
Abstract
Abstract
Background:
Although medical research has proven that breastfeeding is unparalleled in providing the ideal nutrition for infants, “the demarketing of breastmilk substitutes” is a little-known concept. This empirical study tackled the origin and definition of demarketing, examined the different factors affecting the demarketing of breastmilk substitutes in Palestine from the breastfeeding woman's point of view, and developed an appropriate model for the demarketing of breastmilk substitutes. The article subsequently concludes with recommendations for areas of further academic research in the World Health Assembly, for policy makers in Palestine, and for the breastfeeding women themselves.
Subjects and Methods:
An empirical study was conducted to collect the primary data using a questionnaire as a tool in order to test the hypotheses. The questionnaire was distributed to 400 breastfeeding women who were randomly selected from the population.
Results:
The findings proved that there is a relationship between independent variables (i.e., product, price, place, and promotion) and the dependent variable (i.e., demarketing of breastmilk substitutes) based on several reasons discussed thoroughly in this article.
Conclusions:
Product, price, place, and promotion affect the demarketing of breastmilk substitutes in Palestine.
Introduction
One industry at the center of demarketing is breastmilk substitutes. Breastmilk substitutes are one of the most important global health risk factors that have negative effects on both the mother and infant.2–4 Poor breastfeeding practices are still common in both developing and developed regions. Based on previous investigations, only 39% of children worldwide are solely breastfed for 4 months, whereas a significantly smaller proportion is breastfed for the entire recommended 6 months. Breastmilk substitutes and feeding bottles impose a great risk on infants and can be life-threatening. Formula milk and bottles are not sterile products, as both may carry germs. Thus, contaminations leading to fatal infections are likely to occur in bottle-fed infants.5–7
In other words, a breastmilk substitute such as powdered infant formula is one of the most important global health risk factors that have major socioeconomic implications for societies in both developed and developing countries. It has been confirmed that powdered infant formula is associated with serious illness and death in infants due to infections with Enterobacter sakazakii and Salmonella enterica, as it is subject to contamination with harmful bacteria throughout the production process. This is because current manufacturing technology is not capable of producing sterile powdered infant formula (e.g., inappropriate handling).
As stated by the World Health Organization (WHO), 5 artificial feeding is much more expensive, as it requires clean water, specific mixing instructions, and a minimum standard of overall household hygiene. These requirements are not readily met by many households around the world. Currently, suboptimal breastfeeding is associated with over a million deaths each year and 10% of the global disease burden in children. 8 In contrast, it is estimated that a high degree of adoption of optimal breastfeeding practices could prevent 13% of the 10.6 million deaths that occur globally in children under 5 years of age every year. It has been ascertained that infants who are not breastfed for the first months have a 25 times increased risk of dying than infants who are solely breastfed. 5
The International Code of Marketing of Breast-milk Substitutes was adopted by the World Health Assembly, the forum of WHO, on May 21, 1981. 9 (The World Health Assembly is the decision-making body of WHO. It is attended by delegations from all WHO Member States and focuses on a specific health agenda prepared by the Executive Board. The main functions of the World Health Assembly are to determine the policies of the Organization, appoint the Director-General, supervise financial policies, and review and approve the proposed program budget. The World Health Assembly is held annually in Geneva, Switzerland. 10 ) The Code was developed as a global public health strategy to make sure that mothers are not put off breastfeeding and to ensure safe use of breastmilk substitutes if needed. The Code recommends marketing restrictions of breastmilk substitutes (such as infant formula; other milk products, foods, and beverages, including bottle-fed complementary foods; feeding bottles; and teats). It also highlights ethical marketing regulations for the feeding bottles and teats. The Assembly has further clarified certain provisions of the Code in subsequent resolutions.5,11
Within the same context, the Thirty-Fourth World Health Assembly (held in May 1981) stated that all Member States should interpret the International Code into national legislation, involve all connected parties in its implementation, and supervise its compliance with the Code. It also called upon the Director-General of WHO for any possible support to assist the Member States in the Code's implementation. 12 Additionally, in 2005 the World Health Assembly requested that WHO develop such guidelines in order to minimize the risk to infants. 13
Medical research has proven that breastfeeding is unparalleled in providing the ideal nutrition for infants and that it also provides safe, clean, and immunized nutrition for babies.14–21 Food manufacturers have created a wariness in the minds of mothers about whether breastmilk is the best nutrition for the babies (particularly if the infants have been ill or the parents are working mothers). The promotional activities—created by these companies—have been so influential that most people have begun to believe that breastmilk substitutes are better than mother's milk itself.
Based on a study conducted by the International Baby Food Action Network, 22 Palestine does not publish laws based on the International Code of Marketing of Breast-milk Substitutes, as is the case in many other countries. It is worth mentioning that, even though Palestine has one of the highest infant mortality rates worldwide, recent statistics showed a drop in infant mortality rates, from 25.5 for every 1,000 infants in 2000 to 20.6 in 2010. It has also been confirmed that there happened to be an increase in breastfeeding rates between 0 and 5 months from 16.7% in 2000 to 26.2% in 2010. 23
The extensive use of breastmilk substitutes in many countries—including Palestine—could be attributed to the increased pressure places on “modern” behavior. This includes exposure to mass media, contact with western health practices, and assertive marketing of breastmilk substitutes as well as Code violations by baby food manufacturers.24,25 The remaining text of this article is organized as follows: the relevant literature is reviewed, and the methodology used is described; the findings are analyzed and discussed, and, finally, conclusions and recommendations are provided.
Subjects and Methods
Definition of demarketing
Demarketing is simply described as the attempt to discourage demand for a product or service. Demarketing may target overall demand or demand from a specific market segment. An industry definition of demarketing focuses on efforts aimed at discouraging (not destroying) the demand for a product, which (1) a firm cannot supply in large-enough quantities or (2) does not want to supply in a certain region where the high costs of distribution or promotion allow for only a small profit margin. 26
Concerning the more academic definitions of authors and researchers, the concept of demarketing was initially proposed by Kotler and Levy 27 in 1971. They defined demarketing as “that aspect of marketing that deals with discouraging customers in general or a certain class of customer in particular on either a temporary or permanent basis.” In addition, demarketing (in a social marketing context) can also be defined as having the objective to decrease demand by discouraging consumption or use of products such as alcohol and cigarettes that pose a health risk. 28 According to Gupta, 29 demarketing can be defined as marketing aimed at limiting growth, practiced, for example, by governments to conserve natural resources or by companies unable to serve adequately the needs of all potential customers. From the researcher's point of view, it is noted that there is a consensus on what is the meaning of demarketing based on the definition of Kotler and Levy. 27
Types of demarketing
According to Kotler and Levy,
27
there are three types of demarketing depending on the nature of the demand that it is necessary to reduce. These types are:
• General demarketing. This is used when a firm (or government) wants to demarket to everyone. For instance, the government demarkets cigarettes and alcohol (discouraged goods) and illegal drugs (banned goods). In other words, general demarketing occurs when demand for a product or service is deemed to be too high. Demarketing is undertaken to ideally shrink total demand to an acceptable level. • Selective demarketing. This type attempts to lower the demand for a product in a particular market, usually where one market is less profitable than other markets for the product. This is often done where the cost to manufacture, advertise, or promote the product is greater in one market than in other markets. In other words, selective demarketing is concerned with a company seeking to reduce demand within certain segments of the market among specific types of consumer. • Ostensible demarketing. This involves the manufacturer appearing to discourage demand, while actually retaining the intention of increasing it. This relies on the principle that customers will be attracted as the product becomes harder to obtain.
International Code of Marketing of Breast-milk Substitutes
Before discussing the International Code of Marketing of Breast-milk Substitutes, it is crucial to highlight the significance of breastfeeding.
Breastfeeding is safe and clean, and breastmilk is full of antibodies, protecting the infant from many common childhood illnesses such as diarrhea, pneumonia, ear infection, Haemophilus influenzae infection, meningitis, and urinary tract infection.30–32 Additionally, it protects against chronic conditions of childhood such as allergies, type 1 diabetes, ulcerative colitis, and Crohn's disease and is associated with higher IQ scores in low-birth-weight babies. 33 It is also linked to lower mean blood pressure, lower total serum cholesterol, lower prevalence of type 2 diabetes, and lower obesity during adolescence and adult life. 34
For the mother, breastfeeding delays early return of fertility and reduces her risk of postpartum hemorrhage, breast cancer, and ovarian cancer. 35
According to WHO, 34 interventions to improve breastfeeding practices are more cost-effective than those for curative interventions.
The International Code of Marketing of Breast-milk Substitutes basically is a code that protects and promotes breastfeeding through providing adequate information on breastfeeding and marketing regulations for breastmilk substitutes.9,12 (The International Code of Marketing of Breast-milk Substitutes is an international health policy framework for breastfeeding promotion adopted by the Thirty-Fourth Session of the World Health Assembly of the WHO in 1981 as “a minimum requirement” to protect and promote breastfeeding [an equally unique but threatened practice], through the provision of adequate information on appropriate infant feeding and the regulation of the marketing of breastmilk substitutes, bottles, and teats. In subsequent years additional resolutions have further defined and strengthened the Code. 36 The Code was passed by 118 votes to 1, with the United States casting the sole negative vote, whereas three Member States abstained [Argentina, Japan, and Korea].8,37) The Code provides encouragement that babies should be breastfed instead of bottle-fed. If for any reason babies are bottle-fed, then it should be done safely, as well as pointing out that breastmilk substitutes should be available when needed, but not be promoted. 5
Based on a decision made by the World Health Assembly, governments of Member States decide on the legislation, regulations, and/or other suitable measures to give effect to the Code and the subsequent relevant World Health Assembly resolutions in their own countries. This means that it is up to individual Member States to decide what, if any, actions they would take in response to a violation of the Code. 38
The Code specifies clearly that the public should not be subject to promotions of breastmilk substitutes, bottles, and teats. It also states that health facilities and health professionals should not take part in promoting breastmilk substitutes as well as not provide free samples to pregnant women, new mothers, or families.9,39
Since 1981, 84 countries have endorsed all or many of the Code's provisions and the subsequent relevant World Health Assembly resolutions, whereas 14 countries have draft laws pending adoption. To ensure the Code and maternity protection laws are implemented in more countries, UNICEF is working with legislators and lawyers. 36
Previous studies
Numerous studies from different perspectives have been carried out to understand the phenomenon of demarketing of breastmilk substitutes. However, none of the studies examined the demarketing of breastmilk substitutes in Palestine.
It has been proven that the aggressive marketing of breastmilk substitutes results in increased child morbidity and mortality, especially in resource-poor countries. 8 A study conducted on the use of social marketing as a tool for enhancing health promotion programs has revealed that social marketing programs are needed to improve mothers' knowledge of breastfeeding level and increase the prevalence of breastfeeding. 2
In New York City, the infant formula industry has contributed to low rates of breastfeeding through various methods of marketing and advertising infant formula. In addition, although the majority of mothers initiate breastfeeding (85%), a minority of infants are breastfed exclusively at 8 weeks postpartum (25%). 14
In an American Indian population in Minnesota, factors positively associated with breastfeeding initiation included positive breastfeeding attitudes and social support for breastfeeding from the woman's husband/boyfriend and her mother; factors positively associated with breastfeeding at 2 weeks postpartum were support from the woman's mother and positive attitudes about breastfeeding. 40
In Portland, OR, among women who had initiated breastfeeding, 66.8% reported having received hospital discharge packs. Women who received these packs were more likely to exclusively breastfeed for fewer than 10 weeks than were women who had not received the packs. This means that hospital discharge packs are one of several factors that influence breastfeeding duration and exclusivity. 39
One of the major factors associated with inadequate protection, promotion, and support of breastfeeding has been proven to be the lack of political will. 15 Additionally, maternal employment has also been confirmed to be negatively associated with both breastfeeding initiation and breastfeeding duration. 18
In a study investigating the prevalence of violations of the International Code of Marketing of Breast-milk Substitutes carried out in one city each in the countries of Bangladesh, Poland, South Africa, and Thailand, findings have revealed that violations of the Code were detected with a simple survey instrument in all of the four countries studied. Ninety-seven out of 370 (26%) mothers in Bangkok reported receiving free samples of breastmilk substitutes, infant formula, bottles, or teats compared with only one out of 385 mothers in Dhaka. Across the four cities, from three out of 40 (8%) to 20 out of 40 (50%) health facilities had received free samples, which were not being used for research or professional evaluation. 37
Even though the previous studies have been carried out in different regions, there is a semiconsensus among researchers about many of the factors affecting the demarketing of breastmilk substitutes. It is also evident that governments are well positioned to play a central role in the demarketing of breastmilk substitutes.
Research framework
The original work of Kotler and Levy 27 regarding input analyses was found to be useful in constructing this research model. The model is partially normative and partially descriptive, as can be seen in Figure 1.
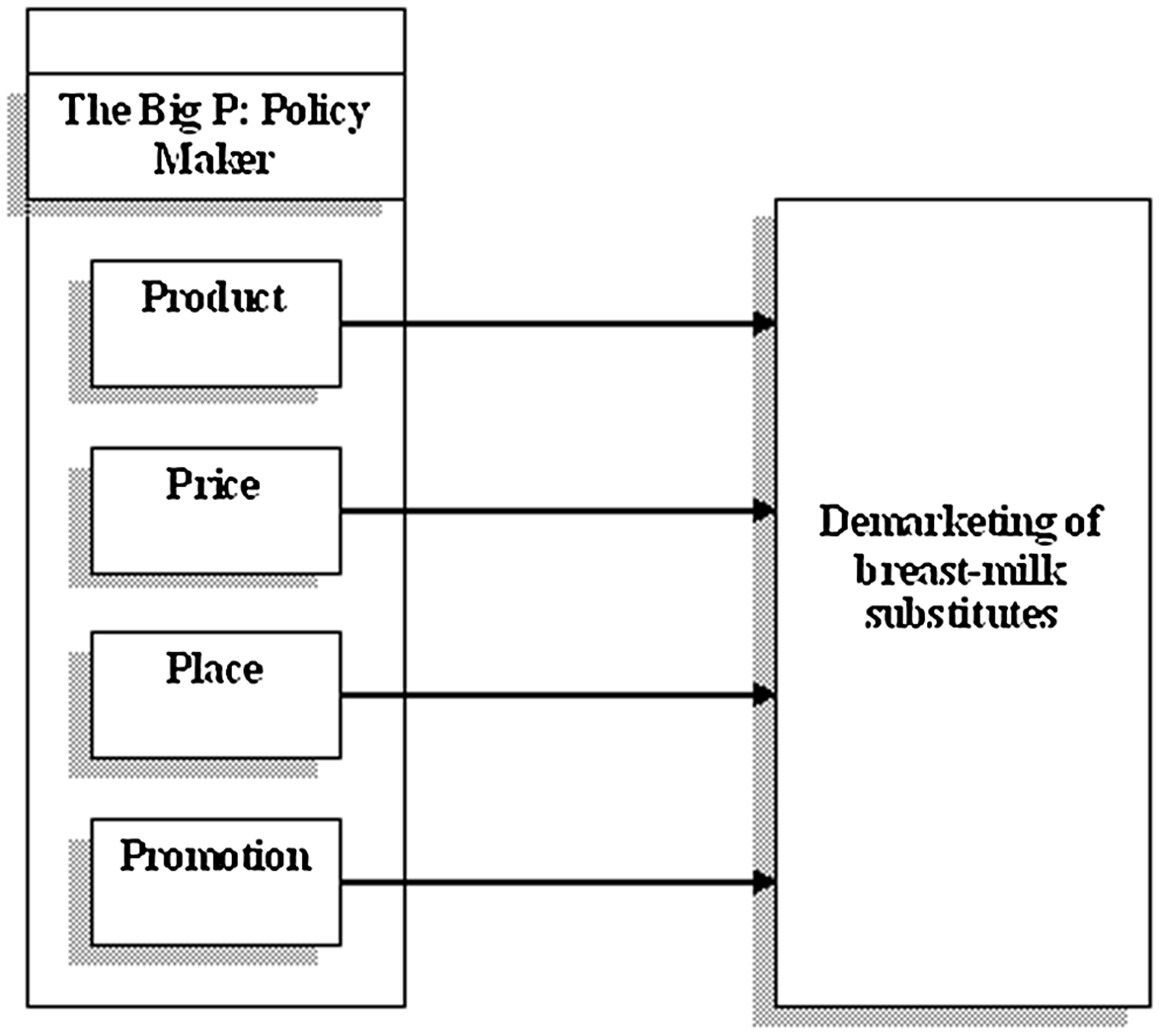
The research framework.
The proposals of Kotler and Levy 27 are partially evident in the normative part of the model. However, the researcher is solely responsible for the descriptive part—upon which the hypotheses of this study will be based. According to Lawther et al., 41 Kotler and Levy 27 acknowledged that their article about demarketing in 1971 was purely theoretical and that there is a need for careful research to substantiate and clarify their ideas.
Methodology and data collection
This research followed a descriptive approach, which is the most logical and appropriate approach to describe the current situation and answer pertinent questions on factors affecting the demarketing of breastmilk substitutes in Palestine. A questionnaire was developed in order to investigate factors affecting demarketing of breastmilk substitutes from the breastfeeding women's point of view.
According to the literature, the population is the entire group under study, which is all the breastfeeding women in Palestine. The sample is a subset of the population that should represent the entire group. For this research, a simple random sample of 400 breastfeeding women was selected.
The sample size was determined following the method of determining sample size. A sample size of 384 could be used in large populations, which will give the researcher a margin error of only 5%. The sample size required can be calculated according to the following formula42,43:
where N is sample size, NP is population size, and e is the errors term, equal to 0.05.
The sample size in this research is more than the recommended number, which will increase the level of certainty. Of the 400 breastfeeding women who were chosen to participate in this research, 17 refused to participate for various reasons; another eight had agreed to participate in the research but either did not answer most of the questions or refused to answer the questions when they saw the questionnaire. Despite these difficulties, the researcher redistributed the 25 questionnaires to obtain a total sample size of 400 breastfeeding women.
Practically, the researcher used a questionnaire designed to study factors affecting demarketing of breastmilk substitutes in Palestine. The questionnaire was reviewed and evaluated by people who specialized and were interested in the field of marketing, and statistics were calculated to guarantee the questionnaire's validity and reliability and to clarify any ambiguity in the questions. The researcher has modified, deleted, and added the necessary parts of the questionnaire in response to the group's suggestions.
After the preliminary design, a pilot study was conducted to evaluate the effectiveness of the survey. The researcher distributed the questionnaire to a sample of 40 breastfeeding women respondents. (An Arabic version of the questionnaire was tested in order to make sure that the questions were easily understood.)
In addition, the researcher used Cronbach's α coefficient test to measure the questionnaire reliability of each section and the total average of the questionnaire. From the analysis, the Cronbach α coefficients were equal to 0.919 as shown in Table 1, which means that they are significant and highly reliable coefficients.
Results and Discussion
Demographic profile
As shown in Table 2 above, the age groups 30 years or less and 31–40 years accounted for the largest percentages of breastfeeding women respondents. In addition, the largest percentage of respondents was unemployed. However, the majority of respondents were bachelor degree holders. Furthermore, the monthly salaries of respondents were between 0 and 1,500 new Israeli shekels.
NIS, new Israeli shekels.
Product impact
In general, Table 3 demonstrates that product affects demarketing of breastmilk substitutes from the breastfeeding women's point of view, as the total mean values (MVs) were equal to 3.28 and the standard deviation (SD) values were equal to 0.765.
MV, mean value; SD, standard deviation.
Price impact
Overall, Table 4 demonstrates that price affects demarketing of breastmilk substitutes from the breastfeeding women's point of view, as the MV was equal to 3.47, and the SD was equal to 0.887.
MV, mean value; SD, standard deviation.
Place impact
In total, Table 5 demonstrates that place affects demarketing of breastmilk substitutes from the breastfeeding women's point of view, as the MV was equal to 3.26, and the SD was 0.881.
MV, mean value; SD, standard deviation.
Promotion impact
Generally speaking, Table 6 demonstrates that promotion affects demarketing of breastmilk substitutes from the breastfeeding women's point of view, as the MV was equal to 3.36, and SD was 0.861.
MV, mean value; SD, standard deviation.
Hypotheses testing by using one-sample test
Table 7 shows that the t test of the demarketing mix product, price, place, and promotion (the “4Ps”) was significant, accounting for 9.794 at a significance (two-tailed) of 0.000. It reveals that there is a statistical relationship between the demarketing mix (product, price, place, and promotion) and the demarketing of breastmilk substitutes from the breastfeeding women's point of view.
Pearson correlation among independent and dependent variables
Significant interrelations existed among the elements of demarketing mix (product, price, place, and promotion) as shown in Table 8.
Conclusions
After careful, thorough, and statistical analysis of the data collected, the following are the most important conclusions of the study:
• Product affects the demarketing of breastmilk substitutes through applying governmental importing restrictions on formula milk, decreasing the amount of formula milk packaged in each container, highlighting the drawbacks of using infant's formula milk as a substitute for breastmilk on the milk container itself, importing high-quality infants' formula milk based on world standards, obliging the infants' milk producers and importers to explain all the product-related information in Arabic, prohibiting the use of infants' photos as a marketing strategy to promote selling the product (infants' milk), providing statements on the superiority of breastfeeding on infants' milk substitutes' labels based on consultation with health professionals, not permitting nutrition and health claims on labels for breastmilk substitutes (unless allowed by national legislation), explicit warnings on labels of breastmilk substitutes to inform mothers about the risk of contamination of powdered formula, and providing labels illustrating the cost and dangers associated with the unnecessary or improper use of the infants' milk substitutes. • Price affects the demarketing of breastmilk substitutes. This relationship exists through raising the price of the infants' milk container, raising the tax applied on the imported processed infants' milk products, diminishing the trust given to the distributors of the processed infants' milk (wholesalers and retailers), and increasing the costs associated with importing licenses and selling processed infants' milk products. • Place affects the demarketing of breastmilk substitutes through limiting and diminishing the number of places where processed infants' milk products are sold, prohibiting processed infants' milk products in public places, creating special areas within public spaces for women intending to feed their infants formula milk, prohibiting hospitals and clinics from displaying posters or any propaganda means for infants' milk products, and prohibiting hospitals and clinics from accepting any container of infants' milk products as advertising materials from the producing companies. • Promotion affects the demarketing of breastmilk substitutes through prohibiting promotion campaigns for processed infants' milk products, increasing and furthering antipromotion campaigns (as noticing pamphlets showing the harms of processed infants' milk products), diminishing cuts on importing of processed infants' milk products, making promotion campaigns (prizes and valuable gifts) by the government and the relevant institutions to those breastfeeding women who gave up processed infants' milk products, prohibiting infants' milk producers and importers from giving free-of-charge samples to pregnant women, children, mothers, or health workers, prohibiting infants' milk producers and importers from giving any infants' milk advertising sample to pregnant women, children, or mothers, prohibiting infants' milk marketers (company representatives) from making direct or indirect contact with or providing advice to pregnant women, children, or mothers, prohibiting infants' milk producers and importers from controlling any event or occasions or conferences for the same purposes, and prohibiting infants' milk producers and importers from promotional devices such as discounts and special displays at the retail level. • It is essential to give the demarketing concept the same importance as that given to the modern marketing concept that relies mainly on the 4Ps of the marketing mix (product, price, place, and promotion) and the integrity between them. • The demarketing concept focuses mainly on two concepts: the promotion concept and its elements represented specifically by advertisements, as well as the product element. Hence, this research will be more comprehensive to shed light on the 4Ps of demarketing. In the same context, it should be noted that most articles of the International Code of Marketing of Breast-milk Substitutes focused mainly on the promotion and the product in sequence. Furthermore, many studies, including Pago et al.,
2
Cattaneo and Quintero-Romero,
15
and Lindenberger and Bryant,
32
focused only on the promotion element. Therefore, the World Health Assembly recommended the necessity of adding some articles related to the price and place. • The Arab communities (including Palestine) are governed by Islamic traditions, as most of the population are Muslims. Although there are many Holy Quran verses encouraging breastfeeding for the first 2 years, such as Luqman:14 (“We have committed man about his parents. His mother carries him in her womb in weakness and debility, weaning him in two years. So he should be grateful to Me and to his parents. To Me is the journeying back”), the percentage of breastfeeding is decreasing constantly because of the promotional campaigns by baby food manufacturers.
Recommendations
First, in the field of studies
• Conducting further research on the concept of “demarketing” in other fields, such as the reduction of sugar consumption.
• Conducting further research on violations of the International Code of Marketing of Breast-milk Substitutes.
• Identifying all the measurement methods of demarketing efficiency and effectiveness to facilitate its application in a practical way to software programs.
Second, for the World Health Assembly
• Changing the title of the code from the “International Code of Marketing of Breast-milk Substitutes” to the “International Code of Demarketing of Breast-milk Substitutes.”
• Adding some articles concerning the price and place of breastmilk substitutes.
• Carrying out intensive promotional activities in all countries in cooperation with local authorities.
• Forming a committee to follow up with governments to issue legislation to commit to the spirit of the Code.
Third, for policy makers in Palestine
• Considering the concept of demarketing is an important concept to diminishing the number of breastfeeding women or make some of them give it up.
• Policy makers should take actions to reduce the rate of use of breastmilk substitutes by using the demarketing mix (product, price, place, and promotion) because the right use of the 4Ps of the demarketing concept is the focal point and because today demarketing of breastmilk substitutes is a must from the researcher's point of view.
• Demarketing policies of policy makers on control of breastmilk substitutes should be applied with the force of law because use of breastmilk substitutes is not a rational choice.
• Policy makers should implement a comprehensive package of control measures for breastmilk substitutes. This will lead to a major fall-off in consumption of breastmilk substitutes.
• The Palestinian Government should act on the Code, taking into consideration subsequent relevant World Health Assembly resolutions. The Government can adopt legislation, regulations, or other measures such as national policies or codes. In addition, the government should take into account that the Code is a minimum requirement, and therefore the government can adopt additional, possibly more stringent, measures than those set out in the Code and make them legally binding.
• Although governments have the primary responsibility to take action on the International Code, they can only achieve this with the full cooperation of all concerned stakeholders, including food manufacturers and distributors, healthcare professionals, nongovernmental organizations, and consumer organizations as follows:
○ Primary responsibility for the implementation and monitoring of the Code lies with governments, acting individually and collectively through the WHO. Other concerned parties, nationally and internationally, should fully collaborate with governments in this endeavor. ○ Manufacturers and distributors of products that fall within the scope of the Code are responsible for monitoring their marketing practices and taking steps to ensure that their conduct fully conforms with the Code. ○ Similarly, health professionals and health managers have a responsibility to monitor marketing practices and ensure that their institutions or practices fully comply with the provisions set forth in the Code. ○ Nongovernmental organizations, institutions, and individuals can draw the attention of manufacturers and distributors to activities that are incompatible with the Code and inform the government so that action can be taken. ○ To be accredited as “Baby-Friendly,” hospitals should avoid supporting the promotional activities of breastmilk substitutes and related products, bottles, and teats and not accept free or low-cost supplies or give out samples of those products. Hence, infant formula needed for infants with medical reasons for its use should be obtained through normal procurement channels.
Fourth, for pregnant women and mothers
Breastmilk substitutes are one of the most important global health risk factors that have major socioeconomic implications for societies, in both developed and developing countries, such as Palestine. And, because the rate of use of breastmilk substitutes in Palestine is considered to be one of the highest in the world, it is subsequently recommended that the community encourage mothers to stop using breastmilk substitutes for their babies along with help from policy makers and further research.
Footnotes
Acknowledgments
The author would like to thank Mrs. Rania Al-Muzaini and Mr. Yaser Kishawi for their valuable editorial assistance in the preparation of this article. In addition, the author would like to thank Mr. Nabil Saraf and Mr. Nabil El Zaeem for their encouragement.
Disclosure Statement
No competing financial interests exist.