
Abstract
Abstract
Background:
Although breast pain remains a common cause of weaning, controversy exists regarding the etiology of chronic pain. Prospective studies are needed to define optimal treatment regimens. We evaluated patient history, exam, and bacterial cultures in breastfeeding women with chronic breast pain. We compared pain resolution and breastfeeding complications in patients responding to conservative therapy (CTX) (n=38) versus those in patients failing CTX and receiving oral antibiotic treatment (OTX) (n=48).
Subjects and Methods:
We prospectively enrolled 86 breastfeeding women with breast pain lasting greater than 1 week and followed up patients through 12 weeks.
Results:
Higher initial breast (p=0.012) and nipple pain severity (p=0.004), less response to latch correction (p=0.015) at baseline visit, and breastmilk Staphylococcus aureus growth (p=0.001) were associated with failing CTX. Pain type was not associated with failure of CTX. When culture results were available at 5 days, breast pain remained higher (p<0.001) in patients failing CTX and starting antibiotics. OTX patients then had more rapid breast pain reduction between 5 and 14 days (score of 3.1 vs. 1.3; p<0.001). By 4 weeks there was no difference (1.8/10 vs. 1.4/10; p=0.088) in breast pain level between groups. Median length of OTX was 14 days. At 12 weeks, weaning frequency (17% vs. 8%; p=0.331) was not statistically different.
Conclusions:
Initial pain severity and limited improvement to latch correction predicts failure of CTX. S. aureus growth is more common in women failing CTX. For those women not responding to CTX, OTX matched to breastmilk culture may significantly decrease their pain and is not associated with increased complications.
Introduction
D
When evaluating chronic pain, clinicians turn to history and physical exam findings.12,22 Commonly pink and flaky sore nipples, and deep, burning, stabbing, shooting, radiating, “feels like glass,” and itching pain are attributed to yeast,7,10,13,17,22–24 whereas past or present cracked nipples, deep, dull aching pain, and breast tenderness on exam are attributed to chronic bacterial infections.12,25 Prospective reporting on history and exam findings that correlate with microbiological data for chronic breast pain is limited and does not follow prospectively through treatment.6,8,24
Conflicting data on yeast and bacteria complicate the treatment of breastfeeding women with chronic breast pain.12,13,17,26 Andrews et al. 10 found a higher frequency of yeast growth. Amir and Pakula 7 and Amir et al. 8 found both Candida and Staphylococcus aureus growth to be higher, whereas Hale et al. 26 found no Candida growth in women with chronic breast pain. Common clinical practice includes treating women with antifungal medication for presumed yeast infections. 22 Yet, recent studies question this practice and suggest a bacterial etiology.12,13,17,26 Clinical treatment remains varied and primarily based on microbiologic or retrospective studies.20–22,27
Data gathered from studies on bacterial causes of acute mastitis and infected nipples found S. aureus to be pathogenic and treatment with oral antibiotics to be beneficial.14,28 The increased frequency of S. aureus in women with chronic pain8,13,29,30 raises the possibility that oral antibiotic treatment (OTX) may decrease pain. In addition to S. aureus, there is speculation that coagulase-negative Staphylococcus (CNS) causes pain.8,12,31 Some experts propose prolonged courses of oral antibiotics for a chronic lactiferous infection. 12 Despite microbiologic studies, little is known about the association between culture results and response to antibiotic treatment.
This study was undertaken to prospectively evaluate the history, exam, bacterial frequency, and quantitative culture results of breastfeeding women with chronic breast pain and prospectively follow responses to conservative therapy (CTX) or OTX.
Subjects and Methods
Study population
The study was conducted at Breastfeeding Medicine of Northeast Ohio, a referral practice for mothers in Northeast Ohio needing specialized medical evaluation for breastfeeding difficulties. This practice is located at a private suburban pediatric practice in Cleveland, OH, viewed by the community as breastfeeding friendly.
Study design
This prospective study was conducted from April 2011 to December 2012. Inclusion criteria for cases were breastfeeding women 18 years old or older presenting at their initial visit to Breastfeeding Medicine of Northeast Ohio with a history of breast pain lasting more than 1 week. Women were excluded if there was clinical evidence of acute inflammation (erythema, warmth, induration, mastitis, or abscess) or plugged ducts or if their symptoms resolved in the office following correction of mechanical factors such as incorrect latch or frenotomy. The first author recruited all cases. All participants gave written informed consent. The research study was approved by the Case Western Reserve University Institutional Review Board.
During the 18-month study period, 494 mothers were evaluated for breastfeeding consults. The two most common reasons were low milk supply (32%) and pain (48%). Of the 237 mothers seen for pain, 148 were excluded because their pain lasted less than 1 week or resolved in the office with treatment, or there was evidence of acute inflammation on initial exam. Eighty-nine mothers with pain lasting more than 1 week were enrolled (Fig. 1). At the initial visit, all women completed a patient questionnaire for demographic information and clinical history. At enrollment, history, exam, and treatment data were collected along with nipple swab and breastmilk samples for quantitative bacterial cultures. All women received initial CTX with mechanical correction, lactation support, and topical ointments (see Supplementary Fig. S1; Supplementary Data are available online at www.liebertonline.com/bfm). If women presented using all-purpose nipple ointment, 32 they were continued on this ointment. For all other women, mupiricin ointment was the initial ointment prescribed. Triamcinolone 0.1% ointment was added if evidence of inflammation or dermatitis was found. The initial visit typically lasted 60 minutes and included evaluation of latch, full feeding, and pump use if appropriate. In addition to suck assessment, infants were evaluated for thrush, torticollis, and ankyloglossia. In addition to detailed questions on pain, maternal history included assessment of milk supply and any report of vasospasm. If the history indicated possible vasospasm, mothers were instructed to use a heating pad for 10 minutes after feeds until the culture results were available. During the study women were offered OTX with failure of CTX. Treatment failure for CTX was defined as pain levels not improving as per patient report when pain levels and culture results were reassessed at the 5-day phone follow-up or at additional times when the patient contacted the clinic with concerns. Treatment failure for both CTX and OTX was further defined as weaning because of pain. When OTX was offered, the narrowest-spectrum antibiotic was chosen based on culture results, antibiotic sensitivities, and patient allergies. Dicloxacillin was the first agent of choice for narrow-spectrum antistaphylococcal penicillin. In penicillin-allergic patients either trimethoprim–sulfamethoxazole or clindamycin was chosen, depending on sensitivities. Pain levels, feeding patterns, and breastfeeding complications were collected at the 5-day phone follow-up, when culture results were available, and via e-mail questionnaires administered at 2, 4, 6, 9, and 12 weeks. All data were collected and managed using the REDCap electronic data capture tools hosted at Case Western Reserve University. 33

Flowchart of patients. f/u, follow-up.
Microbiological samples were obtained from the breast of the more painful side. If there was no difference in pain, the sample was obtained from the right breast. Nipple culture was collected first. The swab was rotated over the nipple/areola in a zigzag pattern as per the University of North Carolina culture protocol. 19 Following cleaning of the nipple/areola multiple times with an alcohol wipe, breastmilk was collected for culture in a sterile container. The specimens were labeled and transported at room temperature to Quest Diagnostics (Greentree, PA) for processing on both tryptic-soy agar with sheep blood and MacConkey's agar as previously described. 30 Both nipple and breastmilk cultures reported bacterial species identification. Breastmilk cultures reported quantitative bacterial growth.
Measures
Breast and nipple pain severity in the last 24 hours was rated by the patient at initial visit, phone call, and e-mail surveys in response to the questions “How bad has your breast pain been in the last 24 hours?” and “How bad has your nipple pain been in the last 24 hours?” Pain was rated on a numerical rating scale from 0 to 10, with 0 indicating no pain and 10 indicating the most severe pain. 34
At the initial visit and e-mail surveys women described the type and timing of their pain and categorically responded to questions on breast and nipple tenderness. Nipple exam findings were recorded categorically. Pain severity was further evaluated on physical examination by evaluation of breast tenderness upon manual expression of breastmilk by the clinician and nipple tenderness when the clinician lightly touched the mother's nipples on examination. Nipple and breast pain levels were recorded at initial latch-on in the office and following in-office correction of latch. All pain levels were rated on a scale from 0 to 10 (see Supplementary Data for measures used at the initial visit and surveys).
Descriptive variables and potential covariates, including history of breastfeeding problems, prior treatment history, current breastfeeding-related diagnoses, bacterial growth, and density, were collected from the study participants as previously described. 30 Breastmilk bacterial density was evaluated as a continuous variable reported as colony-forming units (CFU) per milliliter for each bacterial species.
Treatment, recorded at the initial visit and the phone call, included type of topical ointment and, if appropriate, type and length of administration of antibiotics. Antibiotic duration was recorded through initial prescription duration and compliance on e-mail surveys and confirmed with a chart review. Clinician assessment of other breastfeeding difficulties was recorded categorically as an indirect marker of CTX received, as was maternal response to questions on other treatment at the 2-week and 12-week survey (see Supplementary Data for measures used at the initial visit and surveys). Outcome data for weaning and breastfeeding complications were recorded as previously described. 30
Analyses
Eighty-nine cases were enrolled (Fig. 1). Once collected, the data were exported from REDCap to SPSS software (SPSS, Inc., Chicago, IL) and analyzed under the supervision of the project investigator. Descriptive statistical analyses were performed to examine the distribution and normality of data. The main analyses, testing the associations of CTX/OTX and breast and nipple pain level over time, were conducted on 86 cases.
Our primary analysis was to assess which clinical or bacterial variables predicted need for OTX. Clinical factors from history and exam findings, including pain severity, response to latch correction, pain timing, pain type, and microbiologic data, were evaluated. The primary outcome variable assessed was type of treatment: CTX or OTX. We used χ2 analyses to test the association between type of treatment and categorical factors and analysis of covariance to assess the relationship between type of treatment and continuous factors to control for covariates.
In our secondary analysis, we evaluated the secondary outcome variables, including pain levels, at the six follow-up time points and clinical outcomes. We analyzed the association of CTX and OTX with pain and clinical course. We used mixed between-within analysis of variance with repeated measures, controlling for important covariates, to assess the differences in breast and nipple pain at each time point and the rate of change between time points for CTX versus OTX. Adjusted mean pain scores were plotted separately for nipple and breast pain for the 12-week follow-up period for both the CTX and OTX groups.
Results
In our primary analysis we examined which baseline characteristics predicted response to conservative treatment. We tested the hypothesis that OTX would help pain severity in those patients not responding to CTX, and we analyzed microbiologic factors associated with failure of CTX.
Both CTX and OTX treatment groups had similar baseline characteristics with regard to maternal age, infant age, parity, breastfeeding intent, return to work, race, education, insurance, antibiotic treatment during delivery, and history of breastfeeding difficulties with the current infant. Those patients receiving OTX were significantly more likely to be multiparous mothers (24% vs. 54%, p=0.004). Treatment since delivery as well as current treatment with oral antibiotics, fluconazole, and topical antibiotics was similar between groups (Table 1).
Data are median (range) values or number (%) as indicated.
Pearson's χ2 test was used for dichotomous variables; the Mann–Whitney test was used for the median test.
CTX, conservative therapy; OTX, oral antibiotic treatment.
Baseline pain
We assessed if severity, type, or timing of pain was associated with failing CTX. Nipple and breast pain severity was significantly higher in those patients failing CTX and switching to OTX (Table 2). It is interesting that the OTX group had a shorter median number of weeks of chronic pain (3 weeks vs. 4 weeks; p=0.019), although this was not statistically significant upon correcting for multiparity (p=0.060).
Data are median (range) values, mean (SD) values, or number (%) as indicated.
Pearson χ2 test was used except in cases when the cell count was less than expected, and then Fisher's test was used. For continuous variables, the F test was used.
Adjusted for multiparous delivery by logistic regression for categorical variables, and analysis of covariance was used for continuous variables.
CTX, conservative therapy; OTX, oral antibiotic treatment.
On examination, OTX patients had statistically higher levels of breast tenderness on manual expression (7.2/10 vs. 6/10; p=0.026), nipple tenderness (6.6/10 vs. 4.3/10; p<0.001), cracked nipples (52% vs. 21%; p=0.004), and nipple pain with initial latch in the office (7.8/10 vs. 5.8/10; p=0.001). There was no difference between groups on pain type (Table 2). The time at which the pain occurred did not significantly differ for “pain immediately after” or “between feedings,” but “pain with feeding” was more likely with OTX compared with CTX (100% vs. 90%; p=0.021) (Table 2).
Latch correction
We next examined if response to latch correction predicted the need for antibiotics. Upon correction of latch technique, OTX patients were less likely to see improvement in nipple pain (56% vs. 82%; p=0.015) and continued with higher nipple pain severity (4.3/10 vs. 2.9/10; p=0.003). There was no statistical difference between OTX and CTX for other breastfeeding difficulties diagnosed at the initial visit (Table 2).
Bacterial frequency and antibiotic susceptibility
We next examined microbiologic factors associated with failure of CTX. Breastmilk bacterial culture analysis revealed significantly higher frequency of S. aureus growth in OTX compared with CTX patients (33% vs. 5%; p=0.001). Nipple culture revealed no statistically significant difference in the frequency of bacterial species. Growth of S. aureus in nipple cultures was higher in OTX (30%) compared with CTX (14.9%) patients; however, this was not statistically significant (p=0.11). Other species growth was similar between groups (Table 3). CNS and S. aureus were the two most common species identified. Antibiotic resistance patterns for S. aureus revealed 5% oxacillin resistant, 33% clindamycin resistant, and 0% trimethoprim–sulfamethoxazole resistant. CNS had a resistance frequency of 47% for oxacillin, 47% for clindamycin, and 20% for trimethoprim–sulfamethoxazole.
Data are number (%).
Pearson's χ2 test was used unless the cell count was less than expected, and then Fisher's exact test was used.
CTX, conservative therapy; OTX, oral antibiotic treatment.
We also evaluated microbiologic response to prior or current topical antibiotic treatment or OTX and found that breastmilk S. aureus growth was less likely if mothers had received either past (31.5% vs. 3.1%; p=0.002) or current (27.9% vs. 4%; p=0.013) topical treatment. Similarly, nipple culture S. aureus growth was less likely in mothers with past topical antibiotic use (39% vs. 0%; p=0.001) or current topical antibiotic treatment (35% vs. 0%; p=0.001). Prior oral use did not affect breastmilk culture results but did impact nipple culture for S. aureus and α-hemolytic streptococci. S. aureus was less common on those receiving prior oral antibiotics (30% vs. 8%; p=0.036), and α-hemolytic streptococci were more common (5% vs. 42%; p=0.002) (see Supplementary Table S1).
Quantitative bacterial growth
We next examined whether quantitative assessment of bacterial growth was associated with breast pain treatment requiring OTX. Only S. aureus colony count growth distribution was statistically different between groups (Table 4) (p=0.004). For all other bacteria, colony counts were not significantly different. Breastmilk colony counts revealed no growth of Acinetobacter, diphtheroids, Enterobacter, Enterococcus, Escherichia coli, Klebsiella, and Pseudomonas in >90% of the samples. Given the large number of cultures with undetectable growth, the median colony count was 0 CFU for all bacteria except CNS. Median colony count for CNS was 1,000 CFU/mL for both CTX and OTX (Table 4).
By independent-samples median test.
CFU, colony-forming units; CTX, conservative therapy; OTX, oral antibiotic treatment.
Pain and treatment and clinical course
We next analyzed pain severity over time. We tested the hypothesis that switching to OTX may help decrease pain severity for those patients failing CTX. All mothers received CTX with mechanical correction, lactation support, and topical ointments. To control for variations in CTX, we analyzed maternal use of other treatments during the first 2 weeks (Table 5) and did not find a significant difference. There also was no statistical difference between OTX and CTX on the frequency of the three most commonly prescribed ointments: mupiricin (81% vs. 68%; p=0.169), triamcinolone 0.1% (58% vs. 52%; p=0.591), and all-purpose nipple ointment (12.5% vs. 10%; p=1). Seven women in the OTX group (15%) received antibiotics at the initial office visit either because of planned weaning due to pain (n=5) or because of a high clinical suspicion for bacterial infection (n=2). For all other women, the decision to treat with OTX was made at the time of the phone call to discuss culture results (Fig. 1). Mean number of days from initial visit to phone call follow-up was 5 days (SD 1.6). Mean number of days from the 5-day phone call to the 2-week e-mail assessment survey was 11(SD 5). At the phone call antibiotic selection for women receiving OTX included dicloxacillin (25.6%), trimethoprim–sulfamethoxazole (22%), amoxicillin–clavulanic acid (3.5%), amoxicillin (1.2%), cefdinir (1.2%), clindamycin (1.2%), ciprofloxacin (1.2%), and azithromycin (1.2%).
Pearson's χ2 test was used unless the cell count was less than expected, and then Fisher's exact test was used.
p=0.074 upon controlling for S. aureus.
A repeated-measures analysis of variance was performed on the main effect of pain over time. Analysis of variance repeated without the seven women initially started on OTX did not significantly change the results. The main effect using Wilk's lambda showed that breast pain and nipple pain significantly decreased for both groups over time (p<0.001). A very large effect size was found for both breast (0.638) and nipple (0.754) pain. Changes in breast pain rating were statistically significant from the initial visit to 5 days, from 5 days to 2 weeks, and from 9 weeks to 12 weeks (Fig. 2).
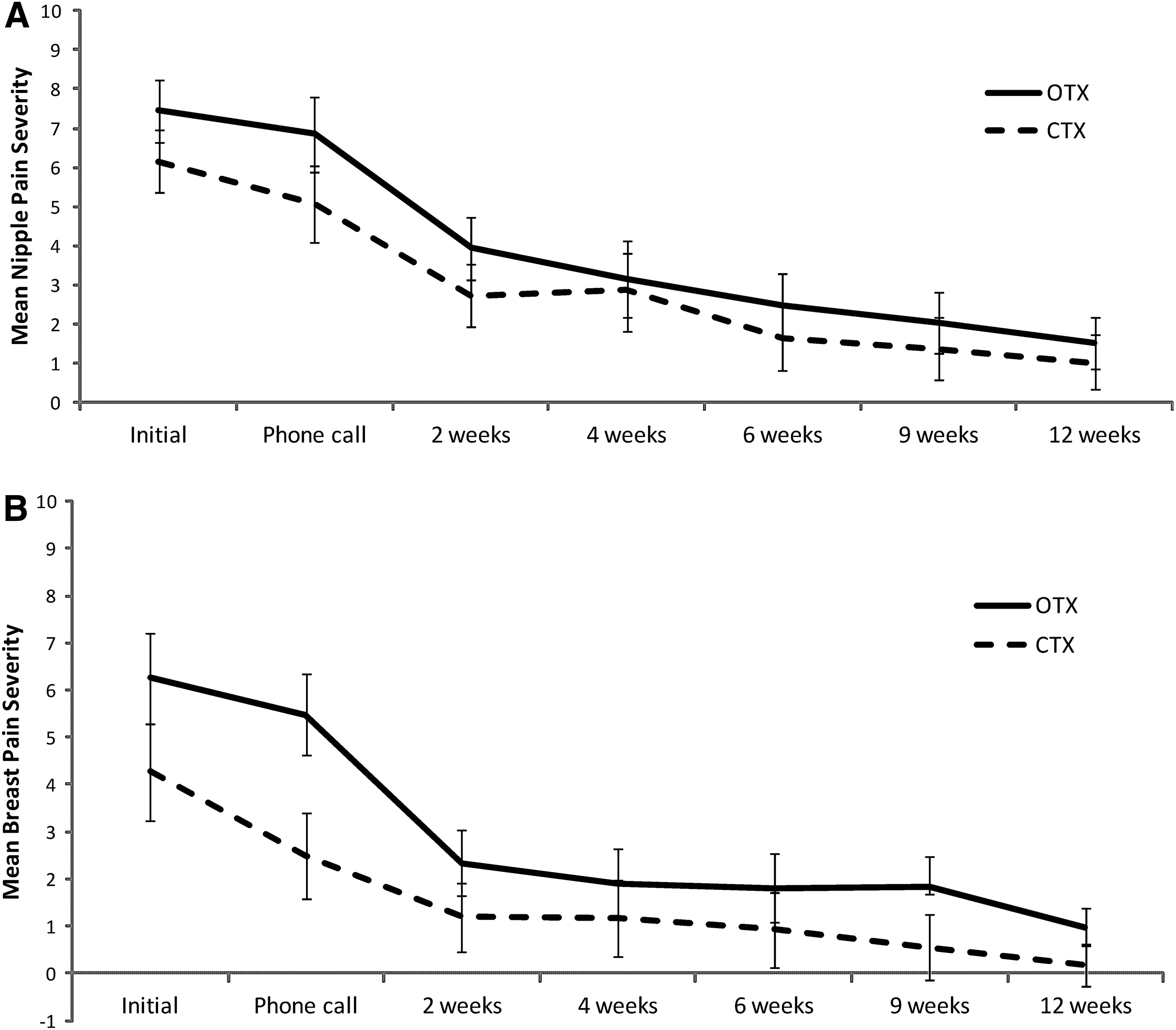
Pain in the conservative therapy (CTX) and oral antibiotic treatment (OTX) groups:
The amount of change from 5 days to 2 weeks differed significantly between the oral and topical treatment groups (p<0.001). From the initial visit to the phone call, breast pain improved by 1.8 points for those continuing CTX but only 0.77 points for those receiving OTX, which was not statistically significant. At the phone call, both nipple (7/10 vs. 4.8/10; p=0.001) and breast pain (5.8/10 vs. 2.5/10; p<0.001) continued at higher levels for OTX. Following the switch to antibiotics, breast pain levels dropped significantly for OTX patients between the phone call and the 2-week e-mail survey (3.1 points drop vs. 1.3 points drop; p<0.001) and continued to fall through the 4-week email survey, such that by 4 weeks there was no significant difference in nipple (3/10 vs. 3/10; p=0.139) or breast pain (1.8/10 vs. 1.4/10; p=0.088) between groups. At 6, 9, and 12 weeks there continued to be no statistical difference in nipple pain between groups (Fig. 1). Breast pain was not significantly different at 6 and 9 weeks, but at 12 weeks, although both OTX and CTX patients had pain levels less than 1 out of 10, the CTX group had statistically significant lower levels (0.18/10 vs. 0.98/10; p=0.007) (Fig. 2).
To further evaluate S. aureus, a repeated-measures analysis of variance examining the trajectory of pain over time for OTX with and without S. aureus growth did not reveal a significant difference at any time point (p=0.974), suggesting that improvement on OTX is not isolated to culture-positive S. aureus. Median length of antibiotic treatment was 14 days (range, 1–28 days; SD 6; 10 days, 25th percentile; 14 days, 50th percentile; 14 days, 75th percentile).
Outcomes
We analyzed if CTX was associated with a higher frequency of breastfeeding complications (Table 5). Twelve-week survey data were available for 83 out of the 86 study subjects. There was no significant difference in outcome data between groups. There was no difference in weaning frequency or reason for weaning between OTX and CTX. Reasons for weaning included pain (9% vs. 17%; p=0.332), low milk supply (3% vs. 3%; p=1.0), and separated from infant (2% vs. 5%; p=1.0). Exclusive breastfeeding did not significantly differ between the CTX and OTX groups during the course of the study: at enrollment, 74% versus 81% (p=0.625); 2-week survey, 82% versus 71% (p=0.242); and 12 week survey, 65% versus 54% (p=0.225).
Although women in the OTX were more likely to report mastitis during the study period (33% vs. 14%; p=0.044), this difference was not significant upon controlling for S. aureus (p=0.074). Review of the two women whose cultures grew S. aureus but who did not receive OTX revealed both were breast pain free at the end of the study. One developed a plugged duct that resolved, and neither developed mastitis or abscess.
Discussion
The primary findings of our study reveal that women with chronic breast pain who fail to respond to CTX are likely to have more severe nipple and breast pain on history and exam. They are less likely to have significant improvement in nipple tenderness on latch correction at the initial office visit and more likely to grow S. aureus on breastmilk culture. To our knowledge, this is the first study to prospectively look at history, exam, bacterial growth, and treatment response for women with chronic breast pain.
Commonly, clinicians rely on history and physical exam to guide decision making for chronic pain.12,20,22,27 It is interesting that in our study there was no clinically significant difference between groups with patient description on type of pain (i.e., shooting, feels like glass, etc.) or timing of whether pain occurred immediately after or between feeds. However, our data suggest that pain severity on history and exam, response to latch correction, and breastmilk cultures are more helpful guides to treatment response.
Prior microbiological studies on infectious causes of breast pain have identified Candida, S. aureus, and CNS as potential pathogens.6,26,31,35 Our study did not evaluate the role of yeast in chronic breast pain. This is a significant limitation of our study. Candida will grow on blood agar, but it is not the optimal medium. 36 Although two nipple cultures (and no breastmilk cultures) grew Candida, these findings are of limited significance. We designed our culture media and study to primarily study relative bacterial growth, and our findings support the proposal of S. aureus as a pathogen. It is interesting that breastmilk from those patients failing to respond to CTX grew other potentially pathogenic bacteria (Pseudomonas, Klebsiella, and E. coli). However, the small numbers limit statistical analysis. We saw no difference in CNS frequency or quantitative bacterial growth between CTX and OTX. The quantitative bacterial analysis, a study strength, addresses the theory that CNS and its potential overgrowth may be a cause of pain.12,31 Our findings do not support a pathogenic role for CNS. However, we did not evaluate CNS subtypes or virulence factors, a proposed explanation for CNS pathogenesis. 31 This was a study limitation. Although our study addresses some of the limitations noted in previous microbiologic studies, 6 larger, randomized, multicenter studies are needed to confirm which bacterial species are pathogenic.
If women do not respond to CTX, treatment with antibiotics, matched by bacterial sensitivity on breastmilk culture, may significantly decrease their breast pain. Given that the OTX group had significantly more rapid pain reduction upon treatment initiation, our study supports a role for OTX in the treatment of women with chronic pain not responding to CTX. Our median length of antibiotic treatment was 14 days, which is significantly less compared with other studies. 12
Our findings also suggest that breastmilk culture may be more helpful than nipple culture in the treatment of women with chronic breast pain who do not respond to CTX. Breastmilk culture helps identify S. aureus and other potential pathogens while providing targeted antibiotic treatment, thereby reducing length of antibiotic use. Further randomized controlled studies on CTX versus OTX are needed to evaluate which patients may benefit, to clarify treatment length, and to minimize overuse of antibiotics that may unnecessarily disrupt the milk microbiome and the infant gastrointestinal tract.
Our study was a prospective, descriptive study that has several limitations. We were unable to control for other causes of pain such as postpartum depression and vasospasm, although we did gather information on other breastfeeding difficulties and found no difference. Although vasospasm was not categorically measured, women in both groups routinely received initial conservative treatment for vasospasm with warm compresses. We also could not control for other antibiotic treatment by other physicians for non–breast pain-related diagnoses, nor did we exclude women with previous or current topical antibiotics. Although our analysis shows this is most likely to affect S. aureus growth, it is important to include these women in studies of chronic breast pain as they represent clinical practice where many women have received prior treatment. Our study addresses this limitation by examining prior and current use, which was not statistically different between groups. Future studies will need to continue to control for treatment history as well as to examine collection technique and culture interpretation in this setting. Outcome variables were by patient self-report and subject to reporting bias. Our patient population was educated with a strong intent to breastfeed, and therefore findings cannot be generalized to other populations.
It is important to note that we found pain reduction occurring over time in both groups and no difference in weaning between groups. The 12-week patient follow-up is a study strength. Given that complications were not higher in the CTX group and that both groups had significant pain resolution, our findings support an initial conservative approach. However, for mothers with persistent severe pain, despite differential evaluation and treatment for all causes of pain, further evaluation and consideration of oral antibiotics are warranted.
Conclusions
For women with chronic breast pain, pain reduces over time with conservative treatment including good lactation support and treatment with topical ointments. For those women not responding to CTX, OTX matched to breastmilk culture growth and sensitivity may significantly decrease their pain. Women with chronic breast pain whose cultures growing S. aureus are more likely to require OTX to resolve their pain. Further prospective and randomized studies, focusing on treatment of breastfeeding women with chronic pain, are needed.
Footnotes
Acknowledgments
Special thanks to Shelly Senders, MD, and the staff at Senders Pediatrics for their continued support in improving breastfeeding practices. We thank Mary Jane Mason for her assistance in the planning stages, Maya Bolman, Beth Hurd, and Anne Vanic for their excellent patient care and their assistance with data collection, and Kathleen Allen, MD, FCAP, FACB, and Diane Ashbaugh, BS, Microbiology M (ASCP), at Quest Diagnostics for arranging the laboratory tests needed to quantify breastmilk bacterial growth and CNS identification. This project was supported in part by a grant from HRSA DHHS/HRSA (D54 HP05444-01-00). This publication was made possible by the Clinical and Translational Science Collaborative of Cleveland (UL1RR024989/UL1TR000439) from the National Center for Advancing Translational Sciences component of the National Institutes of Health (NIH) and NIH Roadmap for Medical Research.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.