
Abstract
Abstract
Background:
Pregnancy is becoming more common in residency, and about 80% of residents are female. This leads to questions of breastfeeding, work demands, and perception of burden by colleagues. This study was designed to assess experiences of (1) breastfeeding obstetrics residents and (2) their colleagues.
Materials and Methods:
This was a cross-sectional study of obstetrics and gynecology residents. Residents were categorized into experience with or no experience with breastfeeding to determine differences.
Results:
Responses were obtained from 404 residents in obstetrics. Breastfeeding is common, with 90% of residents knowing a breastfeeding resident and 22% of residents reporting personal experience with breastfeeding. Breastfeeding residents (n=89) felt support from their faculty and fellow residents. More than one in three breastfeeding mothers felt they placed extra demands on colleagues, despite 80% of colleagues reporting that they did not feel that breastfeeding colleagues placed extra demands. A breastfeeding policy was important to 85% of residents, but only 7% believed their program had one. Two-thirds of breastfeeding residents struggled with low milk supply and stopped breastfeeding early.
Conclusions:
Despite high levels of perceived support from faculty/fellow residents, breastfeeding residents struggle with low milk supply and work demands that lead to early discontinuation.
Introduction
Obstetrics and gynecology residency programs have the largest proportion of female residents (79%) compared with pediatrics (63%) and family medicine (53%). 7 In addition, an increasing number of female residents (approximately 15%) are becoming pregnant, with planned pregnancy rates up to 77%. 8 This increasing proportion of resident mothers provides a dilemma for the specialty of obstetrics and gynecology—a specialty known for long work hours and the stresses of surgical training—not only for the mother resident, but also for colleagues. One irony in obstetrics and gynecology is that these physicians are on the frontlines in terms of breastfeeding promotion to pregnant patients, but are in a career in which many aspects are not conducive to breastfeeding.9–11
Lacking in many studies is the experience of colleagues. It is reasonable to postulate that resident mothers may create extra burdens for colleagues and may negatively impact training. Conversely, colleague residents may value the benefit of learning more about breastfeeding and may use the opportunity to meet educational objectives. Planned pregnancy rates were 93.1% in a small cohort of obstetrics and gynecology residents included in a survey assessing number of cases and surgical experiences, and this study demonstrated that surgical numbers were no different between women with pregnancy during residency and those residents without pregnancy. 12
The specific aims of this cross-sectional study were (1) to assess the experiences of breastfeeding mothers in obstetrics and gynecology residency and (2) to assess the experiences of colleagues. The hypotheses are that mothers who breastfed during obstetrics and gynecology residency would experience early discontinuation due to work demands and that colleague residents would generally be supportive of their breastfeeding resident.
Subjects and Methods
This study was exempted from review by the Maricopa Integrated Health System Institutional Review Board prior to collection of the data. The Accreditation Council for Graduate Medical Education data from 2009–2010 show there are 247 obstetrics and gynecology residency programs with 4,689 residents. 7 Sample size calculation was based on an estimate of 15% of breastfeeding residents (our program's rate) and a small pilot study of eight residents. This pilot study indicated that at least 69 residents in each of two groups were needed to demonstrate clinically useful differences between groups on attitudes about breastfeeding during residency. A clinically useful difference was judged to be about 10%, which is consistent with previous differences seen in our pilot survey, with power set at 80% and α error set at 0.05 (PASS version 08.0.15 software; NCSS, Kaysville, UT). The two groups were defined by respondents' answers to survey questions. The group with breastfeeding experience agreed with the statement that they or a partner had previous or current experience with breastfeeding. In addition to the standard set of survey questions, only female residents who were currently breastfeeding or had previously breastfed were asked additional survey questions on issues related to breastfeeding during residency. The group of colleagues without breastfeeding experience also consisted of obstetrics and gynecology residents who had denied personal or partner experience with breastfeeding. No faculty, attendings, or medical student colleagues were included in this survey.
A survey instrument was developed that addressed major themes and aims of this study, which included maternal and colleague perspectives about breastfeeding during residency (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/bfm). The survey instrument was validated individually with a small group of residents in our program (n=4) who were selected by a random number generator to identify if the wording, pacing, and meaning of questions were satisfactory to achieve study objectives. An additional small group of residents (n=4) piloted and verified the survey instrument to be valid for use with obstetrics and gynecology residents. About 10–15 minutes was required to complete the survey.
Eligible study subjects were all obstetrics and gynecology residents (male and female) currently enrolled in residency in the United States and any recently graduated residents (less than 2 years) who were willing and able to answer online survey questions. Exclusion criteria included those unwilling or unable to answer online survey questions or that it had been more than 2 years since graduation from obstetrics and gynecology residency.
This observational study used a self-administered online survey (SurveyMonkey.com LLC, Palo Alto, CA). An anonymous survey link was e-mailed to residency coordinators in the United States in February 2011, with Institutional Review Board exemption notification, and a request to forward the survey onto residents and recently graduated residents. A second e-mail notification was sent in April 2011 with minimal increase in the number of respondents. Confidentiality was maintained during data collection and analysis phases. The results were anonymous and were not connected to IP addresses or e-mail addresses. Randomly selected respondents received a $50 gift card, which did require respondents to enter their e-mail address to participate; these responses were obtained separately from the data collected.
The primary outcome was the difference in the attitudes of residents with breastfeeding experience and colleague residents during residency. Other variables collected included demographics (such as gender, year in program, age, marital status, ethnicity), number of children, breastfeeding status and history, partner/spouse breastfeeding status and history, experience with colleagues' breastfeeding during residency, and personal experience with breastfeeding during residency (if applicable). Only women with current or previous experience with breastfeeding during residency were asked additional follow-up survey questions on their experience. Themes were explored including reasons for discontinuing breastfeeding, perception of placing extra burdens on colleagues, appropriate places to breastfeed or pump, and personal experiences with colleagues and faculty (if applicable). Survey responses were analyzed for trends, percentages, and common themes. Data were analyzed with χ2 tests for categorical variables and t tests for continuous variables with a p value of ≤0.05 considered to be significant.
Results
Responses were obtained from 404 residents in obstetrics and gynecology (6% response rate), with 141 residents having experience and 263 residents having no experience in breastfeeding. There are small differences in number of respondents due to residents not being required to answer every question. Breastfeeding is common, with about 90% (n=357) of residents knowing a resident who was breastfeeding and overall 22% (n=89, which is 25% of all female residents) of residents reporting personal experience with breastfeeding.
Demographic data (Table 1) between groups of residents with and without breastfeeding experience indicate breastfeeding residents were more likely to be older, further along in obstetrics and gynecology training, and married, but less likely to plan to do a fellowship. There were no significant differences in gender or ethnicity between the groups.
Total study size is 404 residents, with 65% overall in the no experience with breastfeeding group and 35% overall in the experience with breastfeeding group.
Data analyzed with χ2 test, except where indicated.
Data analyzed with independent-groups t test.
Breastfeeding mothers in residency (n=89) generally felt supported by their program director (73%), faculty (73%), and fellow residents (84%). More than one in three breastfeeding mothers (43%) felt they placed extra demands on their fellow colleagues, despite nearly 80% of colleagues (n=294 of 369) reporting they did not feel breastfeeding residents placed extra demands on them. Two-thirds of breastfeeding residents struggled with low milk supply (n=60), and two-thirds of former breastfeeding residents stopped breastfeeding earlier than expected (n=32 of 46). The most common reasons for stopping breastfeeding early included low milk supply (55%), work demands (44%), and the perception that it was too hard during residency (37%). Some (n=5) of the mother residents reported that the baby did not want to latch after receiving many hours of bottles or that the “baby was less interested.” Many residents attempted to add a pumping session (49% [44/89]), supplemented with formula (43% [38/89]) or breastmilk (40% [36/89]), or took herbal supplements (40% [36/89]) to deal with low milk supply (Table 2). Mother residents on average breastfed for 6.9 months, and the rate of breastfeeding at 6 months was 52%, which is still below the Healthy People 2020 goal of 60%. All breastfeeding mothers (100%) felt successful in meeting personal residency goals, and 75% of resident mothers felt successful in meeting personal breastfeeding goals.
The totals for columns are less than individual responses as respondents were allowed to check multiple answers to the question: “How did you deal with low milk supply? Check all that apply.”
There was no significant difference in support given or burden felt by colleague residents based on past breastfeeding experience (Fig. 1). A policy of supporting breastfeeding was important to 85% of all residents, but only 7% believed their program had a policy. There was no difference in the number of times that residents thought a mother should pump on a 12–16-hour shift (three or four times) or during a 24-hour shift (six or seven times) based on previous experience with breastfeeding (Fig. 2). The range of pumping while being on-call did not include zero in the responses from either group (i.e., none of the residents expected a mother resident not to pump for that length of time). Sadly, one resident reported being told by a fellow resident not to breastfeed because of it being too hard to do during residency (however, the vast majority of mother residents never had this experience).
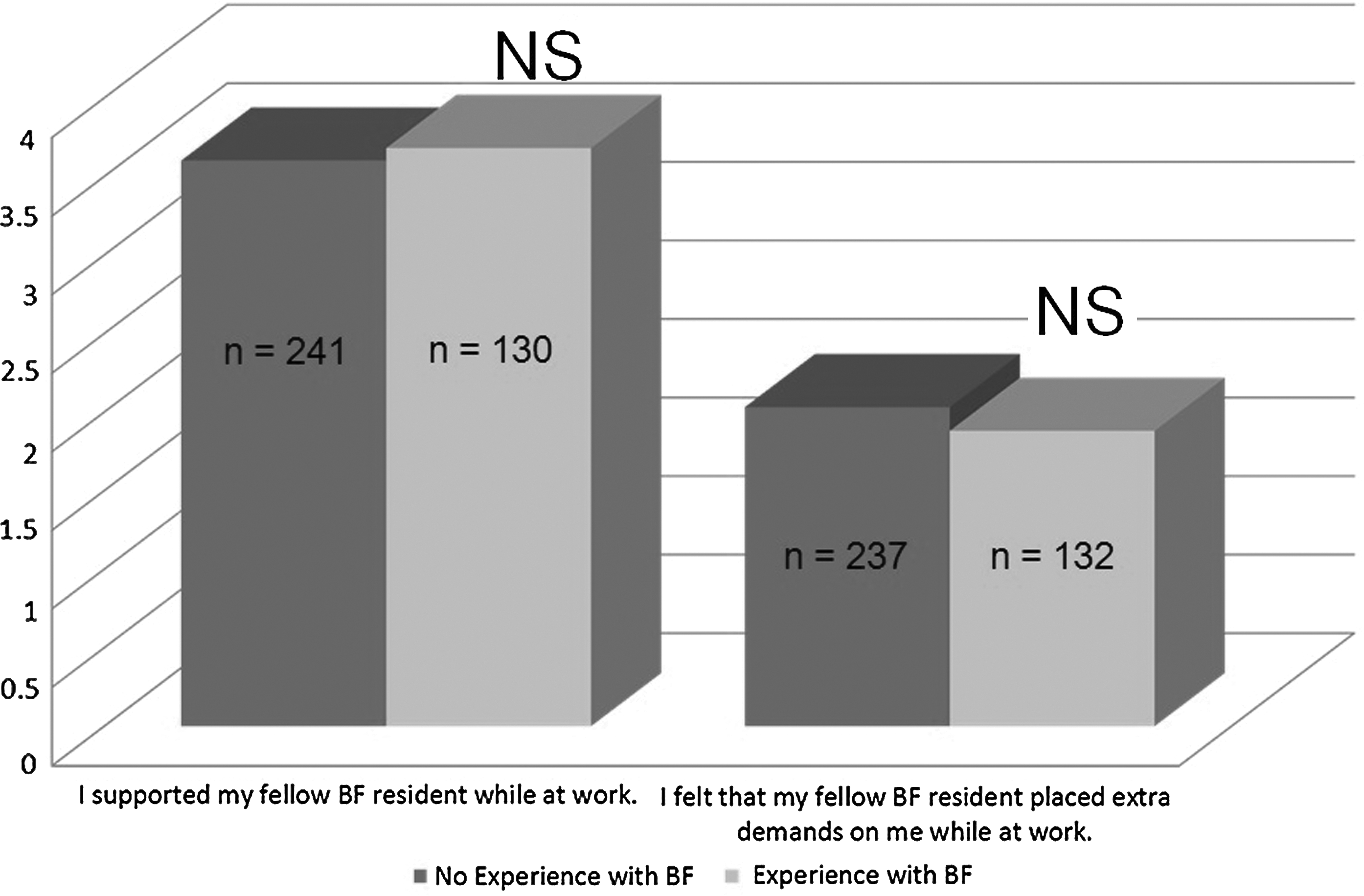
Support given and burden felt by residents based on breastfeeding (BF) experience. There was no significant difference in the support given or burden felt by fellow residents based on past experience with breastfeeding. The y-axis is a Likert 4-point scale, with 4=strongly agree, 3=agree, 2=disagree, and 1=strongly disagree. p<0.05, significant difference; NS, not significant.

Expectations for pumping during being on-call based on breastfeeding (BF) experience. There was no significant difference in the number of times a resident thought a mother should pump in 12–16 hours or a 24-hour period based on past experience with breastfeeding. The y-axis is the number of times there was a need to pump in the given time period. p<0.05, significant difference; NS, not significant.
Suitable places to pump were elicited from mother and colleague residents. In general, places in view of public or patients were discouraged because of professionalism concerns. Most mother residents felt they needed a private place to pump (73%). Call rooms were popular suggestions for places to pump. Other suitable places to pump included a lactation room, office, empty patient room, and bathrooms. Conferences and board checkout received mixed reviews on suitability depending on resident preference due to perceived “hard to hear” or “lack of privacy” issues, but there were no differences in perceived suitability from residents with and without breastfeeding experience.
Discussion
Breastfeeding is common during obstetrics and gynecology residency. One out of four female residents had experience with breastfeeding during residency, and 90% of all residents knew a breastfeeding colleague. Residents with breastfeeding experience were older, further along in obstetrics and gynecology training, more likely to be married, and less likely to plan to do a fellowship than residents without breastfeeding experience.
In general, breastfeeding residents felt that program directors, faculty, and fellow residents were supportive of their decision to breastfeed and felt that they were successful in meeting both residency and breastfeeding goals. Despite high levels of support, many residents struggled with low milk supply and work demands, with three out of four residents discontinuing breastfeeding early. Rates of breastfeeding were encouraging for this study population as more than 52% of residents were still breastfeeding at 6 months postpartum but still fell short of the Healthy People 2020 recommendations for 60%. 1
It is interesting that mother residents felt they placed extra demands on colleague residents to achieve breastfeeding goals, but generally their colleagues did not report feeling that extra demands had been placed upon them. This may be the eternal debate of “mother guilt” or even “resident guilt” when one feels they are not contributing as much because they leave the workplace for a brief time. Mothers also felt guilty about time spent away from their children. It would be curious to assess level of guilt or perception of burden placed on others with long-term breastfeeding rates. A study by Cole et al. 13 on otolaryngology residents demonstrated that guilt and stress are mitigated by program directors using preemptive policies on maternity leave, call issues, and flexible rotation schedules.
Colleague residents (98%) supported breastfeeding residents regardless of the colleagues' previous experience with breastfeeding. Colleague residents generally did not feel that mother residents were placing extra demands on them. This study did not specifically ask about resentment, nor was it reported in open-ended questions. In a previous study, resentment among ear nose and throat residents was mitigated by designing flexible research blocks in which individual study was emphasized. Fears that pregnant residents would have fewer surgical cases by introduction of flexible rotations were allayed by demonstrating no difference in total surgical numbers between pregnant residents and their colleagues. 14 The number of times expected to pump during call shifts was not different between groups with and without experience with breastfeeding, suggesting realistic expectations of colleagues. A study to assess policies to support reasonable breaks for breastfeeding mothers may help to mitigate resentment in colleague residents and relieve stress in maternal residents and would be a worthwhile future study, but clearly this was not a focus of the current study. A policy of supporting breastfeeding was considered important by 85% of residents, but only 7% believed their program had such a policy. Our study did not specifically address with survey questions the 2010 Affordable Care Act Section 4207 breastfeeding law, which requires employers to provide reasonable break time and a private, non-bathroom place for nursing mothers to express breastmilk during the work day, for 1 year after the child's birth. This new requirement became effective when the Affordable Care Act was signed into law on March 23, 2010. Given the requirements of the law, residency coordinators may be more willing to adopt a specific breastfeeding policy for their program.
Both maternal and colleague residents offered opinions on where to pump during residency, with most agreeing that a private place is best. Call rooms and lactation rooms were popular suggestions. Outpatient rotations required more creativity in using empty patient rooms or offices. In general, residents were mixed about pumping in public because of distraction during conferences or the chance that patients might perceive the pumping as unprofessional. Policies should be developed to allow breastfeeding residents access to breaks and private places for the optimal scenario when returning to work (see a sample breastfeeding policy in Fig. 3). A reasonable number of breaks might be considered three or four times in a 12–16-hour period and six or seven times in a 24-hour period, which were the averages suggested by both maternal and colleague residents in this study. In addition, 75% of maternal colleagues felt successful in meeting breastfeeding goals based on the number of pumping or breastfeeding sessions above. The exact number of sessions will vary but can be expected to fall in the ranges above and can be determined by the pattern that mothers breastfed in the first few weeks postpartum. 15
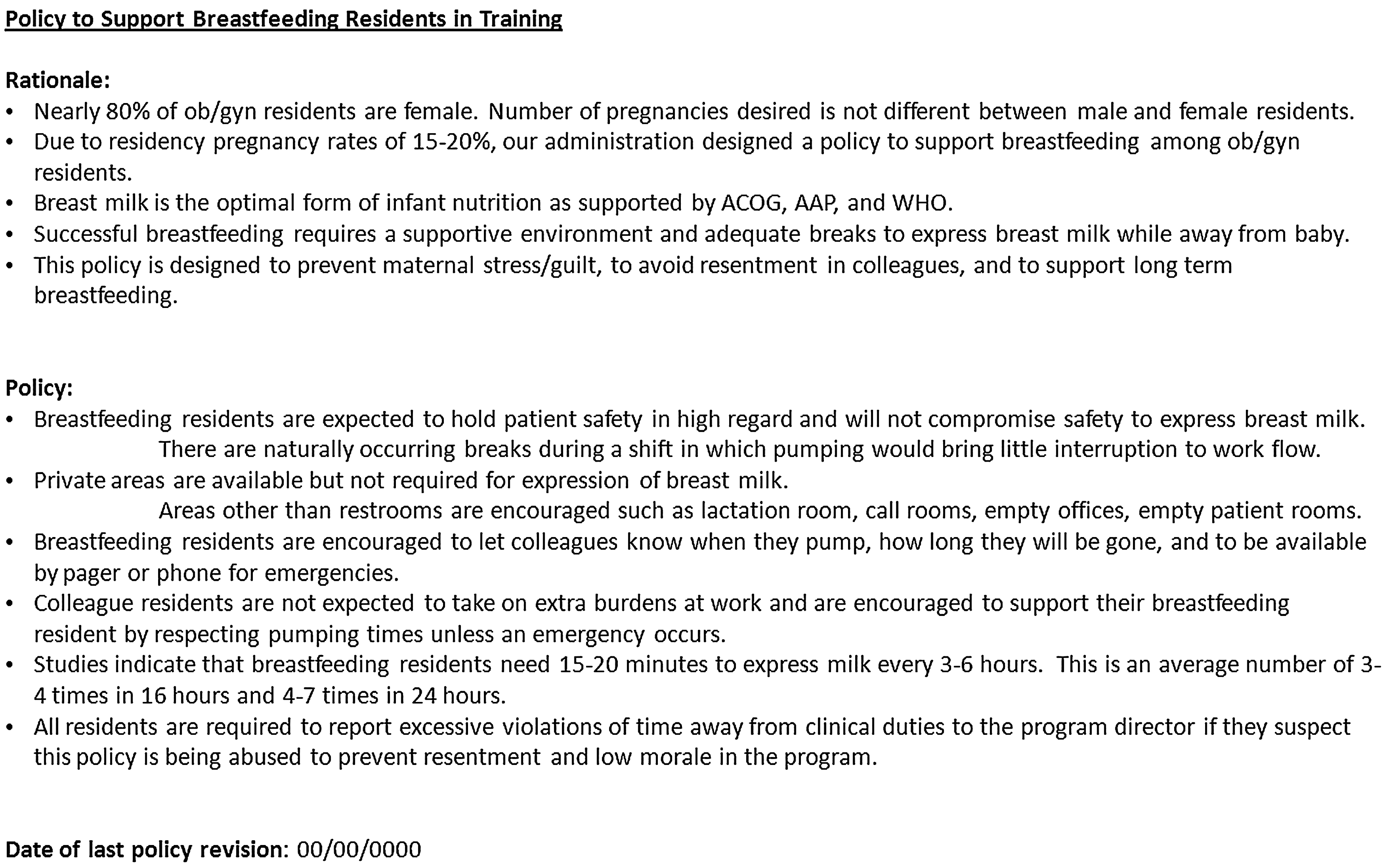
Sample breastfeeding policy for obstetrics and gynecology residency programs. Breastfeeding policies should consider emphasizing patient safety, long-term breastfeeding rates, and prevention of resentment or low morale in residents. General guidelines on expected time needed to breastfeed or pump are supported by this study. AAP, American Academy of Pediatrics; ACOG, American College of Obstetrics and Gynecology; WHO, World Health Organization.
Strengths of this study include that the data and information have not previously been reported (MEDLINE; 1946–May 2012; English language; search terms of “ob,” “residency,” and “breastfeeding”) for obstetrics and gynecology residency programs and may help to provide information to shape policy for program directors in relation to residents, both mothers and colleagues. The data may also help residents considering or planning a pregnancy during residency to become familiar with potential pitfalls in breastfeeding during residency and to help set realistic expectations about breaks and colleague support. This is a comprehensive and cross-sectional review of current breastfeeding practices of mother residents in obstetrics and gynecology residencies. This review also focuses on colleague resident perceptions on breastfeeding in obstetrics and gynecology residency, which are lacking in the current literature (MEDLINE; 1946–May 2012; English language; search terms of “colleague” or “coworker,” “breastfeeding,” and “ob”).
Supporting residents to breastfeed optimally may translate to improve community rates as physician experience has been linked to promotional practices toward patients. 2 This study addresses practical questions on how best to support breastfeeding residents such as expectations on where to pump, how often to pump, and how well supported these residents felt by faculty and peers. Practical questions may help other mothers in demanding job settings to apply these practices to improve breastfeeding success. Future studies could evaluate these practical suggestions and monitor breastfeeding rates before and after implementation. It is hypothesized that implementation of a policy with expectations would improve communication between colleague residents and breastfeeding residents and would likely mitigate feelings of guilt and resentment. Testing levels of guilt and resentment in residents before and after institution of a breastfeeding policy would help to explore this hypothesis. The data from this study indicate that additional studies on maternal guilt and level of success with breastfeeding might be beneficial.
Strengths of this study include savings in time, cost, and resources by administration in an online and self-paced questionnaire. This study also met power requirements, and the survey instrument was validated prior to initiation of the survey to improve the quality and meaning of the responses obtained.
Although the study has many strengths, there are several limitations that may have threatened internal and external validity. Limitations include that this is a cross-sectional study and is subject to recall bias in the responses of both mother and colleague residents. Response bias is inherent in any survey, and it is difficult to know if the non-responding and responding populations are representative of the population without performing a costly and time-laden survey of non-responding residents. It is likely that residents interested in breastfeeding were attracted to the study design and preferentially answered survey questions. However, demographic data were similar to national norms in reference to gender and age for obstetrics and gynecology residents. Despite using a gift card as an incentive, the response rate was low, likely because of multiple survey requests of residents during the same time period and time constraints. There was another breastfeeding survey e-mailed to residents the same month. In addition, there were survey requests of residents on robotics, clinics, and perception of work hours in the same 6 months as the request to participate in this survey. The survey responses were solicited twice with minimal response after the second e-mail. In retrospect, it would have been beneficial to track survey responders and determine what program they were from or at least their geographic location and program size to help determine if there was a systematic exclusion of residents from a particular program or region. For instance, program coordinators may not have forwarded the survey onto their residents, which may have limited the actual pool of eligible participants or may have excluded programs that were not receptive to breastfeeding residents. The low response rate (6%) indicates that actual groups may be different from this sample of residents, and further assessment may be needed to verify this information with a larger sample in future studies. Indeed, many surveys avoid low response rates by using program directors or by focusing on one institution to ensure return of surveys. One study targeting obstetrics and gynecology residents to evaluate opinions on training in female sexual dysfunction had 234 responses of third and fourth year residents, which is a 10% response rate, had a similar study design with an online survey instrument with a national sample size, and re-issued the survey two times; the only difference in methodology with our study was that researchers called the 250 residency coordinators to ensure they had received the survey and forwarded it onto residents. 16
Resident opinions may not reflect written policies. Specific support measures such as flexible schedules and policies were not delineated in this study but have previously been explored. 13 The generalizability of these results to other specialties outside of obstetrics and gynecology is limited. Future studies can address colleague perception of resentment and maternal perception of guilt.
Conclusions
As more women enter residency, challenges for residents to determine optimal timing of pregnancy will become more complex. In addition, work hour restrictions and the increased age of women entering medical school and residency are potentially contributing factors to the increased age of childbearing and need for support with breastfeeding during residency. Program directors will need to determine how best to balance education and patient care with supporting parents. Certainly, pregnancy and breastfeeding during residency are becoming more common. There is a need to balance privacy and breaks for breastfeeding residents with the desire to prevent resentment and low morale of colleagues. These experiences suggest that breastfeeding can be successful with minimal burden on colleague residents. Mother residents should be aware that low milk supply is common. In general, faculty and fellow residents are supportive of breastfeeding residents. Flexible solutions to return to work and addressing breastfeeding with a policy may help to reduce mother residents' sense of guilt and stress and reduce resentment of colleagues. Overall, mother residents were successful in meeting personal residency and breastfeeding goals but did discontinue breastfeeding earlier than desired or recommended by the Healthy People 2020.
Footnotes
Acknowledgments
This study was supported by funding from the Maricopa Medical Foundation. We acknowledge Dean Coonrod, MD, MPH, Chair, Department of Obstetrics and Gynecology, Maricopa Integrated Health System, Phoenix, AZ, for his editorial assistance in preparation of the manuscript. Dr. Coonrod received no compensation for his editorial review of the manuscript.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.