
Abstract
Abstract
Background and Objective:
Until 2010, newborns at our institution were bathed in the nursery at approximately 2 hours of life. In May 2010, infant baths were delayed until at least 12 hours of life. Infants are now bathed in the hospital room with parents' participation and are placed skin-to-skin immediately after the bath. This study explored whether delaying the newborn's first bath correlates with increased in-hospital breastfeeding rates at our Baby-Friendly, urban safety-net hospital.
Subjects and Methods:
We performed a retrospective chart review comparing in-hospital breastfeeding rates during the 6 months before and the 6 months after the bath was delayed.
Results:
Of the infants, 702 met inclusion criteria. Before the bath was delayed, infants were bathed at an average of 2.4 hours of life. Afterward, infants were bathed at an average of 13.5 hours of life. In-hospital exclusive breastfeeding rates increased from 32.7% to 40.2% (p<0.05) after the bath was delayed. Multivariate logistic regression analysis showed that infants born after implementation of delayed bathing had odds of exclusive breastfeeding 39% greater than infants born prior to the intervention (adjusted odds ratio [AOR]=1.39; 95% confidence interval [CI] 1.02, 1.91) and 59% greater odds of near-exclusive breastfeeding (AOR=1.59; 95% CI 1.18, 2.15). The odds of breastfeeding initiation were 166% greater for infants born after the intervention than for infants born before the intervention (AOR=2.66; 95% CI 1.29, 5.46).
Conclusions:
In our cohort, a delayed newborn bath was associated with increased likelihood of breastfeeding initiation and with increased in-hospital breastfeeding rates.
Introduction
T
The Healthy People 2020 goals for breastfeeding rates establish a target of 81.9% breastfeeding initiation and 25.5% exclusive breastfeeding through the first 6 months of life. 8 Data from the Centers for Disease Control and Prevention's 2011 Breastfeeding Report Card show, however, that only 12 states have attained the target rate of breastfeeding initiation, and only two have attained the target rate for exclusive breastfeeding at 6 months. 9
Recent quality improvement efforts have prioritized the promotion of maternity practices that foster breastfeeding during the postpartum stay. These practices include minimizing separation between mothers and infants, increasing time spent skin-to-skin, eliminating pacifiers, and giving supplemental formula only when medically necessary. Long established as part of Baby-Friendly practice, these simple interventions have been shown to increase in-hospital breastfeeding rates. 10 New evidence demonstrates that these practices are also associated with longer duration of breastfeeding after hospital discharge.11,12
Despite the promise of improving breastfeeding rates simply through modification of maternity practices, widespread implementation of these innovations has lagged. In 2007, the Centers for Disease Control and Prevention undertook its first biannual Maternity Practices in Infant Nutrition and Care (mPINC) survey, which allows U.S. maternity facilities to score themselves based on adoption of maternity practices that promote breastfeeding. Results from the 2009 mPINC survey, reflecting scores submitted by more than 2,500 maternity facilities nationally, revealed a disappointing average score of 65 points out of a possible 100. 13 In the context of this quality gap, the Joint Commission identified the exclusive breastfeeding rate at discharge as one of five quality measures in its 2010 Perinatal Care Core Measure Set, which gauges hospital implementation of optimal maternity practices. 14
Many maternity routines that hamper breastfeeding, such as formula supplementation or separation of mothers and infants, are easily identified. Other aspects of routine maternity care, such as the timing of the first bath, have not been studied for their potential impact on breastfeeding rates. At our institution, the impetus for delaying the first bath was the result of analyzing our mPINC score for areas in which we could improve our maternity care to enhance breastfeeding support. We hoped both to decrease maternal–infant separation and to increase exclusive breastfeeding rates. We discussed delaying the bath with colleagues from other Baby-Friendly Hospitals and identified this intervention as a possible route to achieve both of these goals. As delaying the bath was being considered, we underwent a redesign of our unit that created private rooms for all of our patients and allowed us to install sinks that were specially designed for bathing newborns. In May 2010, we changed our newborn care protocol to delay the infant's first bath until at least 12 hours of life. Ours is the first study to examine the impact of delaying the infant's first bath on in-hospital breastfeeding rates.
Subjects and Methods
Prior to implementation of the delayed bath, newborns in our hospital were bathed at approximately 2 hours of life, or later if the neonate had yet to achieve a stable temperature. Nurses bathed infants in the newborn nursery, usually while parents were in the hospital room or surgical recovery area. Infants were sponged clean while still on the warmer. They were then wrapped in a blanket, and their hair was washed under a running faucet. Then infants were dried, wrapped in dry blankets, and placed under the radiant warmer. Under the new protocol, the bath is given after 12 hours of life. Infants are bathed by a nurse or patient care assistant in the sink in the hospital room. Parents participate in bathing the infant, and after the bath, infants are dried and placed skin-to-skin under dry blankets with their mother, father, or another family member.
We conducted a retrospective chart review of infants born at Boston Medical Center (Boston, MA) from November 1, 2009, through October 31, 2010, 6 months before and 6 months after our bathing protocol changed. The study received Boston University Medical Campus Institutional Review Board approval. Boston Medical Center is an urban safety-net teaching hospital affiliated with the Boston University School of Medicine. Patients primarily are low-income, ethnic minorities and medically underserved. In 1999, Boston Medical Center was certified as a Baby-Friendly Hospital, making it one of only 154 U.S. maternity facilities currently having earned this designation as of January 2013. 15
Our primary inclusion criteria were admission to the well infant nursery and eligibility to breastfeed. Infants were excluded because of the following maternal factors: human immunodeficiency virus infection, illicit drug use, or any other contraindication to breastfeeding as identified by the American Academy of Pediatrics. 1 We additionally excluded infants whose mothers were admitted to the intensive care unit after delivery. We also excluded infants who were initially admitted to the nursery but then transferred to the neonatal intensive care unit because of illness. We then performed a detailed review of the chart of every third infant identified sequentially in the unit's admission database. An infant who did not meet inclusion criteria was replaced by the infant immediately following him or her in the database. Maternal and infant information was obtained from the infant admission note and the infant's Labor and Delivery transfer summary. From this group of eligible-to-breastfeed infants, we then excluded those who were born after the delayed bath was implemented but were not eligible for the delayed bathing protocol, specifically infants born to mothers with hepatitis B, hepatitis C, active herpes simplex virus infection, and methicillin-resistant Staphylococcus aureus. We also excluded infants whose parents had requested an early bath or who had their bath delayed for another reason (Fig. 1).
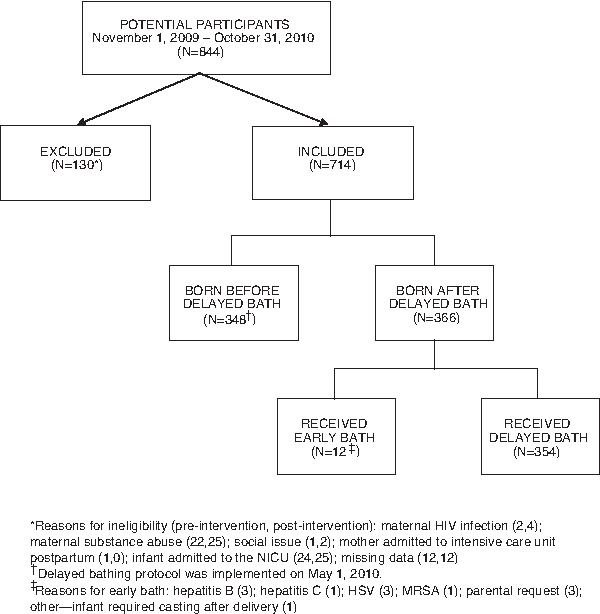
Sample selection method for study participants. HIV, human immunodeficiency virus; HSV, herpes simplex virus; MRSA, methicillin-resistant Staphylococcus aureus; NICU, neonatal intensive care unit.
We defined exclusive breastfeeding as having received no formula, water, or glucose water during the birth hospitalization. Infants who received at least one formula feed, even for a medical indication, were defined as not being exclusively breastfed. Near-exclusive breastfeeding was defined as having from 90% to <100% breastmilk feeds. Breastfeeding initiation was defined as having been breastfed at least once. Breastfeeding categories were determined by a feed-by-feed review of bedside charts, which contain a record of every documented feed that an infant receives during his or her hospital stay. These charts also record the time of the bath.
Bivariate tests of association between the predictor variable (intervention vs. control group status) and each outcome (breastfeeding status) variable were performed using χ2 tests. We used multivariate logistic regression analyses to test for differences in odds of breastfeeding before and after the intervention while controlling for potential confounding factors (maternal age, race/ethnicity, type of insurance, mode of delivery, infant gestational age, and birth weight status). Analyses were performed using STATA version 12 (StataCorp LLC, College Station, TX). All tests of statistical significance used α<0.05.
Results
In total, 714 mother–infant dyads met inclusion criteria. Characteristics of infants and mothers were similar before and after the intervention, with the exception of maternal race (Table 1). Before implementation of the delayed bathing protocol, infants were bathed on average at 2.4 hours of life. After initiation of delayed bathing, infants were bathed on average at 13.5 hours of life. No adverse effects—such as a post-bathing temperature low enough to require a pediatrician to evaluate the infant or to necessitate the use of the radiant warmer—were reported. The parents of only three infants refused a delayed bath.
Some percentages may not add to exactly 100% because of rounding.
Middle Eastern is not a United States Census Bureau category but one that patients may choose to self-identify when registering at our hospital.
Exclusive breastfeeding rate increased from 32.7% in the 6 months before the intervention to 40.2% in the 6 months after the intervention (p<0.05). In our sample, infants born after implementation of the “Delay the Bath Intervention” had odds of exclusive breastfeeding 39% greater than infants born prior to the intervention (adjusted odds ratio [AOR]=1.39; 95% confidence interval [CI] 1.02, 1.91). Babies born after the “Delay the Bath Intervention” had odds of near-exclusive breastfeeding, defined as from 90% to <100% of feeds with breastmilk, 59% greater than those born before the intervention (AOR=1.59; 95% CI 1.18, 2.15). The odds of breastfeeding initiation (i.e., of the infant receiving any breastmilk at all during his or her neonatal hospital stay) were 166% greater for infants born after the intervention than for those born before the intervention (AOR=2.66; 95% CI 1.29, 5.46) (Table 2). This result demonstrates that the likelihood of an eligible-to-breastfeed infant being exclusively formula fed was significantly lower after the intervention than before.
AOR, adjusted odds ratio (adjusted for mother's race/ethnicity, mother's age, mode of delivery, low birth weight, high birth weight, and insurance type); CI, confidence interval.
Discussion
Our results suggest that delaying the newborn bath until 12 hours of life can positively affect both breastfeeding initiation and exclusivity. An early first bath is a maternity routine so ubiquitous as to go practically unnoticed, yet its implications for infant care are profound. Changing this long-standing practice correlated with increased rates of both exclusive and near-exclusive breastfeeding in our sample. At the same time, delayed bathing opened the door for increased breastfeeding initiation. This is especially meaningful for our predominantly poor and minority patient population, who unequally bear the burden of breastfeeding disparities.
There is no prior literature on the association between delayed bathing and short- or long-term changes in breastfeeding rates. Nevertheless, related data suggest several non-mutually exclusive mechanisms by which delaying the bath may affect an infant's ability to breastfeed successfully. These include decreasing the risk of hypothermia and hypoglycemia that accompanies an early bath, decreasing maternal–infant separation, and allowing infants to spend more time skin-to-skin with their mothers.16–24
Neonates are physiologically more vulnerable than adults to hypothermia because of their relatively larger surface area and tendency to lose heat more rapidly. Neonates are also prone to hypoglycemia immediately after birth because in the absence of maternally supplied glucose, infants must rely on liver glycogen stores for gluconeogenesis. Additionally, a hypothermic newborn can quickly become hypoglycemic as the physiologic response to hypothermia taxes the infant's glycogen reserves. 16 Hence, the nature of newborn physiology suggests that early bathing may be a stressful experience that could lead to hypothermia, hypoglycemia, or both, which in turn could hamper an infant's ability to breastfeed.
The effect of timing of the infant's first bath on body temperature has been studied. Penny-MacGillivray 17 compared rectal temperatures of infants bathed at 1 hour and at 4 hours after delivery and found no significant difference in mean temperatures between the groups during the 2 hours after bathing; there was, however, a significant difference between the two groups in mean temperature change from before to after the bath. Infants bathed at 1 hour of life had a significantly greater decrease in temperature from before to after the bath than those bathed at 4 hours of life. It is notable that all infants studied, regardless of whether bathed at 1 or 4 hours of life, experienced a decrease in temperature. 17 Similarly, in a study by Varda and Behnke 18 comparing body temperature of infants bathed at 1 hour of life versus 2 hours of life, no significant difference was found between the two groups, but body temperatures in all participants were significantly lower after bathing.
The question of whether infants should be bathed by nurses under a radiant warmer, as is the standard of care in many institutions, compared with having parents administer the bath, has been addressed in a randomized controlled trial by Medves and O'Brien. 19 Infants in this trial were bathed between 2 and 5 hours of life and were randomized to being bathed by nurses per nursery routine or by parents in the hospital room. As in prior studies, infant temperature decreased significantly during bathing in both the control and the intervention groups. Infants bathed by parents lost an average of 1.2°C, whereas infants bathed by nurses lost an average of 1.5°C, a statistically significant difference. 19
Taken together, these studies indicate that when infants are bathed in the first hours of life, whether as early as 1 hour or as late as 5 hours, core body temperature decreases. Because of reduced thermoregulatory capacity in neonates, lowering body temperature even by 1°C represents a significant change and could contribute to impaired breastfeeding behavior as infants bathed in the first hours of life mobilize metabolic resources to reestablish temperature homeostasis.
Protecting infants from mild iatrogenic hypothermia by delaying their first bath may be an important factor contributing to improved breastfeeding behaviors; preventing early separation of mothers and infants may be another. The benefits of allowing early contact between mothers and infants for breastfeeding have been demonstrated in several studies in different settings. 20 In keeping with Baby-Friendly practice, our previous protocol allowed infants to be bathed after spending as much as 2 hours with their mother in Labor and Delivery. Nevertheless, when we delayed the bath to 12 hours of life, we eliminated a period of early maternal–infant separation that had previously been a fixed part of newborn care.
Delaying the bath prevents a period of early separation; it also incorporates an extended period of skin-to-skin contact into routine well-infant care. Skin-to-skin contact has been shown to have multiple benefits for infants. In a recent study, Bramson et al. 21 showed a dose–response relationship between time spent skin-to-skin in the first 3 hours of life and the likelihood of exclusive in-hospital breastfeeding. Additionally, skin-to-skin contact has been associated with decreased infant crying.22–24 Reduced crying in turn decreases parental perception of hunger and removes a powerful trigger for unnecessary formula supplementation. Finally, skin-to-skin contact has been shown to protect against hypothermia and hypoglycemia. 23 At our hospital, we emphasize skin-to-skin as part of our Baby-Friendly practice, including placing infants skin-to-skin in Labor and Delivery. Until our bathing protocol was changed, however, infants were not being placed skin-to-skin immediately after their bath, a time at which infants are highly likely to benefit from this intervention.
In summary, we believe that implementation of a delayed bathing protocol correlated with improved breastfeeding rates in our sample because of three interrelated factors. First, as noted above, bathing the infant at 12 hours of life may attenuate the risk of hypothermia and hypoglycemia to which the hours-old neonate is more vulnerable. Additionally, as discussed previously, decreasing mother–infant separation and increasing skin-to-skin time are key elements of our Baby-Friendly practice that predate the “Delay the Bath Initiative.” At the same time, however, the process of delaying the bath necessarily decreased maternal–infant separation and increased time spent skin-to-skin. These changes, which are organic to our delayed bathing protocol, may have had a synergistic effect on the breastfeeding rates in our sample.
Our study has several limitations, the greatest of which is the possible erroneous attribution of increased breastfeeding rates to a single intervention, delayed bathing. In considering whether other aspects of our maternity care had changed significantly over the 12 months during which we studied our breastfeeding rates, however, we are unable to identify any other major changes in protocols or procedures. It is also possible that the timing of the bath is only a proxy for decreased separation and increased time spent skin-to-skin, which may independently have been responsible for the measured improvement in breastfeeding rates. Because of the retrospective nature of our study, we were not able to quantify the time spent skin-to-skin or time that mothers and infants were separated because these data were not recorded in infants' charts. Finally, although our unit redesign created a more comfortable environment for bathing infants in their rooms, delayed bathing can be instituted in any maternity setting, and changes in physical plant are not a necessary prerequisite to delayed bathing.
Conclusions
In our sample, delaying the bath by at least 12 hours was associated with statistically significant increases in rates of breastfeeding initiation and exclusive and near-exclusive breastfeeding at our Baby-Friendly hospital. These positive outcomes were achieved through an easily implemented, cost-neutral intervention that was offered to all eligible newborns regardless of maternal intent to breastfeed. Our study is the first to demonstrate that delaying the infant's first bath correlates positively with improved rates of breastfeeding initiation and exclusivity. Delayed bathing may represent another component of optimized maternity practice that supports improved in-hospital breastfeeding rates.
Footnotes
Acknowledgments
We would like to acknowledge the staff of the Birth Place at Boston Medical Center for their remarkable ongoing commitment to improving breastfeeding outcomes for our patients.
Disclosure Statement
No competing financial interests exist.