
Abstract
Abstract
Objective:
A study was made of the influence of breastfeeding and bottle feeding on development of the dental arches and occlusion in an infant population.
Subjects and Methods:
In total, 298 infants (163 girls and 135 boys) were selected from a series of 1,643 preschool children in Seville, Spain, evaluating the type of feeding received after birth (breastfeeding only or bottle feeding only), the duration of such feeding, and its influence upon the parameters that define occlusion of the dental arches. The study comprised a full exploration of the stomatognathic system of the infants and a questionnaire for the parents. SPSS Statistical Package software (SPSS, Inc., Chicago, IL) was used to analyze the results.
Results:
In total, 109 children were exclusively breastfed (36.6%) for an average of 6.8±5.8 months, whereas 189 children were exclusively bottle fed (63.4%) for an average of 17.99±11.5 months. On comparing the occlusal parameters of the two groups, the most beneficial effects (straight terminal plane, canine class I relationship, diastemas, and primate spaces) corresponded to the infants who were breastfed.
Conclusions:
Breastfed infants show better development of the dental arches and a lesser incidence of dental occlusion disorders than bottle-fed infants.
Introduction
B
Other authors have indicated that breastfeeding could be associated with fewer occlusal anomalies11,12 because it favors correct growth of the upper maxilla and the dental arches. This is not the case in bottle-fed infants because the orofacial muscles that intervene in the two feeding modalities differ. 13 However, it should be remembered that the development of the craniofacial complex (mandible, dental arches, tongue, facial muscles) is not only dependent on environmental factors but is also influenced by genetic factors and their interactions.9,14–16
Because occlusal development is conditioned by a range of factors, it is not easy to evaluate the influence of isolated factors. Most studies center on the effects of non-feeding suction habits (dummy, thumb sucking) upon the temporal dentition17–19 and their relation to certain malocclusions such as open bite, overjet, or crossbite,17,20 but they do not separately relate breastfeeding or bottle feeding to the parameters that define correct occlusion. With the purpose of exploring and comparing the direct impact of the two feeding modalities on these parameters, we have carried out a study in preschool children in Seville, Spain—eliminating those additional factors that may influence the results, such as the aforementioned non-feeding suction habits.
We believe correct occlusion of the temporal dentition to be essential for preventing and reducing occlusal problems in the permanent dentition. In this context, we consider it the responsibility of healthcare professionals to underscore the importance of breastfeeding for correct dental arch positioning and dental occlusion, thereby contributing to improvement of patient quality of life and lessening the costs associated with the treatment of malocclusions.
Subjects and Methods
The study selected a total of 1,643 preschool children in 18 nurseries existing in six municipal health districts in the metropolitan area of Seville, representative of the different socioeconomic levels (lower, middle, and upper).
The following inclusion criteria were used: exclusive breastfeeding or bottle feeding (infants with mixed breastfeeding and bottle feeding were excluded); no bad oral habits (dummy, thumb sucking); age from 3 to 6 years (temporal dentition); enrollment in the nurseries included in the study; parents having completed the patient questionnaire; and absence of oral or systemic conditions capable of influencing the results. Of the total sample, 298 preschool children (18.14%) satisfied all these criteria.
The study made use of the material commonly used for oral and dental exploration, and an analysis was made of the occlusal parameters in the three spatial planes, the existence of interdental spaces, and the presence of crowding.
In the anteroposterior plane of the dental arches we analyzed the following:
• Canine relationship or the form of occlusion of the upper and lower canines. Three forms of occlusion were considered: class I, in the case of correct occlusion; class II, when the upper canines were advanced with respect to the lower canines; and class III, when the lower canines were advanced with respect to the upper canines. • Terminal plane or the form of occlusion of the temporal second molars: straight terminal plane; mesial step (the upper molar lies anterior to the lower molar); or distal step (the lower molar lies anterior to the upper molar). • Overjet or the separation of the upper and lower incisors in the anteroposterior plane.
In the transversal plane we analyzed the following: posterior crossbite, this is, the external cuspids (vestibular) of the upper premolars and molars occlude internal to the fossae of the lower premolars and molars; in temporary dentition, we talk about a posterior crossbite when maxillary posterior teeth occlude inside mandibular teeth. These crossbites can affect the two upper hemiarches (bilateral posterior crossbite), a single hemiarch (right or left unilateral posterior crossbite), and even one or several teeth.
In the sagittal plane we analyzed the following: open bite (i.e., in the vertical plane there is a lack of contact of one or more teeth of an arch with the corresponding antagonists) and overbite (i.e., the upper incisors completely cover the lower incisors).
The presence or absence of interdental spaces in the arches was assessed according to the following: interincisal diastemas (separation between the temporal incisors); primate spaces (physiological spaces between the lateral incisors and the upper canines and between the canines and the lower first molars); and dental crowding.
The parents in turn received a questionnaire addressing the type of feeding the infant had received (breastmilk or bottle), whether feeding was of one type only or mixed (alternated), the time for which each feeding modality had been used, and whether the child presented bad oral habits.
SPSS Statistical Package software (SPSS, Inc., Chicago, IL) was used for the analysis of the results. A full descriptive analysis was done, comprising the following variables: gender; age; breastfeeding or bottle feeding and its duration, based on the categories of only breastfeeding or only bottle feeding; the duration of feeding, divided into the three groups of only breastfeeding or only bottle feeding up until 6 months of age, between 6 and 18 months of age, and over 18 months of age; and the oral repercussions of breastfeeding or bottle feeding based on the series of dental parameters of terminal plane, canine occlusion, incisor occlusion, crossbite (right, left, and bilateral), diastemas (anterior and posterior), primate spaces, and crowding (anterior and posterior).
There were no significant gender or age differences among the different groups. Comparisons were made based on the χ2 test in the case of qualitative variables and using analysis of variance in the case of quantitative variables exhibiting a normal distribution, whereas the Kruskal–Wallis test was used in the presence of a non-normal distribution. In all cases a 95% confidence level was accepted.
Results
Of the 1,643 preschool children initially subjected to screening, 298 (163 girls and 135 boys) met all the study inclusion criteria. The age distribution was as follows: 12 subjects were 3 years old, 103 subjects were 4 years old, 158 subjects were 5 years old, and 25 subjects were 6 years old. Regarding the type of feeding, 109 children (36.6%; 53 girls and 56 boys) received only breastfeeding, whereas 189 children (63.4%; 110 girls and 79 boys) received only bottle feeding.
In relation to the duration of breastfeeding, over one-half of the children were breastfed for a maximum of 6 months (Fig. 1). In contrast, most of the bottle-fed infants received this type of feeding for between 6 and 18 months (Fig. 2).
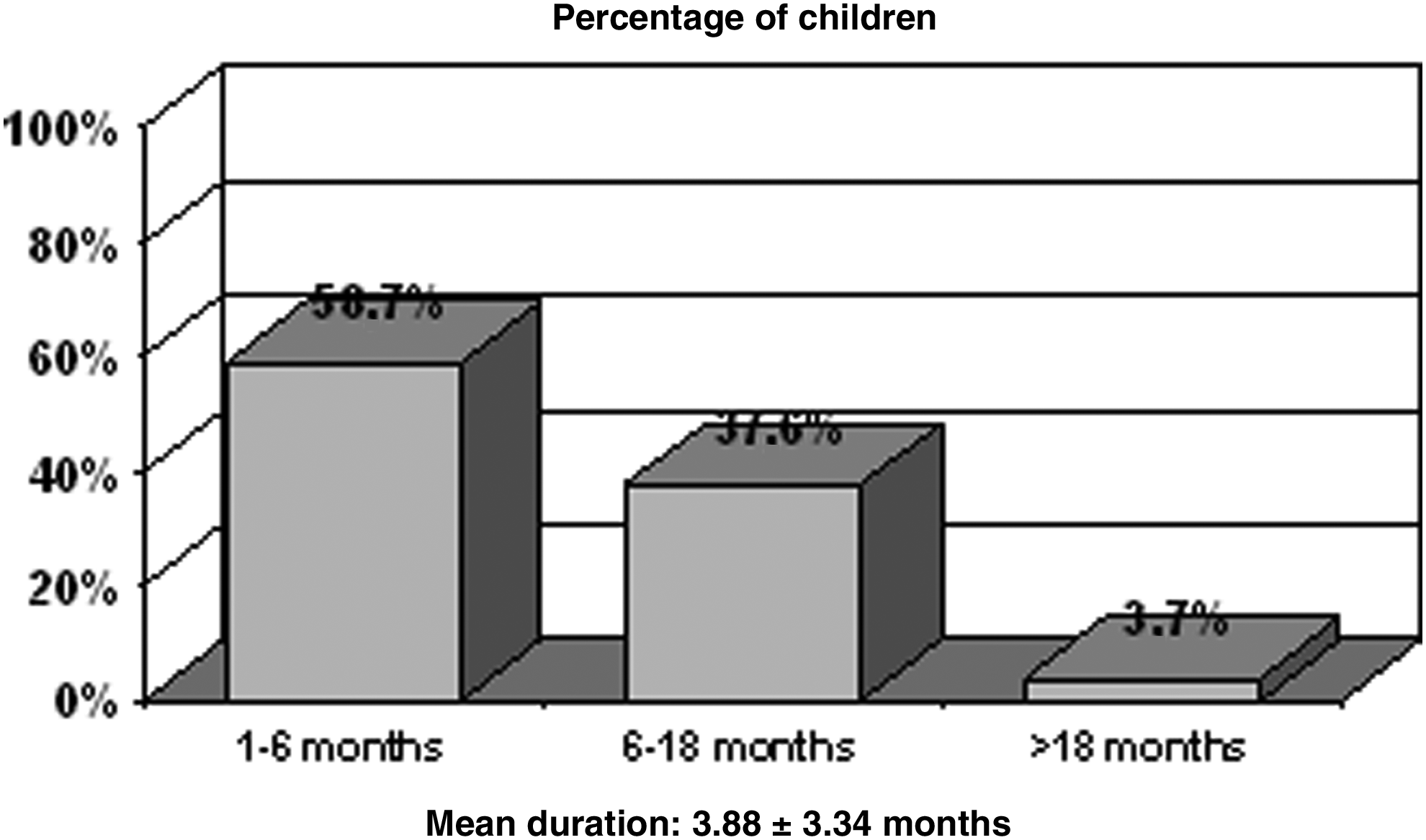
Duration of breastfeeding (mean duration, 3.88±3.34 months).
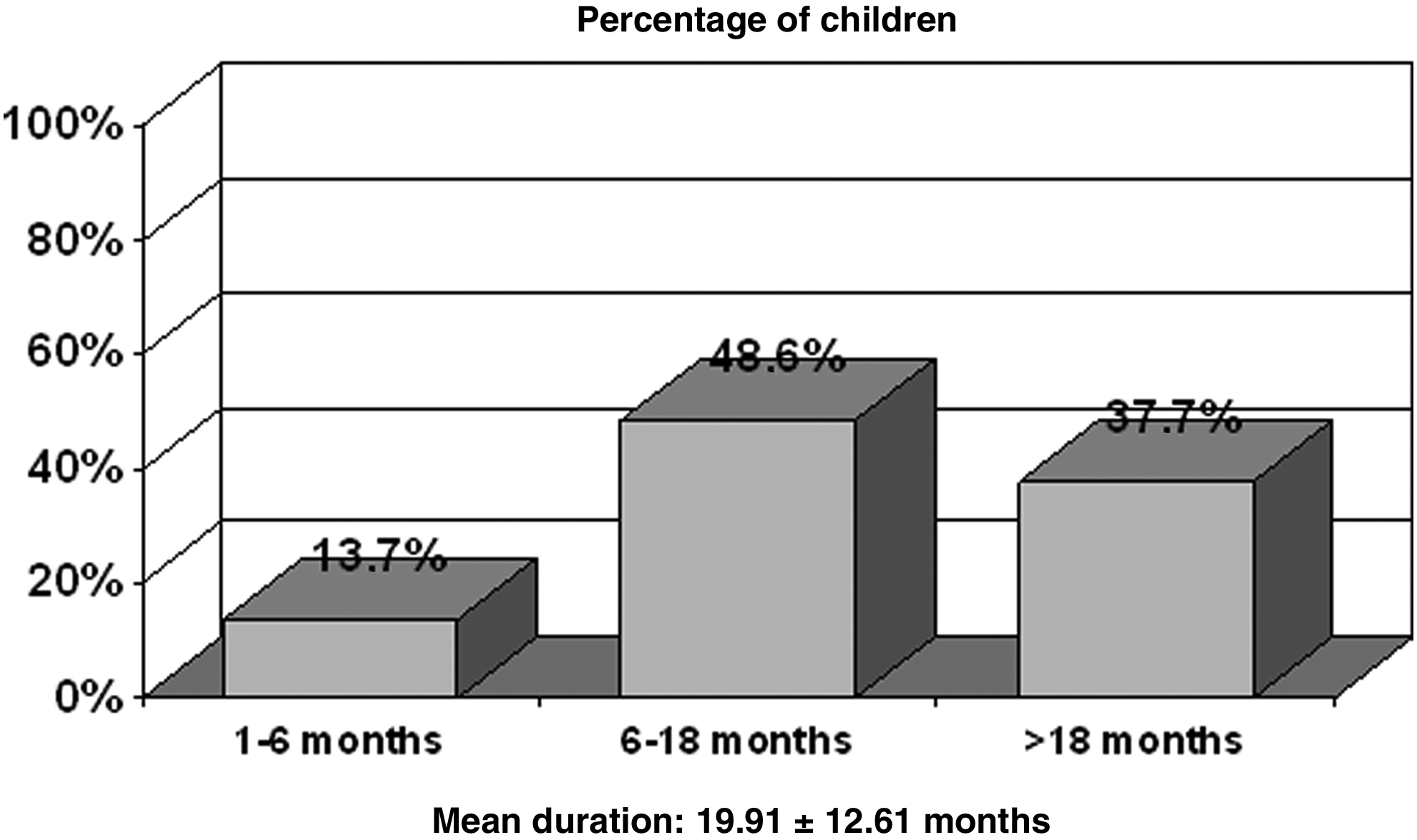
Duration of bottle feeding (mean duration, 19.91±12.61 months).
Because our aim was to explore the oral repercussions of breastfeeding and bottle feeding, we correlated the occlusal parameters obtained at exploration with the feeding variables of the children. In this context, a statistically significant relationship was observed between the type of feeding and the terminal plane: a larger percentage of straight terminal planes (favorable for occlusion) was recorded in the breastfeeding group, with a larger percentage of distal terminal planes (pathological) among the infants who were only bottle fed (Fig. 3). However, on considering the time factor referred to each feeding modality, a statistically significant correlation was observed with the duration of bottle feeding but not with the duration of breastfeeding (Figs. 4 and 5).

Terminal plane related to breastfeeding or bottle feeding. p<0.05.
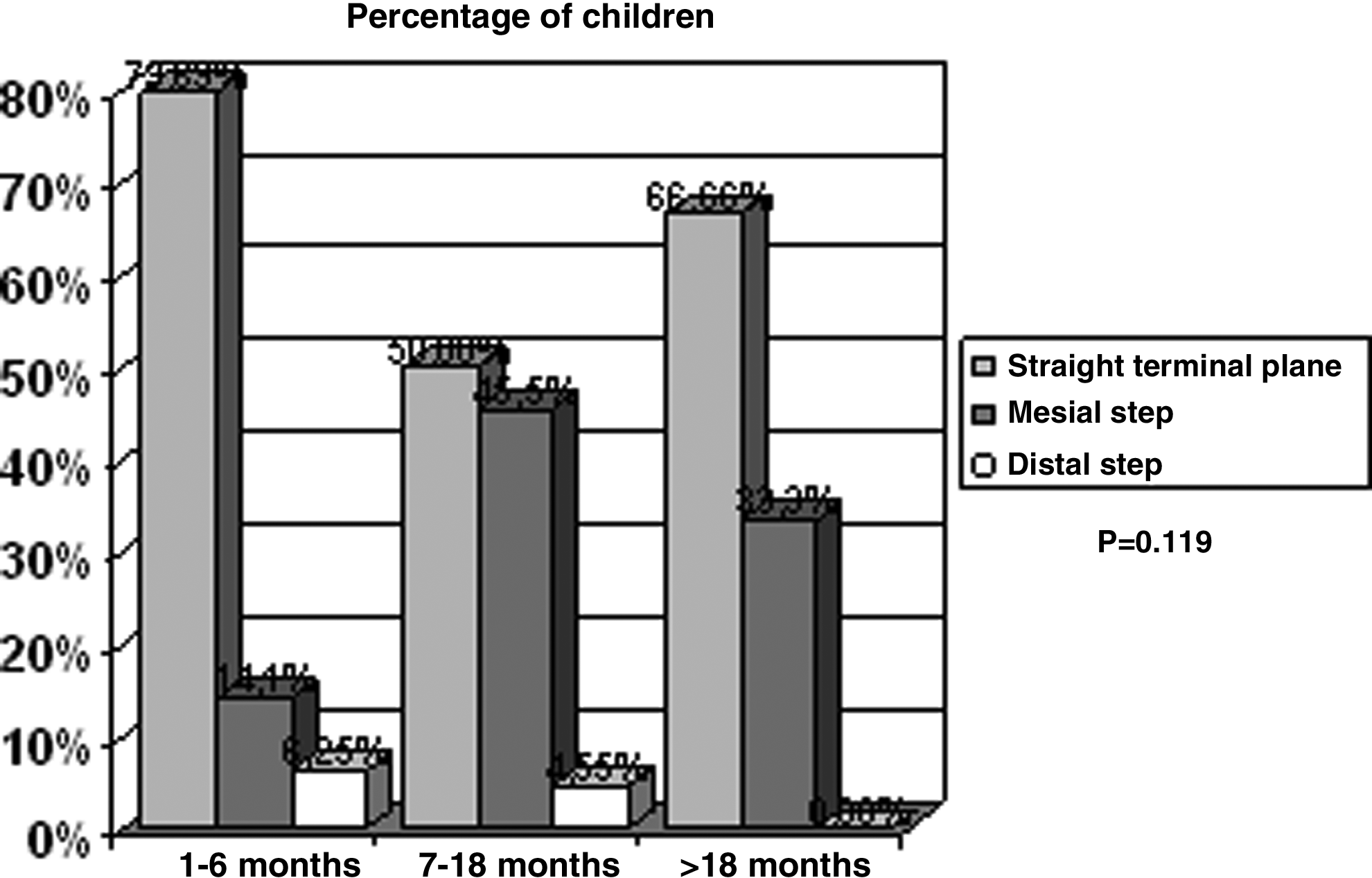
Duration of breastfeeding related to terminal plane. p=0.119.
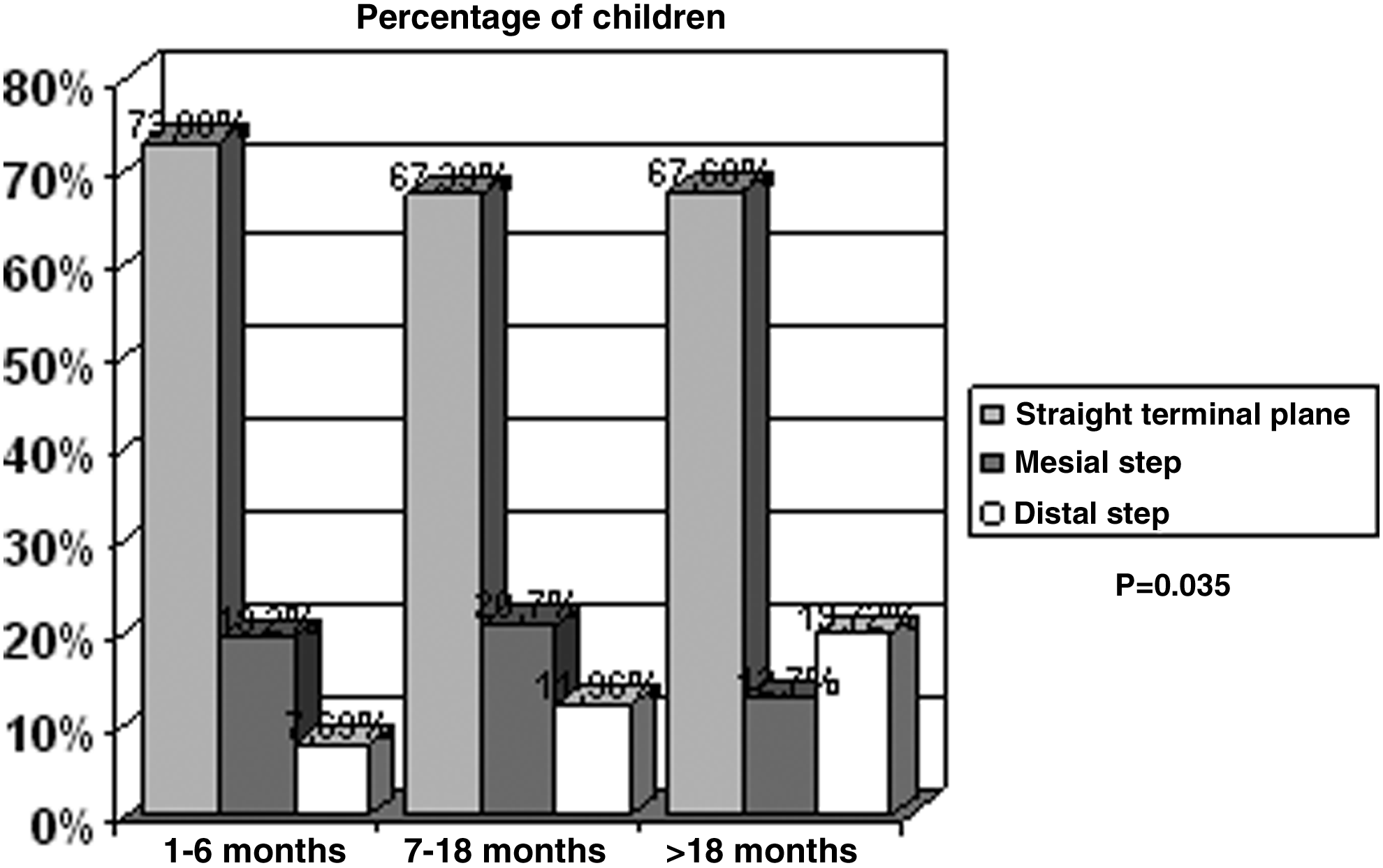
Duration of bottle feeding related to terminal plane. p=0.035.
Although statistical significance was not reached, the infants who were breastfed showed a higher incidence of canine class I relationship, which is optimum for dental occlusion (observed in 88.1% of the breastfed infants and in 81.5% of those who were bottle-fed only). In contrast, bottle feeding was associated with an increased probability of canine class II relationship, which is pathological (observed in 16.4% of the bottle-fed infants vs. 10.1% of the breastfed patients). However, the incidence of canine class III did not appear to be influenced by either breastfeeding or bottle feeding. Likewise, we found no significant differences in canine relationships on considering the duration of either breastfeeding or bottle feeding.
Again, although statistical significance was not reached, diastemas and primate spaces were seen to be more frequent among the breastfed infants than in those who received bottle feeding; this observation is favorable for correct occlusion. In effect, 36.1% of the breastfed infants had diastemas in both the upper and the lower arch versus 31.2% of those who received bottle feeding, whereas upper and lower primate spaces were recorded in 43.1% and 37.6% of the cases, respectively.
Dental crowding in turn was seen to be less common among the children who were breastfed than in those who received bottle feeding. On the other hand, and in the same way as in the case of the interincisal diastemas and primate spaces, no significant differences in crowding were noted on also considering the time factor (i.e., the duration of each feeding modality).
A significantly higher frequency of anterior open bite was recorded in the bottle-fed children. Likewise, and although statistically significant differences were not observed, the magnitude of overjet was greater among the infants that had received bottle feeding for the longest period of time.
Finally, as regards the occlusal parameters, we found no significant relationship between the duration of bottle feeding and posterior crossbite. Although we found a higher proportion of posterior crossbites for those bottle-fed children (16.65% vs. 14.67% among those breastfed), this was not statistically significant.
Discussion
Although all the major medical organizations advocate exclusive breastfeeding during the first 6 months of life,21–23 its prevalence and duration in Europe fall short of the World Health Organization recommendations. Nevertheless, between 1996 and 2006, the prevalence of exclusive breastfeeding during the first 6 months increased significantly in Europe, from 10% to 19%. 24
According to the latest data (those from 1997) of the Nursing Committee of the Spanish Association of Pediatrics, the average duration of breastfeeding is 3.2 months.25,26 However, the latest Spanish national health survey, conducted in 2006, found the percentage of women starting exclusive breastfeeding to be 68.4%, although only 24.7% maintained breastfeeding for 6 months. 27 In our series, 36.6% of the preschool children received breastfeeding, and of these, 43.1% were breastfed for more than 6 months. This indicates that the campaigns launched by different organizations in favor of breastfeeding are proving successful, at least in our setting, 28 although in our study 63.4% of the infants continued to receive bottle feeding, and 15.9% of these infants maintained this feeding modality for over 24 months.
As has been mentioned, breastfeeding is of great importance for correct development of the stomatognathic system. Proffit 8 described the great mandibular effort infants must make during the lactation period and underscored that this favors both nasal breathing and harmonious development of the dental arches. In turn, Legović and Ostrić 9 described how breastfeeding can condition the growth and development of the maxillofacial region.
All these aspects have been observed in our study, although corroborated by measurements of different occlusal parameters. Thus, we found a higher incidence of canine class I relationships in exclusively breastfed infants and a greater incidence of class II occlusions in those who had only received bottle feeding.
In agreement with the observations of Lescano and Varela, 29 our study recorded a higher frequency of interincisal diastemas and primate spaces in the breastfeeding infants and a greater incidence of dental crowding in those who were bottle fed. These dental spaces facilitate a better self-cleansing and a greater ease for dental hygiene, and therefore a lower probability of occurrence of dental caries in these children.
Some authors, such as Humphreys and Leighton, 30 have reported no deleterious effects of bottle feeding on dental occlusion. However, a great majority of investigators, including Hanna, 31 Harvold et al., 32 Van der Linden, 33 Hunt, 34 and Moss and Picton, 35 consider that bottle feeding for more than 18 months can cause occlusal disorders. A pioneering study in this sense was published by Hellman, 36 who suggested an association between bottle feeding and the appearance of certain malocclusions.
We observed a statistically significant relationship between bottle feeding and certain occlusal alterations, such as an increased frequency of distal step occlusion or canine class II relationships. This explains why authors such as Warren and Bishara 19 recommend suspending bottle feeding at an early age.
Although we observed no statistically significant increase in overjet in these preschool children, as described by other authors,30–32 in the anterior sector we noted a significant relation to open bite, likewise mentioned by the above authors, and more recently by Romero et al., 37 although these studies addressed not only feeding modality but also non-feeding habits.
Conclusions
Our study of the occlusal implications of exclusive breastfeeding or bottle feeding, independently of other bad non-feeding habits, found the parameters leading to correct occlusion (canine class I, interincisal diastemas, primate spaces, lesser dental crowding) to be more prevalent in infants who are breastfed, with a statistically significant relationship being observed in the case of the straight terminal plane.
In contrast, infants who are exclusively bottle fed show a significantly increased presence of terminal planes with distal step occlusion, canine class II relationships, anterior open bite, and crowding, with these being parameters that do not favor correct occlusion.
In view of the results obtained, we consider breastfeeding for at least 6 months to favor correct occlusion in the temporal dentition, which in turn facilitates normal occlusion in the permanent dentition.
Footnotes
Acknowledgments
All the authors have contributed in the same way to the development of the present study.
Disclosure Statement
No competing financial interests exist.