
Abstract
Abstract
Background:
Worldwide, women fail to reach the recommended exclusive breastfeeding target of 6 months postpartum. The objective of this study was to present a conceptual and methodological synthesis of interventions designed to promote exclusive breastfeeding to 6 months in high-income countries.
Materials and Methods:
A systematic search of leading databases was conducted for scholarly peer-reviewed randomized trials published between January 2000 and June 2013. Seventeen articles were identified as relevant; all were published in English and assessed exclusive breastfeeding with a follow-up period extending beyond 4 months postpartum. Articles were analyzed for overall quality of evidence, regarding duration of exclusive breastfeeding, using the Grading and Recommendations Assessment, Development, and Evaluation approach.
Results:
A significant increase in the duration of exclusive breastfeeding was found in eight of the 17 studies, with most interventions using supportive or educational approaches. Interventions in pregnancy focused on educating mothers on the benefits of exclusive breastfeeding. Fifteen interventions took place, at least in part, in the postnatal period and provided educational and emotional support to mothers. Of the eight successful interventions, five took part in the postnatal period in the mothers' own homes. The quality of the evidence for duration of exclusive breastfeeding was moderate.
Conclusions:
The most successful interventions were conducted in the postnatal period and over a long period of time; however, the findings were inconsistent. No study assessed intervention fidelity, and only two studies noted maternal body mass index, a variable known to affect exclusive breastfeeding rates. Further research is needed to provide a robust evidence base to inform future interventions.
Introduction
T
The WHO recommends exclusive breastfeeding in the first 6 months of life, and yet data suggest that globally the percentage of babies exclusively breastfed for <6 months (babies 0–5 months exclusively breastfed in the previous 24 hours) is only 37%. 10 The determinates of these rates vary across the world and become very evident when comparing low- and high-income countries. Barriers and determinants of breastfeeding in low-income countries include cultural beliefs, education, marketing of formula, and access to healthcare, among others.11–14 Barriers in high-income countries include obesity, 15 returning to work, 16 poor family support, 17 and embarrassment about feeding in public, 17 as well as education. 17 This review focuses specifically on studies published with women from high-income countries.
In Australia, around 90% of all women initiate breastfeeding. Over time, however, the number of babies exclusive breastfed declines dramatically, with only approximately 2% of infants exclusively breastfed to 6 months of age. 18 The latest U.S. data report that exclusive breastfeeding at 6 months varies considerably, from 26.3% to as low as 7.6%, averaging 16.3%. 19 The rates of exclusive breastfeeding are even lower in the United Kingdom, with <1% of women reporting exclusive breastfeeding to 6 months. 20 These rates reflect a significant public health problem that needs to be addressed.
The past decade has seen several interventions designed to increase the initiation of breastfeeding as well as exclusivity to 6 months. However, to our knowledge, there has been no systematic review of interventions specifically designed to increase exclusive breastfeeding to 6 months in high-income countries. Previous review articles have focused on low- and middle-income countries, 21 structured versus non-structured breastfeeding programs, 22 health benefits, including the effect of breastfeeding on infections during infancy,23,24 breastfeeding after cesarean delivery, 25 and the psychosocial predictors of exclusive breastfeeding. 26 The primary aim of our systematic review was to reveal the effective elements of exclusive breastfeeding interventions in high-income countries with a secondary aim to provide recommendations for clinical practice. We included studies published from 2000 onward by evaluating the methods adopted (i.e., the sample of women targeted, the content of the intervention, the duration, the pre- and post-intervention measurements, the definition of exclusive breastfeeding), the theory driving the intervention, and the quality of the evidence using the Grading and Recommendations Assessment, Development, and Evaluation (GRADE) guidelines. 27
Materials and Methods
Information sources
Articles were acquired from a search of nine databases: Academic Search Complete; CINAHL with full text; The Cochrane Library: Embase: Health Policy Reference Centre; Health Source Consumer Edition; Health Source—Nursing/Academic Edition; Maternity and Infant Care: MEDLINE with full text; PsycARTICLES; Psychology and Behavioral Sciences Collection; and PsycINFO. The search terms used (Fig. 1) resulted in a total of 952 abstracts, which were reviewed for suitability by one author (M.F.). A full electronic search strategy for the MEDLINE database is shown in Supplementary Figure S1 (Supplementary Data are available online at www.liebertonline.com/bfm).

Search terms.
Eligibility criteria and study selection
A search of scholarly peer-reviewed publications was conducted for recent randomized trials published in English between January 2000 and June 2013. Articles were excluded if they were not published in English, had a follow-up period of <4 months postpartum, or referred specifically to developing or low-income countries. Other exclusion criteria were articles specific to adolescent mothers, those not aimed at increasing exclusive breastfeeding specifically, or those specific to breastfeeding in the presence of maternal smoking or a human immunodeficiency virus–positive status. Of the initial 952 abstracts revealed, 30 full-text articles were found to be relevant and were read in their entirety by all the authors. With unanimous agreement across authors obtained by discussion, a further 13 articles were excluded, leaving 17 studies for the current review: 13 randomized controlled trials and four cluster-randomized trials (Figure 2 gives a summary of the systematic search record, and Supplementary Table S1 details excluded studies with reasons).
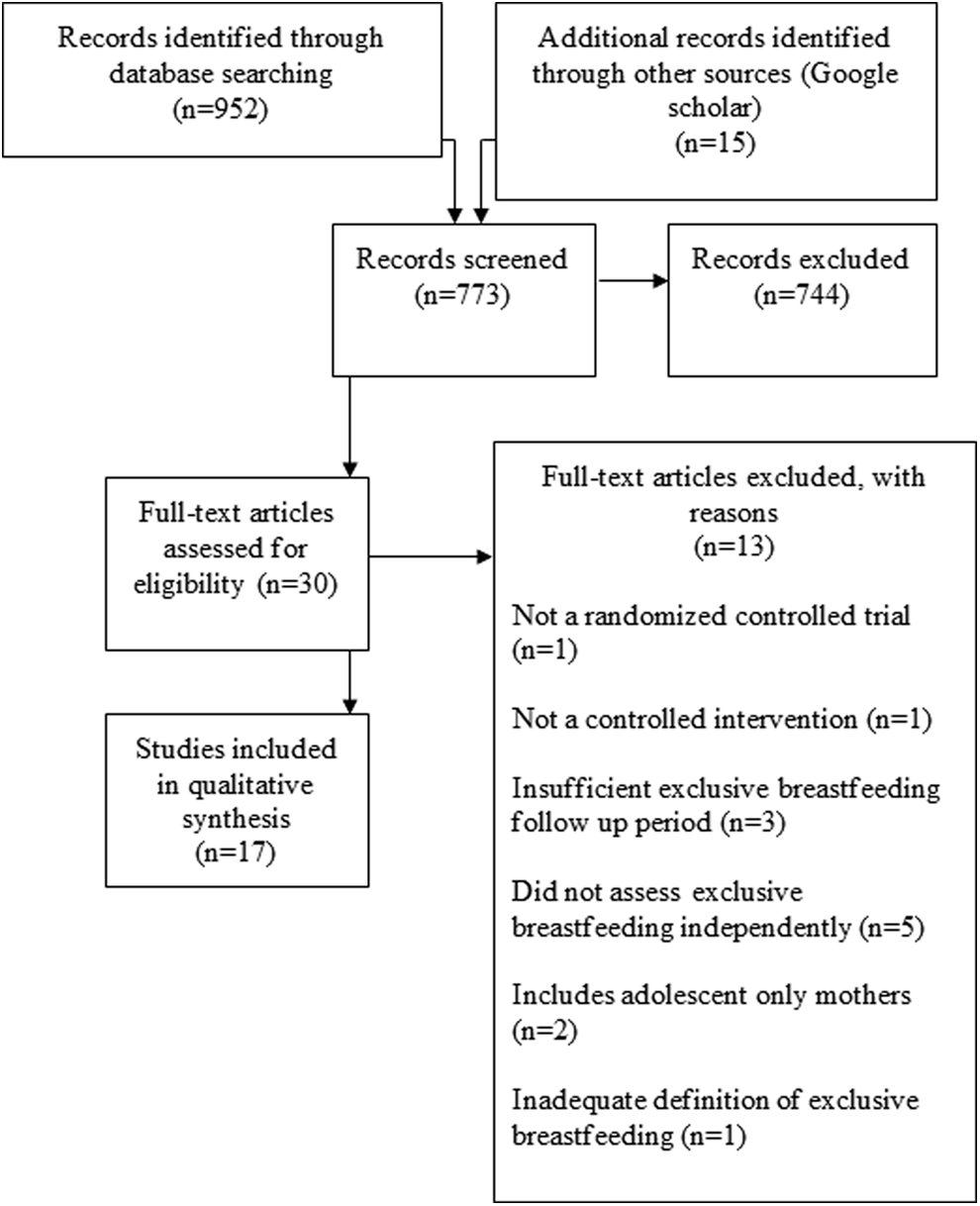
PRISMA systematic search record.
Data collection
Data including authors and country, main aim, main outcomes, sample, design, exclusive breastfeeding definition, and theoretical basis were extracted from articles and entered into Table 1.
BIBS, Bassett Improving Breastfeeding Study; BMI, body mass index; NA, not available; SD, standard deviation; SES, socioeconomic status; SGD, Singapore dollars; USD, U.S. dollars.
Risk of bias
Risk of bias for individual studies was determined by a validity scoring system, modified from the Cochrane Collaboration's tool for assessing risk of bias and used by Gardner et al. 28 This system assesses and scores statistical power, intervention fidelity, blinding of outcome assessors, and intention-to-treat analysis. Scores were awarded on achievement of the required criteria. For statistical power, studies were allocated a score of 2 where power was met and a score of 0 where power analysis was not noted or statistical power was not met. Studies were given a score of 2 when attempt to assess intervention fidelity was noted and a score of 0 when intervention fidelity was not noted. For blinding of outcome assessors, studies were awarded a score of 2 where assessors were blind to group allocations and a score of 0 where blinding was either not implemented or not mentioned in the design of the study. Finally, if no intention-to-treat analysis was used or this was unclear, studies were allocated a score of 0, and they were scored as 2 if it was used. The mean risk of bias score for all included studies was assessed; scores could range from 0 to 8, with lower scores indicating a higher risk of bias.
Data analysis using the GRADE approach
The included studies were also assessed for their overall quality of evidence using the GRADE approach 27 as recommended by the Cochrane Handbook for Systematic Reviews of Interventions. 29 The trials were evaluated for the five factors that decrease the quality of evidence: limitations of the design, inconsistency, indirectness, imprecision, and publication bias. Then the three factors that increase the quality of the evidence—having a large magnitude of effect, plausible confounding variables, and dose–response gradient—are added. An overall determination can then be made about the quality of evidence. Randomized controlled trials have a high rating, and this is either downgraded or upgraded dependent on the GRADE evaluation.
Results
General description
Of all the interventions, five were conducted in the United States,30–34 three each in Australia35–37 and the United Kingdom,38–40 and one each in Turkey, 41 The Netherlands, 42 Denmark, 43 the Republic of Belarus, 44 Singapore, 45 and Malaysia. 46 One study 32 revealed the author used theoretical underpinnings in the development of his intervention, referencing the social cognitive learning theory of Bandura.47,48 Two of the 17 trials stated explicitly that they adopted the WHO's definition 1 of exclusive breastfeeding.42,46 Two studies used the term “full breastfeeding,” which allows for the consumption of vitamins, minerals, water, juice, medicine, and ritualistic and traditional liquids.36,37 Nine of the 17 interventions defined exclusive breastfeeding as the infant receiving nothing but breastmilk,30,31,34,35,38,41,43–45 with the remaining studies not providing a definition.32,33,39,40
In the reviewed studies, the ages of participants ranged between 16 and 40 years. The ethnicity of participants varied owing to the international sample. Three studies included a sample of approximately 70% white participants.31,38,39 Two studies included approximately 70% African American participants.33,41 The study of Bonuck et al. 30 included 57% Hispanic women and 36% African American women. Tahir and Al-Sadat 46 reported a predominantly Malay sample. Furthermore, Kronborg et al. 43 reported that all their participants were Danish, and the studies conducted in Turkey and Jordan did not specifically note ethnicity.36,41
Six studies included only primiparous women in their sample.32,34–36,40,41 One study did not note parity percentage, 44 whereas another did not mention participant parity. 33 For all the remaining studies both primiparous and multiparous women were evenly distributed.30,31,34,37–39,41,45,46
Risk of bias
The average risk of bias across all studies was 2.8 out of a possible 8 using the scoring system previously described (higher scores equal lower risk of bias). No study achieved the maximum score of 8. Only one study received a score of 6, 43 seven received a score of 4,4,30,35,36,38,39,45 seven received a score of 2,31,32,34,37,40,42,46 and two received a score of 0.33,41
Intervention components
Details of the intervention methodologies (time of delivery [prenatal and/or postnatal], delivery by hospital staff and/or lactation experts, peer support, telephone support, face-to-face support, number of intervention sessions/duration of intervention, follow-up time points, and findings in relation to success of the interventions for any breastfeeding and for exclusive breastfeeding) are presented in Supplementary Table S2. The majority of interventions focused primarily on providing maternal support30,33,34,37,43,46 or education.35,36,39,41,42,45 Other methods investigated the use of sidecar cribs attached to mothers' beds, 38 mother–infant skin-to-skin contact, 31 breastfeeding logs, 32 or midwife education.40,44
All four interventions implemented during pregnancy focused on maternal education. This was through antenatal classes,35,39 lactation consultant/peer counseling, 30 and written and oral information regarding breastfeeding practices and milk storage. 42 Of these interventions, two continued into the postnatal period. One provided a single in-hospital and a single home postnatal visit to women and made lactation consultants available until 12 months postpartum. 30 The other provided one postnatal home visit; however, the specific timing was not defined. 42 Overall, most education interventions focused on training the mothers by providing advice and teaching skills about exclusive breastfeeding practices. This was provided in both a one-on-one36,41,42,45 and group35,39 setting.
Six of the interventions that commenced in the postnatal period provided home/telephone support. Two provided face-to-face home visits,41,43 three provided telephone support,34,36,46 and one provided both. 33 One intervention utilized peer support persons, 33 and another applied physical stimulation via breastfeeding pumps. 34
Several postnatal interventions provided only in-hospital support to mothers through midwife education strategies,40,44 mother–infant proximity,31,38 or single educational sessions and educational material. 45 In contrast, Pollard 32 focused on increasing the mother's awareness by encouraging self-monitoring via a daily breastfeeding log; this intervention took place within the participant's home and was self-administered.
Effect of interventions on initiation/duration of exclusive breastfeeding
Of the 17 studies included in this systematic review, eight did not significantly increase the duration and rates of exclusive breastfeeding,30,34–40 whereas nine demonstrated a statistically significant improvement.31–33,41–46 Of these significant results, only seven significantly increased exclusive breastfeeding rates to 6 months postpartum.31–33,41–44 Furthermore, only Kramer et al. 44 assessed their results for clinical significance; they concluded that their findings represented a substantial clinical reduction in an infant's risk of infection.
Successful interventions
Successful interventions tended to be support-based programs providing additional home-based and telephone support by lactation experts.33,43 These support interventions commenced in the postnatal period and extended over a relatively long period (from approximately 5 weeks to 6 months). Two interventions were education-based: one focused on providing additional face-to-face postnatal breastfeeding education 3 days after birth, 41 and the other used written and verbal information in both the prenatal and postnatal periods. 42 Other successful interventions used novel approaches for breastfeeding promotion. One used unlimited kangaroo care (skin-to-skin contact), 31 and another used self-observation via a breastfeeding log. 32 Additionally, a study compared nurses trained in the WHO and UNICEF Baby-Friendly Hospital Initiative 9 with those administering usual care. 44
Of all successful interventions, only one commenced in pregnancy 42 ; however, this study continued into the postnatal period. Two interventions concluded at hospital discharge.31,44 Other successful interventions spanned a longer period: from a minimum of 3 weeks 32 up to 5 weeks 43 through to 6 months. 33 The final successful study designed their program so the participant had only one contact with the intervention. 41
Unsuccessful interventions
Studies that did not demonstrate a significant increase in the duration of exclusive breastfeeding were generally education only and provided one intervention session to mothers.35,36,39 Only one of these included follow-up phone calls (at 2 and 4 months after birth). 36 Another unsuccessful intervention educated midwives to use a “hands off” approach to breastfeeding care. 40 Studies attributed their negative results to the Hawthorne effect,36,39 existing high standards of maternal breastfeeding care, 34 and under-recruitment of participants. 40
Some support interventions did not demonstrate a significant increase in exclusive breastfeeding. Two provided long-term lactation counseling/care to mothers,30,37 whereas another assessed the effects of telephone support or the use of a breast pump in obese women.34,46 One intervention comprised a trial of sidecar cribs attached to mothers' hospital beds. 38 Of those interventions that did not demonstrate an effect on exclusive breastfeeding, two were conducted in pregnancy only,35,39 whereas the remainder were implemented in the postnatal period.30,34,36–38,40,46 Furthermore, the majority of unsuccessful interventions were short-term, taking place during participants' hospital stay34,38,40 or were single-contact interventions.35,39 Four interventions provided some ongoing support or education following hospital discharge.30,36,37,46 Of these latter support interventions, one identified the in-hospital nature of the trial implementation as a limiting factor; it suggested that the intervention may have been more successful had it been implemented within the comfort of participants' own homes. 30 Other results were attributed to existing high breastfeeding rates in the study population 37 and increased awareness of breastfeeding practices caused by weekly reporting. 38 The intervention not being implemented as planned 34 was another stated reason, as well as the unknown combination of multiple factors that influence exclusive breastfeeding at 6 months. 46
Intervention control and fidelity
Detailed information regarding study power, intervention fidelity, definitions of usual care, stratification, consideration of maternal body mass index, and intention-to-treat analysis is provided in Supplementary Table S3. Of the 17 included studies, seven either did not provide power calculations, or the studies were underpowered.33–35,39–41,45 Of these, four did not provide evidence of effectiveness of the intervention being examined in the trial.34,37,39,40 Furthermore, in the studies where several individuals were involved in the delivery/implementation of the intervention, the researchers did not assess the fidelity of the administration of the intervention program.30,31,33–42,44,45
Demographic factors such as age, education, socioeconomic status, and parity were measured and considered when sampling and analyzing the data. However, only two studies reported maternal body mass index,34,46 which is a known risk factor that impacts breastfeeding rates.49–51
GRADE quality rating of evidence
Given that all included intervention studies were randomized controlled trials, there is potential for a high quality of evidence. However, because of the inconsistent results produced by these studies as well as the limitations of design (lack of power, lack of intervention fidelity, use of some unstandardized measures, and varied definitions of both exclusive breastfeeding and “usual care”), the quality of evidence for breastfeeding interventions and exclusive breastfeeding outcomes is moderate according to GRADE guidelines (see Supplementary Table S4).
Discussion
The aim of this systematic review was to reveal the effective elements of interventions designed to increase exclusive breastfeeding to 6 months. We have provided a conceptual and methodological synthesis of the strategies used in order to better understand what makes such interventions successful.
The vast majority of successful interventions commenced in the postnatal period,32,33,41,43–45 with only one beginning in pregnancy and continuing into the postnatal period. 42 These findings indicate that the postnatal phase is likely the most effective time to promote exclusive breastfeeding. Aksu et al. 41 credited their intervention's success in part to the delayed (3 days postpartum) education provided to mothers. They believed this delay allowed mothers to recover, settle, and approach breastfeeding concerns with a clear and calm mindset. The women returned home 24 hours after birth, and perhaps the delay in study initiation gave the women time to adjust, which assisted in their confidence.
It is also important to note that the majority of successful interventions continued for a relatively long period (from 3 weeks to 6 months), providing ongoing assistance to mothers.32,33,42,43 It is likely that extended contact with support persons, as well as the intervention program itself, assisted in the increase of maternal confidence, persistence, self-efficacy, and motivation.
Overall, support-based initiatives were the most successful in increasing the duration of exclusive breastfeeding. The success of these interventions may be due to increasing maternal confidence and breastfeeding self-efficacy through interaction with lactation professionals33,43 and peer support persons. 33 The highly interactive nature of these supportive interventions may be more meaningful to women, thereby promoting longer-term breastfeeding practices. Interventions provided to mothers within their own home appear to be effective, with five of the eight successful interventions doing so.32,33,41–43 It is possible that by providing interventions in homes, researchers were able to reduce anxiety and allow the women to make full use of the programs provided to them.
It has been proposed that education programs that include various forms of support may be successful in the promotion of sustained breastfeeding. 52 Therefore it is not surprising that education and support were the two main approaches to breastfeeding promotion in the trials reviewed here. Support was given in several ways, including peer support, expert counseling, and the Baby-Friendly Hospital Initiative. Promotion efforts via education typically took place in the prenatal stage, with researchers theorizing that this knowledge would influence a mother's intentions to initiate and maintain exclusive breastfeeding. Three education-only interventions successfully increased exclusive breastfeeding.41,42,45 Results by Gijsbers et al. 42 support previous research and indicate that increasing a mother's intention to breastfeed in the prenatal period can increase initiation and duration of breastfeeding.53,54 However, given that Aksu et al. 41 conducted education in the postnatal period, it may have been the supportive, face-to-face nature of their intervention that led to their significant findings.
Of the successful interventions included in the current review, several have incorporated the social learning and cognitive theories of Bandura.47,48 These theories highlight the importance of a strong support network, 47 as well as the internal concept of self-efficacy, or self-confidence in motivating behavior. 48 Previous research indicates the importance of these theories in predicting breastfeeding behavior. A positive relationship has been found between social support and breastfeeding success.55,56 Additionally, breastfeeding self-efficacy in mothers significantly impacts breastfeeding initiation and duration.57–59 Of these successful interventions one incorporated peer support, 33 and three included self-efficacy building support strategies administered by lactation experts.33,43,44 Another provided education by lactation consultants, 45 with the remaining utilizing a daily feeding log to help women monitor and compare their breastfeeding behavior. 32
What are the limitations of current approaches to exclusive breastfeeding promotion?
Of the interventions that did not produce statistically significant results, one was underpowered to detect differences between intervention and control groups, 40 and another did not provide a power calculation. 34 Insufficient participant numbers were likely to have had a detrimental effect on the ability of these studies to detect a change if one existed and may in part explain the lack of evidence of effective interventions.
Interventions were inconsistent in their definition of “usual care,” and 10 did not even provide a definition32,34,36,38–40,42,44–46 (see Supplementary Table S3). In trials where usual care was defined, there was substantial variation: from one midwife-implemented education session 41 to accessing a large number of resources as well as postnatal home visits.33,35,37 This lack of a common definition of “usual care” makes the comparison of the intervention's effectiveness difficult. In an instance where “usual care” is very supportive, the numbers needed to detect a statistical difference would need to be inflated.
In cases where several research team members were involved in intervention implementation, no details were provided of measures undertaken to assess the administration of the intervention program. One study did attempt to stratify participants by midwife experience in an effort to reduce variation. 40 However, sample size appears not to have been adjusted for stratification, and whether this intervention was implemented in a consistent way is unknown. Of all interventions included in the current review, 10 were analyzed on an intention-to-treat basis.30,34–39,43–45 Of these interventions only three were successful at increasing exclusive breastfeeding practices,36,43,45 with only two of these significantly increasing exclusive breastfeeding to 6 months postpartum.36,43 Furthermore, four of the reviewed studies that included more than one service provider did not stratify participant randomization across maternity services.30,31,36,42
The majority of the studies reviewed here did not report maternal body mass index (see Supplementary Table S3). Evidence indicates that women who are classified as obese have increased difficulty in breastfeeding, including positioning, 15 and a delay in lactation49,60 and discontinue breastfeeding sooner than women of normal weight,47,48 often within 2 weeks postpartum. 61 This increased difficulty along with the growing concern of global obesity rates complicates the challenge of complying with WHO breastfeeding recommendations. 62
Future research
Our review has highlighted limitations in the research to date that prevent definitive conclusions about intervention efficacy. It is clear there is a need to continue research in this area to develop effective interventions that promote exclusive breastfeeding in women. Furthermore, this research needs to be adequately powered to detect a significant increase in the proportion of women breastfeeding exclusively to a designated time point after birth (preferably to 6 months after birth, in line with WHO recommendations). 1 The design of new interventions needs to be guided by theory for the greatest chance of a successful intervention.
There are several specific areas where further research is needed. This includes ways to better understand and promote the efficacy of interventions delivered within one's home, which were shown to be effective. Recognizing that maternal body mass index has a measurable effect on exclusive breastfeeding duration, it becomes even more important that breastfeeding interventions are robust and potentially specialized for overweight and obese women. Interventions that focus on overcoming the barriers of breastfeeding to 6 months, including maternal perceptions, embarrassment, and family support, among others, are also very important.
Conclusions
The findings of this review suggest that postbirth support-based programs that extend over a relatively long period and generally take place within the women's homes are effective in increasing exclusive breastfeeding initiation and duration. Given the benefits of exclusive breastfeeding for both infants and mothers, research into interventions that extend it to 6 months is urgently needed.
Author Contributions
All authors planned the article. M.F. performed the systematic search under the guidance of H.S. and C.N. H.S. wrote the article with M.F. C.N., B.K., P.S., and H.M. read multiple drafts and provided constructive feedback for further improvements.
Footnotes
Disclosure Statement
No competing financial interests exist.