
Abstract
Abstract
Objective:
The benefit of antenatal nipple correction remains inconclusive. This study aims to demonstrate the value of breast cups in lengthening of short nipples and to compare the breastfeeding rate between the users and the nonusers.
Subjects and Methods:
Singleton pregnant women with at least one short nipple (<7.0 mm) were enrolled at a gestational age (GA) of 16–20 weeks. All participants were randomly allocated into the breast cup group (BC group) and the expectant group (EX group). The first group was requested to wear breast cups for at least 8 hours during the daytime, whereas the second group was not. The nipple length was evaluated prior to the study and at every visit until GA of 36 weeks by the same blinded evaluator.
Results:
Among 90 eligible participants (43 in the BC group, 47 in the EX group), the nipple elongation in the BC group was significantly higher than in the EX group (2.37±1.29 mm versus 1.84±0.98 mm; p=0.032), with a mean difference of 0.53±0.24 mm (95% confidence interval 0.05, 1.01). On Day 3, there was an insignificantly higher number of mothers with a LATCH score of ≥7 in the BC group. The 3-month exclusive breastfeeding rate in the BC group was insignificantly greater than that of the EX group (65.39% versus 50.0%; p=0.35).
Conclusions:
Breast cups are safe and well tolerated by users and evidently increase the length of short nipples and enhance the exclusive breastfeeding rate.
Introduction
Therefore, the aim of this study is to demonstrate the value of breast cups in improving the nipple length of short-nipple pregnant women. The secondary objective is to determine the breastfeeding success rate between the treated and the expectant groups.
Subjects and Methods
This randomized controlled trial was conducted at Siriraj Hospital, Mahidol University, Bangkok, Thailand. The research protocol was approved [protocol number 655/2551(EC2)] and followed the ethical standards of the institutional review board.
Singleton pregnant women with unilateral or bilateral short nipples (<7.0 mm) who attended at the antenatal care clinic between July 2009 and July 2010 were invited into the study by breastfeeding expert midwives. The pregnant women who met the criteria of age between 18 and 40 years old, gestational age (GA) of 16–20 weeks, and having no previous history of breastfeeding were recruited into the study. Patients with uncertain date, inverted (crater-like) nipple, prior nipple or breast surgery, and previous preterm birth were excluded. In cases of poor adherence to the instructed protocol, lack of completing at least four follow-up sessions, and preterm delivery (GA <36 weeks), the patients were withdrawn from the study. For sample size calculation, increasing the nipple length by 1.0±1.3 mm or greater was considered as having clinical importance. 9 By setting the probability of type I error and the power of test at 0.05 and 90%, respectively, a minimum of 72 participants had to be enrolled to the study.
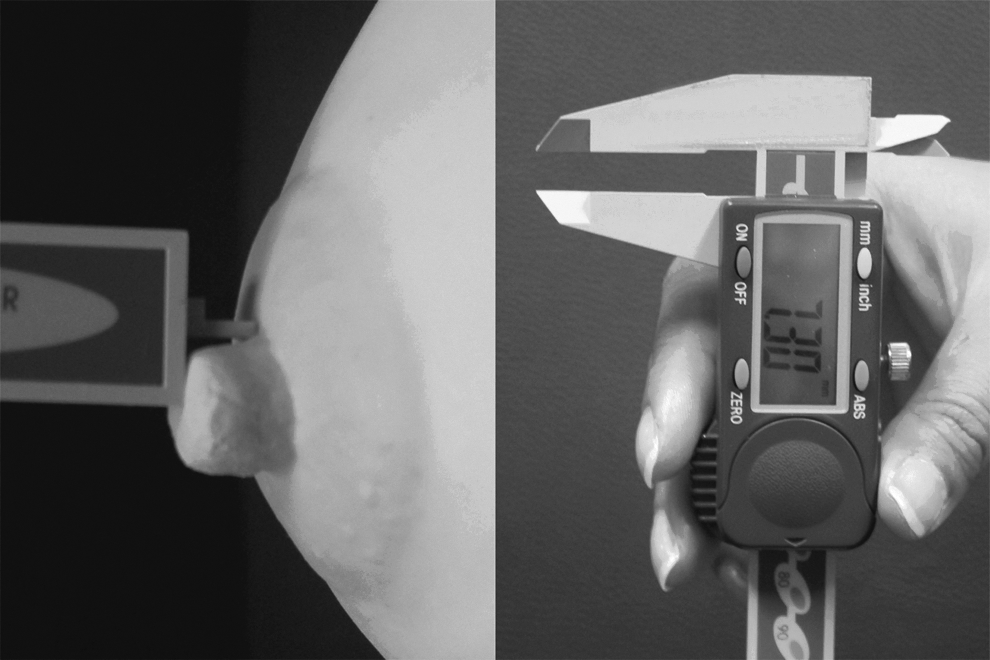
The study population was randomly allocated into two equal groups—the breast cup group (BC group) and the expectant group (EX group)—according to the number that contained in the opaque envelope randomly chosen by the researcher. The number was already block randomized by using nQuery Advisor® software (version 6.01; Statistical Solutions Ltd., Cork, Ireland, United Kingdom). Every participant underwent nipple and areola assessment in a private room. Prior to the evaluation, both nipples of each patient who sat in an upright position were rolled for 5 seconds, and then the nipple length and diameter were measured with a very precise digital Vernier caliper in millimeter units to 2 decimals (Fig. 1). For inverted nipple diagnosis, the pinch test was done by grasping each nipple at base with forefinger and thumb, and then both fingers were pressed together around the nipple base. In the case of an inverted nipple, it will clearly retract from its base. 10 The areola consistency was also determined by applying firm but gentle pressure with the index finger and thumb on either side of the areola behind the nipple. The patients in the BC group were instructed to wear both breast cups underneath their brassieres for at least 8 hours per day or 56 hours per week during daytime, whereas the participants in the EX group were asked to do nothing. Any participant in the BC group who wore breast cups for less than 80% of the required duration was withdrawn from the study. In the control group, any patient who used any treatment for nipple correction was also removed from the trial. To avoid the effect of co-intervention, the participants in the each group were separately counseled and seen for a 2–4-week follow-up depending on GA. The pregnant women in the BC group were asked to remove the breast cups on the day of evaluation.
Nipples and areolas of all cases were assessed by the same evaluator without knowledge of to which group the participant belonged. The compliance, side effects, and satisfaction of the treatment were also evaluated from the participant's self-assessment form in every visit. Postnatal lactation support was provided to all patients before discharge from the hospital. Early breastfeeding success rate was evaluated in term of LATCH score on Day 3 after delivery. Then, mothers were asked about their infant feeding type—namely, exclusive breastfeeding, mixed feeding, or formula feeding—by phone at both weeks 6 and 12.
All statistical analyses were performed using computer software (SPSS version 18; SPSS, Inc., Chicago, IL). The comparisons of demographic data, nipple length, nipple diameter, LATCH score on Day 3, and infant feeding type at weeks 6 and 12 between the two groups were determined by using an independent t test and Pearson's χ2 test. The statistical significance was reported by a p value of <0.05 with 95% confidence interval.
Results
In total, 96 pregnant women initially enrolled into the study, but six were withdrawn from the study: three cases of abortions and three cases of incomplete follow-up. Finally, there were 90 participants remaining, with 43 cases in the BC group and 47 cases in the EX group. The demographic data of the sample population showed no significant differences between the two groups (Table 1).
Data are mean±SE values.
The statistical significance was analyzed by independent t test. A p value of <0.05 was statistically significant.
For the two nipples of each patient, we elected to use the data from the shorter side as a representative for statistical analysis. Means of pretreatment nipple length in the BC group and the EX group were comparable (4.19±1.08 mm and 4.41±1.29 mm, respectively; p=0.387). During pregnancy, nipple elongation was demonstrated in both groups. However, the improvement of nipple length in the treated group was 0.53 mm greater than in the control group with statistical significance (2.37±1.29 mm and 1.84±0.98 mm, respectively; p=0.032). The nipple widening was also observed along with increase in GA, but there was no statistical difference between the two groups (1.62±1.50 mm and 1.57±1.19 mm, respectively; p=0.858) (Table 2).
Data are mean±SE values.
The statistical significance was analyzed by independent t test. A p value of <0.05 was statistically significant.
To demonstrate the clinical improvement, the type of nipple length was classified into three groups: very short (<4.0 mm), short (4.0–6.9 mm), and normal (≥7 mm) nipples. The outcome in the BC group was better than in the EX group in term of the conversion of very short and short nipples to normal nipples (21 of 43 [48.83%] versus 15 of 47 [31.91%], respectively) (Table 3). However, there was no statistical difference by McNemar's test analysis.
Nipple length was classified into three groups by length: very short (<4.0 mm), short (4.0–6.9 mm), and normal (≥7 mm).
It is interesting that the number of patients with a LATCH score of ≥7 on Day 3 in the BC group was higher than in the EX group without statistical significance (37.5% versus 22.6%; p=0.182). However, the exclusive breastfeeding rate on Day 3 in the BC group was significantly lower than in the EX group (63.9% versus 37.9%; p=0.037; data not shown). The high initial breastfeeding failure or delayed lactogenesis in the treated group could be derived from various factors, including maternal or fetal stress during labor and delivery. As a result, it might impair the milk ejection reflex and milk production reduction. Unfortunately, the data we collected were not useful for exploring this concern. At 3 months after delivery, the number of women exclusively breastfeeding between the two groups changed. Despite the fact that similar lactation supports were given to both groups during hospitalization, the percentage of exclusive breastfeeding in the BC group rose considerably up to 65.39%, whereas that of the EX group steadily decreased to 50% (Table 4). Regarding the side effect of breast cup wearing, most of the users (95.3%) felt that it was comfortable to wear the devices during pregnancy. In this group, the incidence of mild uterine contraction with spontaneous recovery was 48.1%.
The statistical significance was analyzed by Pearson's χ2 test. A p value of <0.05 was statistically significant.
Discussion
In an effort to increase breastfeeding practices, the United Nations International Children's Emergency Fund (UNICEF) and the World Health Organization had launched an international campaign of the Baby-Friendly Hospital Initiative since 1991 through the 10 Steps to Successful Breastfeeding. Nevertheless, global breastfeeding rates remained low and showed marked social inequalities, especially in developed countries. In 2005, the breastfeeding rate in the sixth month in the United Kingdom was the lowest in Europe, compared with Sweden (22% versus 72%). 11 In Singapore, a national survey in 2001 found that the breastfeeding rate dropped from 72% at the first month to 21% by 6 months. 12 Recently, a randomized controlled trial showed that women receiving either antenatal breastfeeding education or postnatal lactation support were two times more likely to breastfeed exclusively at 6 months compared with women who received routine care. 13
In Thailand, a national survey in 2005 reported that exclusive breastfeeding at 6 months was only 14.5%, whereas the national target of the 9th National Health Development Plan has been set at 30%. 14 Siriraj Hospital as a tertiary hospital setting has been certified by UNICEF as the first Baby-Friendly university hospital in Thailand since 1993. In agreement with the 10 Steps to Successful Breastfeeding, antenatal education of breastfeeding benefits, breast examination, and nipple preparation have been provided for all pregnant women. Based on our previous study, 1 women with a nipple length of ≥7 mm are more likely to succeed in breastfeeding at a four times higher rate than those with short nipples. In our practice, if a flat, inverted nipple or hard areola is detected, anatomical correction will be offered during pregnancy by various techniques, including Hoffman's exercise, breast cups, and nipple puller. In addition, postnatal lactation support is provided to all mothers before discharge. However, the benefit of antenatal nipple preparation has been in doubt in terms of anatomical improvement or successful breastfeeding as reported by two randomized controlled studies.5,6 Moreover, the result discouraged the policy of routine breast examination and antenatal nipple correction during pregnancy, which has been a global practice.
Unlike previous findings, our study revealed a higher degree of nipple elongation for the BC group compared with the EX group. In our study, only short-nipple pregnant women were enrolled, whereas inverted nipple cases were excluded. It could be explained that inverted nipple was actually a surgical rather than a mechanically corrected condition.
We also showed better clinical outcome in term of the conversion of short and very short nipples to normal nipple length in the treated group. Because of high loss of follow-up rates, the study was barely to conclude that the exclusive breastfeeding rate was improved by breast cups. Further study must be done to demonstrate the impact of prenatal breast cup wearing on breastfeeding success. Despite complaint of skin rash (22.2%) and mild uterine contraction (48.1%), the majority of breast cup users tolerated wearing breast cups very well.
Owing to the research methodology, our randomized controlled trial had no sample selection bias. The single evaluator did not know to which group each participant belonged. In this study, women with inverted nipples who were uncorrectable without surgery were excluded. Regarding the accuracy of measurement, the digital Vernier caliper was able to determine the nipple length in millimeter units to 2 decimals. The compliance of mothers in each group was closely monitored by the clinical project manager and documented in case record forms to ensure that all participants complied with the assigned intervention without co-intervention. In statistical analysis, the nipple length from the most severe side was selected for analysis.
In this study, 30–40% of cases were unable to contact by phone after delivery. Therefore, the data on infant feeding type at weeks 6 and 12 were incomplete. Nevertheless, the exclusive breastfeeding rate at 3 months in our study remained high, amounting to 57% (32 of 56 cases). It has been reported that 68% of mothers admitted that early lactation problems were the main reason they stopped breastfeeding before 2 months postpartum. 15 Thus, early postpartum lactation support from healthcare providers should be given to all patients for breastfeeding establishment and maintenance. Further study should be focused on the effect of postpartum intervention on breastfeeding success rate, including the benefit of breast cup or breast pump use and peer support from the breastfeeding group.
Conclusions
Breast cups are safe and well tolerated by the users and evidently increase the length in short-nipple mothers as well as enhance the exclusive breastfeeding rate. Therefore, breast examination and nipple preparation are undoubtedly important and strongly recommended in antenatal care practice.
Footnotes
Acknowledgments
Funding is supported by the Routine to Research Management Fund, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand.
Disclosure Statement
No competing financial interests exist.