address these issues, Healthy People 2020 includes a goal to “increase the proportion of employer worksite Lactation Support Programs to 38%” (up from 25% in 2009), 11 and The Surgeon General's Call to Action to Support Breastfeeding, 12 issued in January 2011, includes a section calling for lactation support in employment settings. It recognizes that breastfeeding rates will increase with changes in the workplace, such as longer and/or paid maternity leave, part-time hours, and breastfeeding support programs. The Internal Revenue Service in 2010 deemed that breast pumps and supplies that assist lactation are considered medical supplies, 13 thus making these eligible for tax breaks and/or flexible spending accounts.
The passage of the Patient Protection and Affordable Care Act (ACA), signed into law by President Obama in 2010, 14 was a major victory for nursing women in the workforce. Many of the ACA's breastfeeding provisions come from the Breastfeeding Promotion Act (HR 2819, S 1244), which was first introduced in both Congressional houses in June 2009 by Representative Carolyn B. Maloney (NY) and Senator Jeff Merkley (OR). 15 In the ACA, under the Fair Labor Standards (Section 7), 16 businesses with 50 or more employees are required to provide reasonable break time and a secure space, not a restroom, to nursing mothers for up to 1 year after the birth of their child. Companies with fewer than 50 employees are not subject to the break time requirement if compliance with the provision would impose undue hardship, but these companies are not automatically exempt. Meeting the requirements to become exempt is tedious, 15 requiring review of the difficulty or expense of compliance for specific employers compared with the size, resources, nature, and structure of the business. All the employer's employees, regardless of worksite, are considered when determining application of this exemption. 17 With the Supreme Court's decision to uphold the ACA, 18 the implementation of workplace breastfeeding support continues. Individual states can create their own laws, and the law with superior provisions takes precedence. Even with these provisions in place, many women still struggle to express breastmilk at work. Unfortunately, for employers that do not comply with the law, there are no real mechanisms in place to enforce the law.
The Business Case for Breastfeeding (BC4BF) toolkit, released in 2008 by the Maternal and Child Health Bureau in the Health Resources and Services Administration, U.S. Department of Health and Human Services, is a valuable resource available free, online in English and Spanish, to employers developing worksite lactation support. 7 The Health Resources and Services Administration conducted qualitative research with businesses to determine the efficacy of the BC4BF toolkit for use in business settings. The toolkit contains both print and electronic resources and provides materials and information targeted specifically for employers, employees, and others. It outlines the benefits of worksite lactation support for employers and provides them with resources to develop their own program. The toolkit also provides information and resources for new mothers, including advice for approaching supervisors about lactation support.
The toolkit contains data 7 summarized below, indicating that supporting breastfeeding mothers in the workplace is better for the business bottom line. Businesses with lactation support programs (LSPs) show higher retention rates. For example, Mutual of Omaha boasts an 83% retention rate of female employees versus the national average of 59%. As most employers know, retaining good employees is much less expensive than training new staff. A study at Aetna determined that the return on investment in LSPs is 3 to 1. Companies with LSPs also have lower healthcare costs. CIGNA demonstrated an annual savings of $240,000 in healthcare expenses; there were 60% fewer prescriptions dispensed, and the company saved $60,000 in reduced absenteeism rates. Mutual of Omaha demonstrated an annual savings of over $115,000 in healthcare claims among enrolled families; per-person costs were over $1,200 more for employees who did not participate in the lactation program.
Materials and Methods
With funding from the Virginia Department of Health, the Consortium for Infant and Child Health (CINCH), a children's health coalition sponsored by Eastern Virginia Medical School, implemented the BC4BF among employers in the multicity region of Hampton Roads in Southeastern Virginia. From September 2010 through October 2011, CINCH conducted a BC4BF implementation program at worksites in five Hampton Roads cities: Chesapeake, Newport News, Norfolk, Portsmouth, and Virginia Beach. Employers were recruited from existing organizational partners of CINCH and from employers of large numbers of women of childbearing age, 16–44 years old. The focus was on healthcare facilities as organizations likely to value lactation support and respond favorably to this program. Recruitment strategies included e-mail, phone, and in-person contact during meetings, information-sharing at health reform seminars, and a workplace wellness conference.
The program goals were (1) to educate at least 20 employers about the program and how it might benefit their business, (2) to engage at least 10 employers to review the applicability of the program and assess their specific worksite needs for a new or enhanced LSP, (3) to implement the program in the engaged worksites, providing technical assistance for planning, policy development, and environmental changes, and (4) to evaluate progress and outcomes. Each employer was contacted by phone and e-mail and offered an in-person consultation, site visit, and free technical assistance from the program manager. A lactation assessment form (LAF) was adapted from the BC4BF toolkit for planning purposes. The LAF was required for those businesses requesting incentives to help establish their lactation spaces. The program provided incentives, including a selection of tangible items, such as hospital-grade breast pumps, chairs, tables, refrigerators, and other supplies.
Project staff reached over 20 employers with education about BC4BF. Seventeen of these employers were engaged, as determined by their providing a letter of support for the program, having a consultation meeting with program staff, and/or agreeing to follow BC4BF guidelines as feasible for their organization. Employers were recruited on an ongoing basis; thus engagement varied from 4 to 12 months of participation. Staff assessed progress on the following six outcome measures using ordinal rating scales:
1. Level of engagement in the BC4BF program 2. Stage of organizational change based on the Transtheoretical Model of Behavior Change
19
3. Level of LSP comprehensiveness 4. Policy development 5. Physical environment 6. Social environment
The policy and two environment scales were adapted from the Community Health Assessment and Group Evaluation (CHANGE) tool developed by the Centers for Disease Control and Prevention 20 to measure policy, systems, and environmental change. Table 1 describes these measurement scales.
Fifteen of the 17 employers agreed to complete the LAF as a baseline record of the type of employment setting, with human resources information including numbers of women employees of childbearing age, relevant policies, physical space, and funding available for lactation support. At each worksite, a contact person was identified to “champion” the establishment of the LSP, including developing written policy, establishing lactation rooms, identifying and securing supplies for the rooms, and utilizing the incentives available from CINCH and the Virginia Department of Health. The champion was vital in facilitating a breastfeeding-friendly work environment. Champions were persons with influence in the organization, such as an occupational health nurse, human resources manager, or department director. The champion worked with the CINCH program manager to implement the BC4BF in a manner tailored to the needs and resources of that worksite.
Progress toward improved lactation support was scored using the six ordinal scale measures mentioned above. A follow-up study was conducted during June and July 2012, approximately 8 months post-program, to further assess sustainability and maintenance of changes. A brief follow-up questionnaire was developed and administered via telephone to key contacts at each worksite. Employers were given follow-up scores for five of the six scales described above, omitting Engagement because there was no opportunity to maintain engagement after the end of the program in October 2011. Wilcoxon Signed Rank tests for repeated measures were performed to compare baseline, post-intervention, and follow-up median scores.
Results
Seventeen employers provided adequate data to be included in the analysis. Fifteen of these completed the LAF as required to receive incentives; two opted not to receive incentives and did not complete the LAF. Twelve (80%) of the 15 organizations completing the LAF were mid- to large-size employers (100 to over 500 employees), and 80% were health organizations. Program staff conducted interviews and site visits to verify information and collect baseline assessment data for each worksite, including the two that did not complete the LAF. Among all 17 employers evaluated, over 6,200 women of childbearing age were impacted by this program. In two cases, hospital systems included two or more separate worksites. When policies were developed at the central locations, those policies were to be implemented at each worksite under the umbrella of the parent company. Each worksite had varying resources available for providing lactation spaces. Hence, eight new lactation policies were developed and implemented at 13 different worksites.
Median changes in scores from baseline to post-intervention were significant in the positive direction (p≤0.001) on the six outcome measures, and ranged as follows. Ranked from 1 (initial consultation) to 4 (high engagement with the program), means for engagement progressed from 1 to 3.65. Scaled from 1 (not thinking about starting an LSP) to 5 (maintenance of implementation), stage of change progressed from 1.76 to 3.94, indicating the action stage in which the LSP is operational. Scaled from 1 (no lactation support) to 3 (superior support), LSP Comprehensiveness progressed from 1.71 to 2.88, indicating the addition of components such as a lactation room, educational resources, promotion of the LSP, and social support. Scaled from 1 (no policy identified as needed) to 5 (policy evaluation and enforcement), policy progressed from 1.29 to 3.53, indicating movement through policy development to implementation of a written policy. Scaled from 1 (no or few elements in place) to 5 (all elements in place), physical environment progressed from 1.59 to 4.00 with most elements in place. Elements included items such as a private, clean space with electrical outlet, locks and appropriate signage, chair, table, cleaning supplies, running water, and milk and pump kit storage options. Scaled from 1 (no/negative support) to 5 (enthusiastic support communicated), social environment progressed from 2.53 to 3.94, indicating movement from some support to active support and absence of criticism or harassment. All changes were significant at a p value of ≤0.001. Figure 1 illustrates these results and those in the next section.
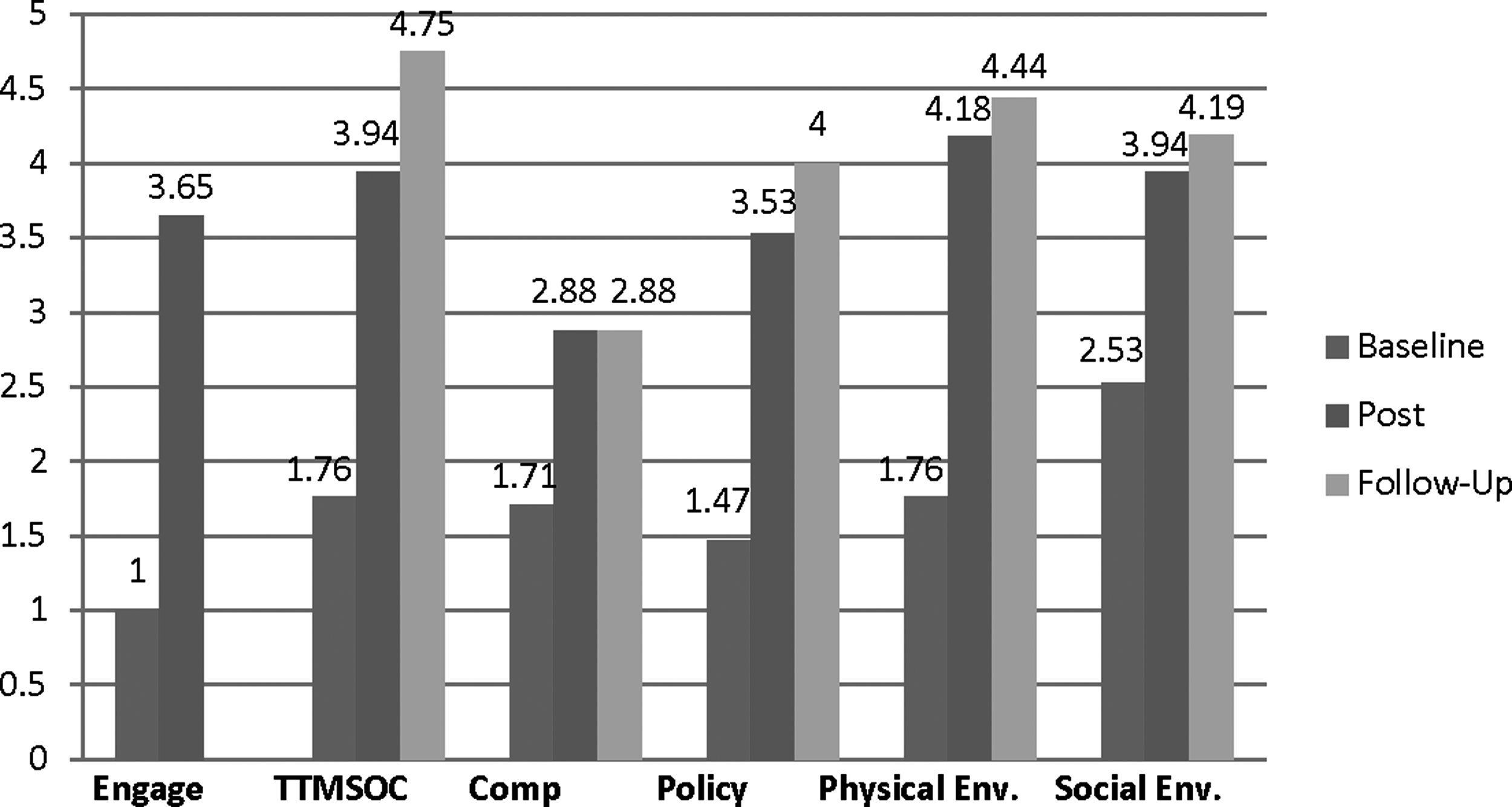
The Business Case for Breastfeeding lactation support program status over time: baseline, post-intervention, and follow-up. Comp, comprehensiveness of lactation support program; Engage, engagement; Policy, policy development and implementation; Physical Env., physical environment; Social Env., social environment; TTMSOC, Transtheoretical Model—Stage of Organizational Change.
Sixteen of the original 17 employers completed a follow-up questionnaire designed to ascertain the status of LSP maintenance 8 months post-program. None of the 16 employers had lost any elements of their LSP since post-test. Most programs remained the same, whereas several had gained elements. Because of these improvements, the mean scores for four of the five evaluation scales increased from post-test to follow-up. The largest gain was in the Transtheoretical Model of Behavior Change Stage of Change scale with a post-test mean score of 3.94 compared with a follow-up mean score of 4.75. Although the majority of employers were in the Action stage of change at post-test, most, having maintained their program for 6 months or longer, had progressed to the Maintenance stage at follow-up.
The policy, physical environment, and social environment scales saw more modest increases from post-test to follow-up. The policy mean score increased from 3.53 to 4.00 because of three employers progressing from 3 (Policy formulation) to 4 (Written policy and implementation) and three other employers progressing from 4 to 5 (Policy evaluation and enforcement). The physical environment mean score increased from 4.24 to 4.44 because of three employers increasing their physical environment score from 4 (Most elements in place) to 5 (All elements in place). Finally, the social environment mean score increased from 3.94 to 4.13 from post-test to follow-up because two employers increased their scores from 4 (Active support) to 5 (Enthusiastic support). The Wilcoxon Signed Rank Test for nonparametric data yielded significant changes from post-test to follow-up in stage of change, policy, and physical environment (p value ≤0.05). Figure 1 illustrates the results of the original baseline, post-test, and follow-up comparisons.
Discussion and Conclusions
It was thought that employers in the health field and those who were also CINCH partners would be supportive of establishing lactation support policies and LSPs and could serve as role models for non-health entities. This assumption was borne out as the majority of participating employers were large health organizations, and several were CINCH members. Additionally, project planners believed it would be more difficult to engage non–health-related organizations to implement the model if local healthcare entities had very limited LSPs in place.
This project was successful in facilitating changes in policies and environments of 15 of 17 worksites to support breastfeeding mothers and in maintaining those gains in 14 organizations over time. Limitations include limited generalizability outside healthcare settings. Also, because employers differ in their need for employee lactation support and our scores allow for this broad array of responses, employers could have high scores for implementation, such as stage of change, comprehensiveness, policy, and basic physical environment and still not fully meet the needs of their employees. Conversely, employers could make extensive changes to meet the needs of their employees, but this may not be fully reflected in their scores. Next steps include further refinement of the measurement methods. Currently underway is implementation of the BC4BF in more diverse employment settings.
Footnotes
Acknowledgments
The Virginia Department of Health provided the core funding for this project. Eastern Virginia Medical School provided support for the follow-up study and manuscript development. All of the employers, champions, and supporters of this project contributed to the success of the work, and we are grateful to all of them.
Disclosure Statement
No competing financial interests exist.