
Abstract
Abstract
Breastfeeding is recommended exclusively for the first 6 months of life, with continuation after the addition of complementary foods for at least 1 year of life. Breastfeeding rates are low in the Southeastern United States, especially among African Americans. Disparities in breastfeeding rates between African Americans and whites are especially pronounced in Memphis (Shelby County), TN. Our research objectives were to explore this disparity using focus groups, specifically to identify perceived barriers, and also to seek possible solutions from the target population. Focus groups were conducted in nine community settings within the county. Groups primarily consisted of women of childbearing years, but groups with men, grandmothers, and teens were also conducted. Common barriers for breastfeeding that were identified included pain, embarrassment with public nursing, going back to work, concern about “partying” and breastfeeding, and “just not wanting to” breastfeed. A notable finding was a substantial concern about sexuality and breastfeeding. As a possible solution, participants recommended putting breastfeeding educational materials widely across the county in many venues. Barriers to breastfeeding in Memphis are similar to those in other areas, with key concerns about sexuality and partying. Involving the target population yielded specific recommendations to improve breastfeeding promotion efforts.
Introduction
H
Evidence for the life-saving benefits of breastfeeding is overwhelming. The Surgeon General has reframed the discussion of the health benefits of breastfeeding, by highlighting excess risks due to not breastfeeding for both mother and infant. 5 Evidence for these excess risks is robust and includes an increased risk to infants for the following: respiratory infections, gastroenteritis, otitis media, obesity, diabetes, eczema, asthma, sudden infant death syndrome, and even certain types of cancer. 6 Among formula-fed preterm infants, the increased risk of necrotizing enterocolitis is substantial compared with infants fed breastmilk. 6 Mothers who do not breastfeed are at an increased risk of breast and ovarian cancer, 6 along with hypertension, hyperlipidemia, cardiovascular disease, and diabetes. 7 Cost savings associated with the risk reductions of these diseases have been estimated to be over $13 billion if 90% of mothers exclusively breastfed up to the recommended 6 months of life for pediatric illnesses 8 and $17.4 billion resulting from maternal premature death. 9
Despite the cumulative and compelling evidence for increased health risks, increased cost, and even increased risk of death within the non-breastfeeding mother/baby dyad, some women still choose not to breastfeed. Of great concern is the striking disparity in breastfeeding rates between African Americans and whites, with significantly lower breastfeeding rates among the African American population. As part of the National Immunization Survey, the Centers for Disease Control and Prevention noted this striking disparity in breastfeeding rates across the nation, with a 35% difference in 1990 for breastfeeding initiation between non-Hispanic blacks and non-Hispanic whites. 10 Today there remains a 20% difference in breastfeeding initiation rates among non-Hispanic blacks compared with non-Hispanic whites, with the largest differences in southeastern states. 11
The most recent Centers for Disease Control and Prevention National Immunization Survey documents that only 59% of Tennessee babies have any breastfeeding initiated and that only 4.1% are exclusively breastfeeding at 6 months. 12 These rates are far below the Healthy People 2020 goals for breastfeeding of 81.9% initiation, 60.6% at 6 months, and 34.1% at 12 months, as well as 46.2% exclusively breastfeeding at 3 months with 25.5% exclusively breastfeeding at 6 months. 13 Within the Tennessee African American population, the disparity in breastfeeding rates is striking, with the annual average 2004–2010 breastfeeding initiation of 44.7% for African Americans and 66.6% for whites. 14 Unfortunately, this extreme racial disparity in breastfeeding rates is even more pronounced in Shelby County, Tennessee, where the disparity has been approximately 35% over the past decade. Even for the most recent 2011 birth certificate data, only 52.6% of African American mothers even intend to breastfeed, compared with 82.1% of white mothers, a gap of nearly 30%. 14
In Memphis, TN, high rates of infant mortality, obesity, and diabetes are particularly problematic.15–17 Considering Memphis and Shelby County's high rates of infant mortality, obesity, and diabetes, all disparately increased among the African American population, breastfeeding remains an important vehicle by which to improve the health of the community.18–23 To identify the reasons for the extremely low breastfeeding rates among the African American population in Shelby County, Tennessee, we conducted a qualitative study with African American mothers, grandmothers, and fathers, to identify barriers they face, as a prelude for planning appropriate interventions.
Materials and Methods
Study design
We used focus groups to understand perceptions of barriers and identify persons who help motivate or influence breastfeeding in populations with low breastfeeding rates in Memphis. The study protocol was developed, including rationale for the study, informed consents, recruitment flyers, and questions for the focus groups, based on a literature review of current knowledge about breastfeeding disparities, barriers, and influences. Discussion topics included history of breastfeeding, sources of information, influences for initiating breastfeeding, barriers, and suggestions to increase breastfeeding rates. Specific questions asked in the groups are listed in Table 1. A doctoral student from the University of Memphis School of Public Health, with considerable experience in community research, was hired and trained to facilitate the focus groups. The Principal Investigator (J.L.W.) attended all focus groups, acted as recorder, and audio-recorded all sessions to ensure trustworthiness of the data. A transcriptionist was hired to transcribe the audio recordings. Signed informed consent was obtained from all participants. All data were maintained electronically in a password-protected computer, with the tapes and printed data (recorder notes) in a locked cabinet, to ensure confidentiality, privacy, and auditability. The research protocol was approved by the University of Memphis Institutional Review Board.
Selection of focus group locations and recruitment of participants
Community organizations servicing clients in locations with low breastfeeding rates were contacted to recruit participants from their clientele for focus groups. The following organizations agreed to participate: Agape Powerlines, serving children and families in under-resourced communities of poverty and homelessness; Christ Community Health Services, providing high-quality healthcare to the underserved in the context of distinctly Christian service; the Birthright of Memphis, a nonprofit helping any girl or woman, regardless of age, race, creed, or marital or economic status, who feels distressed by an unplanned pregnancy; Porter Leath, helping more than 10,000 low-income children and families with programs to meet their developmental, health, and social needs; Oasis of Hope, a nonprofit community-based Christian organization that changes hearts and lives by creating an “oasis” in the center of an urban neighborhood infamous for high infant mortality, poverty, and crime; Neighborhood Christian Center, building stronger families and neighborhoods by providing compassionate Christ-centered ministries to those in need; Baby Feat, courageous outreach of the Infant Mortality Force Memphis, a baby safety center geared toward education, prevention, health, and wellness for Memphis Babies; Nurse Family Partnership, a home visitation program to low-income first-time mothers; and Church Health Center, providing healthcare for the working uninsured and promoting healthy bodies and spirits for all. Recruitment flyers included announcement of a $20 incentive for each participant after completion of the focus group. The goal of recruitment for each group was to have six to 10 participants, as recommended to provide thematic saturation. 24 The types of groups were adult women of childbearing years, teen girls, grandmothers, and fathers.
Analysis
All data were transcribed verbatim. The responses of the participants were evaluated using the “Long Table” approach. 24 Themes and subthemes were determined, and responses were sorted and collated by the Principal Investigator (J.L.W.) and reviewed by a second expert in breastfeeding who is also an International Board Certified Lactation Consultant. Differences were resolved by discussion, and responses were categorized by age and sex if a trend was noted.
Results
Study population
Nine focus groups (86 participants) were conducted during the fall of 2011 at various community locations in Memphis. All participants were African American except for one Latino and one white woman. Most participants were native Memphians. Table 2 gives the demographic breakdown of participants by age.
Personal breastfeeding experience and history
Each participant was asked to state if she (or in the case of the men, if the mother of his baby) had personally breastfed a baby. Of the 77 participants who had children, 31 (40%) reported some previous breastfeeding, ranging from 2 weeks to 28 months (Fig. 1). The participants were also asked to recall if they themselves had been breastfed. Many participants were unaware of this information (40%), but of those who were aware (60%), about half recalled being told that they were themselves breastfed. Over half of the participants who knew they were breastfed also reported breastfeeding their own baby, compared with 21% of those who knew that they were not themselves breastfed.
Participants who have breastfed or are breastfeeding. The participants were asked to state whether they had breastfed or were currently breastfeeding at the time of the focus groups. For the men, they were asked whether their children had been breastfed. A participant was counted as having breastfed if at least one child was breastfed and that child was breastfed up to at least 2 weeks of age. Those who commented that they breastfed for 1 or 2 days were not counted in this group.
Personal influences
The first set of questions to all participants focused on overall influences of breastfeeding, to identify encouragers and discouragers. A majority (57%) of all participants stated that they had friends or family who had breastfed previously; similarly, 58% of the breastfeeding participants had friends or family who had breastfed. Many participants related that cousins, aunts, mothers, and grandmothers had breastfed, as well as friends. One participant noted her own employer, for whom she was a nanny, had breastfed four children and was an encouraging influence on her to breastfeed. Some female participants mentioned their brothers, whose children had been breastfed, as their influence.
Many participants noted that they were educated about breastfeeding by their doctors, nurses, Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) offices, various prenatal parenting classes, and family members. Some participants noted that “everybody” was encouraging them to breastfeed. Two participants mentioned their own father was the encourager; however, only one named the baby's father as an encourager. It is interesting that two participants specifically stated that no one talked to them about breastfeeding. When asked about people, institutions, and situations that discouraged them from breastfeeding, they frequently mentioned that their friends said breastfeeding hurt. Some women were discouraged if the baby did not get off to a good start breastfeeding. Several participants mentioned that fathers of the babies were discouragers.
The overall “most important influence” noted by the participants was themselves. Many said it was their own decision; they were determined, and they wanted to do the best for their baby's health. Several mentioned their own mother was the most important influence, but only two female participants mentioned the baby's father as the most important influence. Most fathers said that would leave the decision up to the baby's mother. Many who did not breastfeed said their most important consideration was pain or lack of time.
Knowledge of benefits to baby and mom
Participants were overall knowledgeable about the benefits of breastfeeding for the infants. They were especially aware of overall benefits to the immune system, including decreased occurrence of ear infections and other illnesses. Many participants mentioned that breastfeeding is the natural way to feed a baby, with the best nutrition and nutrients. Twelve participants mentioned the effects of breastfeeding to increase brain development and intelligence. Other common responses were improved bonding between breastfeeding mothers and their infants, as well as improved digestion with breastmilk. One participant mentioned reduced obesity among breastfed babies, and another mentioned decreased cancer risk.
Knowledge of benefits to mothers related to breastfeeding, or risks inherent in not breastfeeding, was more limited. Seven participants related knowledge of decreased incidence of breast cancer in mothers who breastfeed. The main benefit mentioned by most responders was rapid weight loss, or getting their shape back. Several also mentioned the special bond created by breastfeeding as a benefit to mothers as well as infants. Two participants mentioned decreased costs associated with breastfeeding, and several (especially grandmothers) noted its convenience.
Reasons for African American women in Memphis not to breastfeed
Participants were asked for their opinions about the African American population of Memphis as a community: specifically, why women did not even choose to start breastfeeding, and why women stopped after starting breastfeeding. Table 3 lists the prominent themes expressed across all focus groups, which included concerns about pain, nursing in public, going back to work, and fear of sagging and that it “wasn't right” for a baby to be suckling on a mother's breast, with many concerns about sexuality and breastfeeding. A novel theme emerged: concern about “partying” and breastfeeding.
Biggest barrier
After these discussions, each participant was then asked to name what she or he thought was the “biggest barrier” to breastfeeding. The most commonly cited barriers to breastfeeding were drugs and partying, laziness, and just not wanting to breastfeed. A lack of knowledge, pain, inconvenience, and the WIC program were also mentioned (Fig. 2).
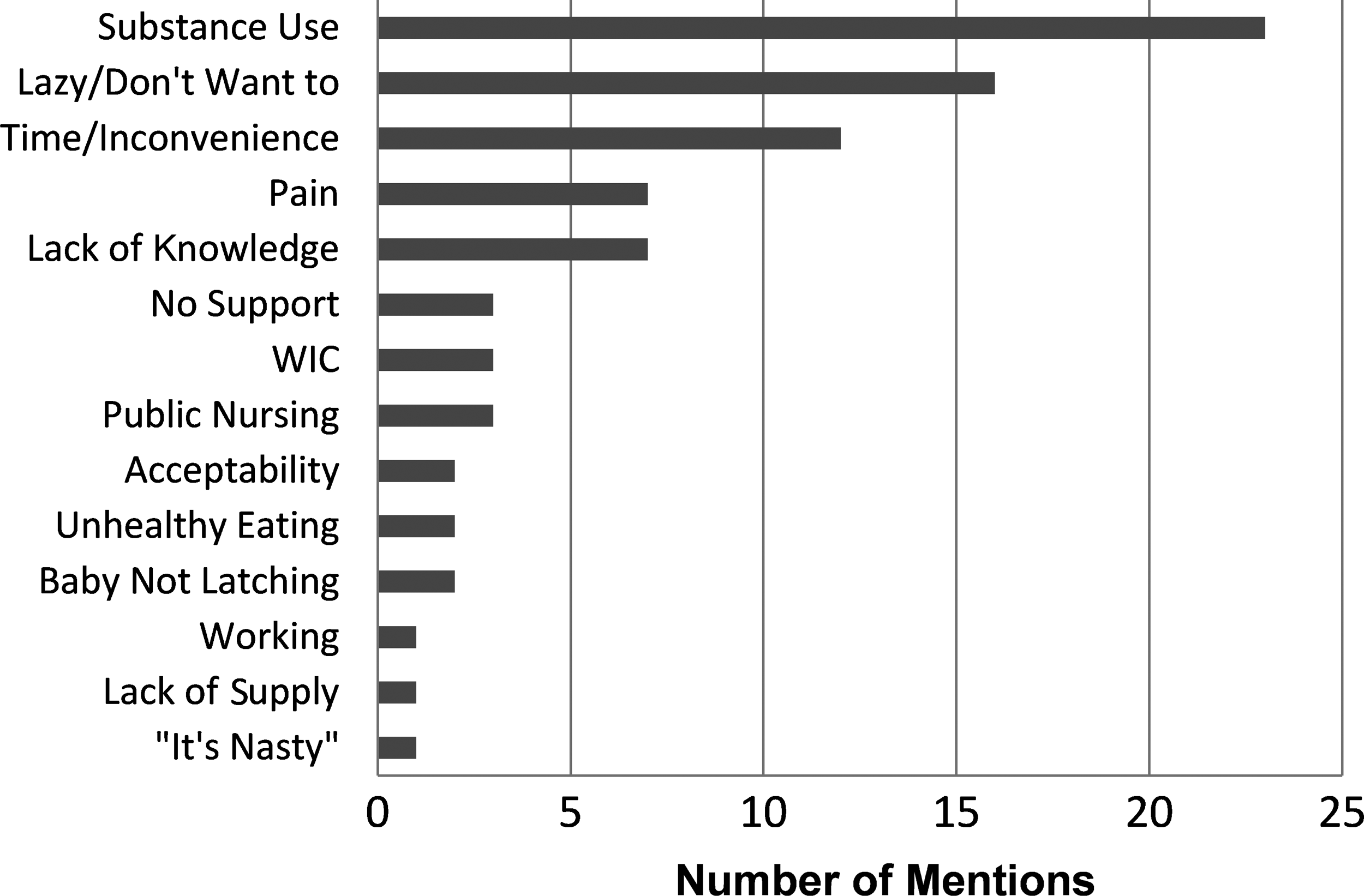
Biggest barrier to breastfeeding. After discussion of the many barriers noted in Table 3, the focus group participants were asked to identify the biggest barrier, in their opinion, to breastfeeding. The results were tallied, and their answers are shown here, illustrating a wide variety of personal, medical, and social reasons to not breastfeed. WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
If there was one thing…
Participants were then asked to think of solutions to breastfeeding barriers they had identified, identifying the “one thing” to make a change in how women choose to feed their babies. The most frequently stated solution was to provide more information and education to the women of Memphis, which should be located “everywhere” around the community, including doctors' offices, schools, hospitals, churches, and even locations such as juvenile court and the post office. Educational efforts mentioned were free classes, home visitation programs, support groups, programs in the schools and churches, and incentivizing programs, including rap or other youthful avenues into breastfeeding education. Several recommended more advertisements and billboards about breastfeeding. One stated, “They promote everything else; why not promote breastfeeding?” Several mothers said breast pumps need to be provided for breastfeeding mothers, and some men agreed with pumping to avoid breastfeeding in public.
Discussion
Many factors work together to influence a mother's feeding choice for her infant. Known predictors of choosing not to breastfeed include the following: low income, lower education, younger age, employment outside of the home, lack of role models, lack of peer and family support, fear of pain, and lack of support from healthcare providers. 25 The consensus of data suggests that African Americans have disparately low rates of breastfeeding intention, initiation, and duration 5 even after controlling for various sociodemographic variables.26,27
This focus group study was designed to identify the barriers to breastfeeding within the African American population of Memphis, a target population with extremely low breastfeeding rates and a disproportionate share of adverse health outcomes. In addition to identifying the barriers and influences to breastfeeding in Memphis, possible solutions were elicited from focus group members.
Our cohorts seemed representative of the African American breastfeeding experience in Memphis, in that 31 of 77 (40%) of participants initiated breastfeeding (Fig. 1), similar to the 2004–2010 annual average Shelby County birth certificate data where only 44.7% of African American women expressed intention to breastfeed. 14 We observed that African American mothers in these Memphis focus groups derive support from grandmothers, extended family, and friends; however, only a few mentioned support from fathers of the babies. Some of our participants noted that even their own fathers were supportive. Although only half of the participants knew their own breastfeeding history, those who did know that they had been breastfed were more likely to breastfeed their own babies, as has been noted as an influencing factor previously. 28 Clearly, the interpersonal sphere of influence affects a mother's decision to breastfeed in Memphis as across the nation.29,30 When breastfeeding is not the norm in the interpersonal sphere, these key influencers can provide support or discouragement. Furthermore, Memphis African American women, men, and grandmothers in the focus groups were very aware of the many benefits the baby receives from breastfeeding, although they were not as well versed on the benefits to mothers. These perceived health benefits did not translate into changed behavior or an increased likelihood of breastfeeding, however, because of many barriers they perceive and experience.
Some barriers to breastfeeding within the Memphis African American population were similar to those found across the nation (Table 3). Women were concerned about pain, whether they had already nursed and experienced pain themselves or just heard “stories” about painful nursing; even the men said that “pain” was a significant barrier to breastfeeding for the women they knew.31–34 Going back to work was noted as a barrier to breastfeeding, as was lack of support or role models and lack of knowledge about how to breastfeed.34–36
Public nursing was a particularly significant concern to many participants here as it is nationally,37–39 even to the point of disgust when they saw other women nurse in public. Several women commented that white women nursing their toddlers in public were particularly disturbing to them, especially if the nursing mother was not discreet. This consensus was definitely seconded by male participants, stating they do not want the mother of their child to nurse in public. It is notable that several men mentioned that public places needed private locations for women to nurse, similar to previous findings that low-income individuals and African Americans are most likely to accept breastfeeding policies that establish lactation rooms in public places. 38 It is interesting that our participants did not mention the Tennessee law protecting a mother's right to breastfeed wherever she has the right to be. 40 Public nursing is not the cultural norm for this target population and therefore is a definite barrier to breastfeeding, as moms on the go with babies will need to feed them when they are hungry, wherever and whenever that occurs.
Another striking and consistent theme in this African American population was the concern about breastfeeding and sexuality. This may be tied to concerns about public breastfeeding, because our men's group verified that breasts attract attention. Sexualization of the breast as a deterrent to breastfeeding has been reported, 41 but this theme was striking among all age groups, including one grandmother who mentioned the possibility of inciting rape if a mother was seen nursing in public. Several young mothers stated it just didn't “feel right” to have the baby “sucking on the nipple.” The women were vivid with stories and comments they received from the baby's father or other men, typically negative attitudes about breastfeeding. Tied to the theme of sexuality of the breast was the barrier of potential future sagging of the breasts. From having to wear push-up bras to losing her “core,” this was a definite concern among focus group participants. As long as breasts are seen as sexual objects, their appearance will influence a mother's decision to breastfeed.
A novel theme mentioned by our participants was that “partying,” or mothers' drug, alcohol, and tobacco use, was a major barrier to breastfeeding. It is interesting that many participants felt this was a significant problem in Memphis. However, they were speaking of other mothers, and especially young mothers, but not specifically about themselves. The American Academy of Pediatrics lists illicit drug use as a specific contraindication to breastfeeding, although alcohol and smoking are not, presuming the mother only has “one single celebratory drink” and that she smokes away from her baby. 3 Our finding that a barrier to breastfeeding among young Memphis mothers may be illicit drug use and partying creates an opportunity to work toward eliminating this barrier by providing resources to help them quit the offending behaviors. Home visitation programs have shown some promise in curtailing maternal drug use and prolonging breastfeeding, 42 but close follow-up is an absolute imperative in these atypical cases.
With the many identified barriers to breastfeeding that women in Memphis face, the answers to the question “What is the ONE THING we can do to help more women in Memphis breastfeed?” are crucial to examine before future planning of interventions to support Memphians. Information and education were the top suggestions, and it is interesting that the various modes of information and education dissemination mentioned by the participants are in agreement with several of the Surgeon General's Action Steps to support breastfeeding. 5 Our participants requested support for the mothers and extended family, as well as convenient classes for family members to attend, including such venues as churches, community centers, and schools. Several participants also mentioned improving education through various home visitation programs and recommended different kinds of media to reach the target population, such as video and rap, which fits into the Surgeon General's Call to Action to Support Breastfeeding. 5 To the follow-up question, “Where should we have breastfeeding information in Memphis?,” the focus group participants responded “Everywhere!” and suggested clinics, hospitals, churches, schools, and even juvenile court and the food stamp office—in effect, a saturation of the city with breastfeeding information. The focus group participants also mirrored the Surgeon General's Call 5 by suggesting images of breastfeeding be placed around the city. They offered opinions about billboard and bus stop images to help the Shelby County Breastfeeding Coalition's plan for a media campaign.
One study limitation was that participants knew they were recruited to talk about breastfeeding. Although the recruitment flyer specifically stated that opinions were sought with “No Wrong Answer,” it is possible that participants may have had special interest and knowledge of the topic and were not representative of the target population at large. Another potential limitation of the study was the small groups of teens in two locations. Finally, given the qualitative nature of the study, and the relatively small sample size, the information collected here must be considered exploratory and hypothesis generating, rather than hypothesis testing.
The local implications of this study are considerable. The mere process of reaching into community groups and seeking opinions about breastfeeding was of great importance to participants. Several participants thanked us for asking for their opinions. Some stated they “learned a lot” in the groups, although there was no specific teaching by trained individuals during these sessions, and they were learning only from each other. Four of the nine sites have requested a follow-up breastfeeding class.
Conclusions
This qualitative study has delineated significant barriers to breastfeeding among African Americans in Shelby County, Tennessee. In addition to previously mentioned difficulties with pain, reluctance to breastfeed in public, and concern about the time involved, our focus groups identified important issues about partying while breastfeeding and a prominent concern about the sexuality of breastfeeding. It is important that the focus groups offered specific suggestions about ways to overcome these barriers with special emphasis on broad education and public awareness. These results will be incorporated into a future public campaign.
Footnotes
Acknowledgments
The authors thank Joni Rose, RD, IBCLC, who served as a secondary reviewer of thematic responses, Pamela Giacosa, who transcribed the audiotapes, and Vikki Nolan, DSc, MPH, who reviewed the manuscript in its early stages. The study was funded by a CATCH grant from the American Academy of Pediatrics awarded to the Principal Investigator (J.L.W.).
Disclosure Statement
No competing financial interests exist.