
Abstract

Recent policy statements of the U.S. Surgeon General and the American Academy of Pediatrics strongly support HMBANA's mission:
Action 12: Identify and address obstacles to greater availability of safe banked donor milk for fragile infants —Actions to Improve Breastfeeding, The Surgeon General's “Call to Action to Support Breastfeeding,”
1
2011 The potent benefits of human milk are such that all preterm infants should receive human milk. Mother's own milk, fresh or frozen, should be the primary diet, and it should be fortified appropriately for the infant born weighing less than 1.5 kg. If mother's own milk is unavailable despite significant lactation support, pasteurized donor milk should be used. Quality control of pasteurized donor milk is important and should be monitored. —“Breastfeeding and the Use of Human Milk,”
2
American Academy of Pediatrics, 2012
HMBANA milk banks receive milk expressed, frozen, and donated by unpaid, screened, and approved lactating women, process it via the Holder pasteurization method, and dispense it to meet the specific medical needs of infants for whom it is prescribed. Some banks operate remote depots to provide additional local facilities to accept the milk, and some make provision to accept milk from remote locations shipped with dry ice. All member banks operate according to the organization's strict guidelines, updated annually. 3
Over 70% of the processed donor milk is dispensed to hospital neonatal intensive care units, primarily for treatment of severely low birth weight infants, who are at high risk for bloodstream infections, necrotizing enterocolitis, and feeding intolerances. Although mother's own milk is preferred, many mothers of premature infants are unable to provide an adequate supply of expressed milk, and, of course, breastfeeding is difficult or impossible with the very preterm. Donor milk is prescribed also for outpatient infants with such diagnoses as formula intolerance, feeding difficulties, malabsorption, failure to thrive, and congenital anomalies.
Currently 16 HMBANA banks operate in the United States and Canada, with several more under development or at various exploratory and planning stages (Fig. 1). Some HMBANA banks are established as independent, nonprofit organizations with their own boards of directors; others function as departments within hospitals or medical centers. HMBANA banks dispensed nearly 2,500,000 ounces of processed milk in 2012, an increase of 67% over 2009 (Fig. 2).

HMBANA milk bank locations in the United States and Canada: Calgary, AB, Canada; Vancouver, BC, Canada; San Jose, CA; Denver, CO; Indianapolis, IN; Coralville (Iowa City), IA; Kalamazoo, MI; Kansas City, MO; Newtonville (Boston), MA; Raleigh, NC; Columbus, OH; Austin, TX; and Fort Worth, TX, Oklahoma City, OK, Portland, OR, Toronto, ON, Canada, and other sites are in development (dark colored drops).
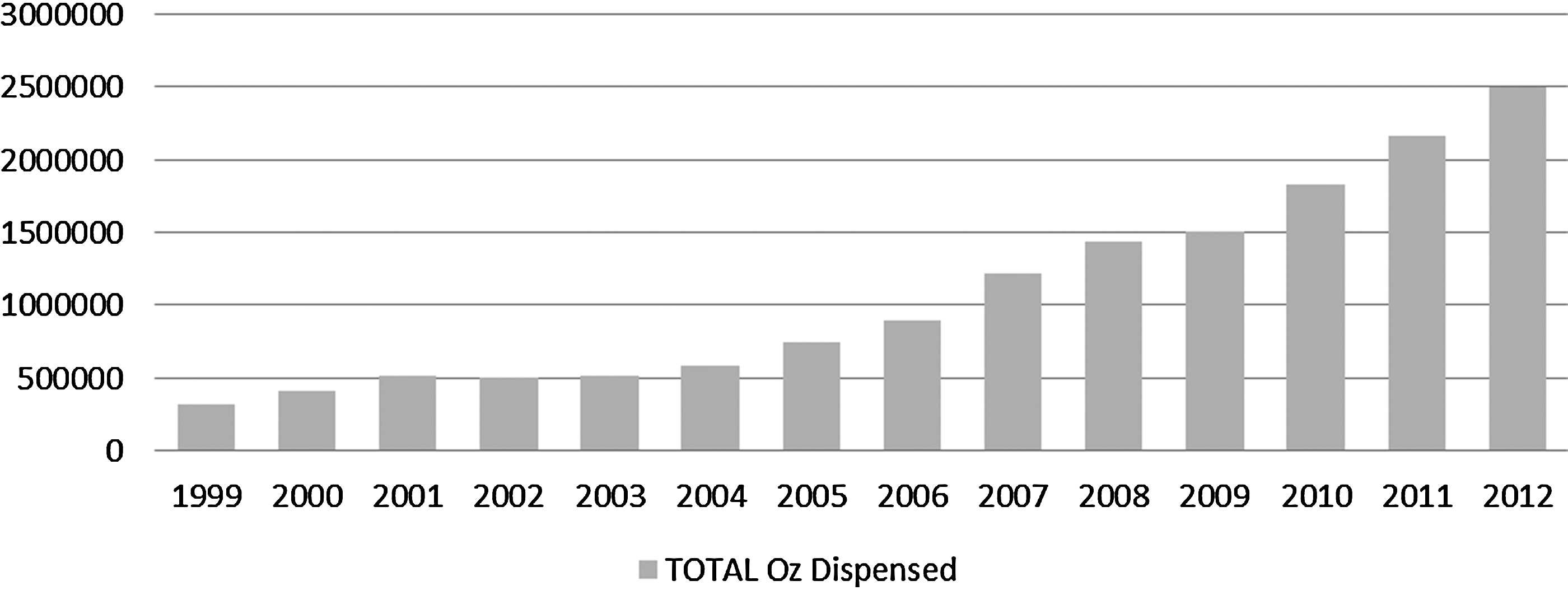
Growth in amount of donor milk dispensed by HMBANA milk banks.
Growth in the number of milk banks, the amount of donor milk dispensed, and the number of hospitals and outpatients served are testimony to the increasing recognition by healthcare providers and parents of the value of safe donor human milk.
4
HMBANA milk banks nevertheless face several challenges
5
:
• Demand outstrips supply. Growing numbers of hospitals are placing orders for donor human milk as research determines that, compared with formula, donor milk improves feeding tolerances, decreases sepsis and necrotizing enterocolitis rates, and reduces rates of re-hospitalizations. Outreach and advocacy by member banks and HMBANA also contribute to growing understanding of and requests for donor milk. Supply is limited, however, by suboptimal breastfeeding rates and a lack of awareness of milk banking and its benefits. • Informal sharing diverts some donor milk to less needy infants. Although no systematic data are available, it is evident that a substantial amount of donor milk is being shared informally or sold via Internet channels. This bypassing of milk banks presents two problems. First, recipient infants are put at risk when fed milk that has not been pasteurized and cultured from donors who have not passed screening tests. Anecdotal evidence indicates that some informal donors consider themselves healthy, despite being turned away by milk banks because of medication or herbal product use, risky lifestyle, or medical history. And, notwithstanding HMBANA's rigorous donor screening, each bank discards some donor milk that fails bacteriological standards for safe dispensing.
6
Second, donor milk shared informally or sold for feeding to healthy infants potentially deprives premature and at-risk infants of milk needed to survive and thrive. • Efforts to increase supply must not compromise safety. HMBANA's commitment to meeting demand for safe donor human milk led in 2011 to formation of two committees of experts in the fields of microbiology and pharmaceuticals. Each committee reviews clinical data to determine screening and bacteriological standards for donor human milk. Publication of a standard microbiology testing protocol for HMBANA milk banks in the 2013 Guidelines for the Operation of a Donor Human Milk Bank
3
aims to ensure optimal testing and subsequent dispensing or discarding of milk. The medication committee reviews data pertaining to the transferability of pharmaceutical products and the potential subsequent effect on the infant, leading to clear standards for screening and approving milk donors. • Variation in donated milk may affect health outcomes. Research conducted by the Mothers' Milk Bank at Austin, TX, demonstrates significant variation in the macronutrient levels of milk donated to a milk bank. These findings have led a majority of HMBANA milk banks to incorporate nutritional analysis and labeling into their processes. Although not an HMBANA requirement, per se, data on nutritional content provide important input for evaluation of infant outcomes. • Hospital funding and insurance coverage are often inadequate. The economic benefits of human milk compared with formula are now well documented. Despite these reports and the costs to insurance carriers for inpatient neonatal care, many neonatal intensive care units remain resistant to providing unit funds to cover donor human milk processing fees. Parents of outpatients face an even greater challenge as private insurers frequently refuse to cover donor milk fees. Several HMBANA milk banks maintain charitable care programs, funded by donations, to provide financial assistance to outpatients' families who lack resources. It is not yet known how healthcare reform will affect this situation.
HMBANA and its member banks are responding to these challenges through outreach and advocacy via traditional and social media channels, engagement in and support for research and development, and partnerships with providers, researchers, and other advocates, including the United States Breastfeeding Committee. HMBANA milk banks are increasingly recognized for their critical role in the infant healthcare system.
Footnotes
Disclosure Statement
No competing financial interests exist.