
Abstract

O
In June 2007, Nationwide Children's Hospital, Columbus, OH, added a peer counselor component (1.0 fulltime equivalent) to the already established lactation program based in the NICUs. A retrospective chart review was conducted on Nationwide Children's Hospital NICU admissions after the addition of peer counselors (January 1, 2008–June 30, 2008 and January 1, 2011–June 30, 2011). Medical records were reviewed from admissions to one of three main campus-based Level III NICUs (95 beds; 900+ admissions/year). Infants who were not admitted to the NICU within 7 days of birth, who died during hospital admission and/or whose mother died during hospital admission, who were medically unable to accept breastmilk, or whose mothers who were medically unable to provide breastmilk (i.e., human immunodeficiency virus–positive status, maternal drug abuse, and chemotherapy administration) were excluded. Additionally, in 2002 a lactation policy was implemented requiring lactation staff to screen infants within 72 hours of admission to determine level of care status for lactation intervention. If infants were not admitted to the NICU long enough for lactation staff to screen them, these infants were also excluded. The primary outcomes of interest were provision of any maternal breastmilk (infant receiving any maternal breastmilk via direct breastfeeding and/or pumping regardless of supplementation with formula), exclusive breastmilk (infant receiving exclusive maternal milk via direct breastfeeding and/or pumping without any formula supplementation), and any direct breastfeeding during NICU admission and at discharge (infant fed directly at the breast for at least one feeding with or without subsequent formula supplementation). Infants who received donor milk only were not included in analyses. This study received approval from the Nationwide Children's Hospital Institutional Review Board. χ2 tests were used to determine overall differences between specific lactation staff and breastfeeding outcomes during hospital stay. Analyses were completed using SAS version 9.3 software (SAS Institute, Cary, NC).
Overall, 401 mother–infant pairs made up the study population for analyses. Breastfeeding rates were highest for all breastfeeding outcomes during the hospital stay among mothers seen by both peer counselors and lactation consultants (Fig. 1). Specifically, 44% of mothers seen by both provided any breastmilk to their infants, versus 12% and 15% among peer counselors and lactation consultants only, respectively (p<0.001). Exclusive breastfeeding rates were 11% (vs. 2% and 3%, respectively; p<0.001), and direct breastfeeding rates were 31% (vs. 5% and 13%, respectively; p<0.001) among mothers seen by both. Similarly, any, exclusive, and direct breastfeeding rates at discharge were highest among mothers seen by both peer counselors and lactation consultants. Approximately 34% of mothers seen by both provided any breastmilk to their infants at discharge, compared with 11% and 14% among peer counselors and lactation consultants only, respectively (p<0.001). Exclusive breastfeeding rates were 19% (vs. 4% and 6%, respectively; p<0.001), and direct breastfeeding rates were 25% (vs. 4% and 12%, respectively; p<0.001).
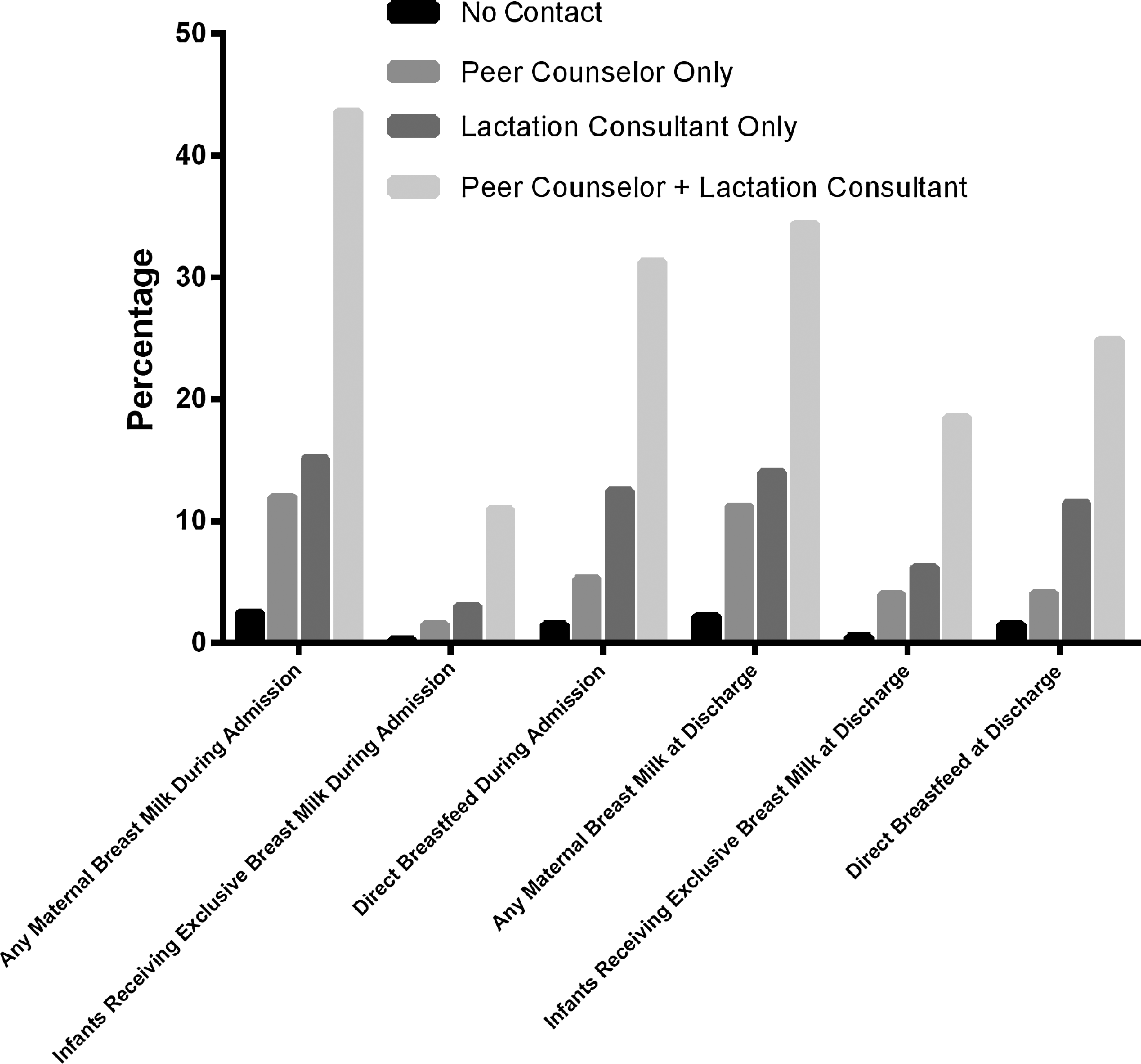
Breastfeeding outcomes during hospital stay by lactation staff type. χ2 tests for overall differences within each outcome were significant at p<0.001. Breastfeeding outcomes were classified as any maternal breastmilk (infant receiving any maternal breastmilk via direct breastfeeding and/or pumping regardless of supplementation with formula), exclusive breastmilk (infant receiving exclusive maternal milk via direct breastfeeding and/or pumping without any formula supplementation), and any direct breastfeeding during NICU admission and at discharge (infant fed directly at the breast for at least one feeding with or without subsequent formula supplementation) during neonatal intensive care unit admission and at discharge. Estimates do not include exclusive donor milk.
To our knowledge, this is the first study to show the combination of peer counselors and lactation consultants led to higher any, exclusive, and direct breastfeeding rates overall in a non-delivery hospital NICU setting. Research on breastfeeding support specific to non-delivery hospitals is lacking, and this study contributes data relevant to this setting. By expanding the lactation staff to add peer counselors, the proportion of mothers seen in the NICU increased (60% vs. 88%), which is likely one of the contributing factors to the observed increased breastfeeding rates. One of the main limitations of this study was the retrospective chart review study design, which relies on the medical record for data and thus issues related to clinical documentation and interpretation. 3 However, the breastfeeding data are based on medical chart documentation, not mothers' self-report, strengthening the reliability of the breastfeeding data. In conclusion, NICU lactation programs should consider combining lactation consultants with peer counselors to complement and enhance breastfeeding support to improve outcomes.
Footnotes
Acknowledgments
Thank you to the entire lactation team at Nationwide Children's Hospital for their efforts to improve NICU breastfeeding rates. Thank you to Nancy Ryan-Wenger, PhD, for her initial contributions to this project. Thank you to Sarah Keim, PhD, and Julie Gooding, MD, for comments on early versions of the manuscript.