
Abstract
Abstract
Introduction:
Breastfeeding difficulties are sometimes attributable to tongue-tie with short-term relief after frenotomy. Limited follow-up is available, and predictors for nonsuccessful frenotomy have not yet been found.
Patients and Methods:
We recruited 264 mother–infant dyads who underwent lingual frenotomy for breastfeeding difficulties. Data regarding the indications, anatomy of the tongue, and the response of the infant were noted by the physician. Mothers were contacted by telephone at 2 weeks, 3 months, and 6 months after frenotomy to answer a questionnaire.
Results:
Two weeks after frenotomy, 89% of mothers were still breastfeeding. An improvement in breastfeeding was reported by three-quarters of the mothers, but, unexpectedly, 3% reported worsening. At 3 and 6 months after the procedure, 68% and 56% of mothers were still breastfeeding, respectively. We could not find any predictor to indicate those infants in whom breastfeeding would not improve.
Conclusions:
There are favorable long-term effects of frenotomy on breastfeeding. Lingual frenotomy does not always alleviate breastfeeding difficulties, and rarely worsening ensues. We could not find any predictor for successful breastfeeding after frenotomy. We speculate that because the procedure is minor, in the event of breastfeeding difficulties, lingual frenotomy should be considered as an effective tool to assist in long-term breastfeeding.
Introduction
B
We conducted this prospective study on maternal evaluation of their experience in breastfeeding over a 6-month period after their infants underwent frenotomy. Our aim was to amass follow-up data on these mother–infant dyads and to search for predictors of breastfeeding success following frenotomy.
Patients and Methods
All mothers of infants who had breastfeeding difficulties for which they underwent lingual frenotomy either at bedside or as an office procedure were eligible for study enrollment. Approval of the institutional board of human experimentation and the Israeli Ministry of Health was obtained, and all participating mothers signed an informed consent form. By design, only term infants with no congenital anomalies were included. There were no other exclusion criteria for participation in the study.
A questionnaire that included items describing the indications for the procedure, the anatomy of the tongue, a description of the procedure, and the response of the infant in terms of breastfeeding behavior was filled in by the physician who performed the frenotomy. Breastfeeding problems included failure to latch (i.e., repeated detachments from the nipple, inability to latch, falling asleep on the breast), sore nipples, and pain while breastfeeding or nipple bruising. Mothers were contacted by telephone (by the research assistant Carmit Golan) at 2 weeks, 3 months, and 6 months after the lingual frenotomy, and their responses to standardized items on a separate questionnaire were recorded.
Between March 2010 to October 2010, we recruited 264 mothers whose infants underwent lingual frenotomy at a median age of 14 (range, 1–135) days of life. All frenotomies were performed after evaluation by a lactation consultant that ruled out other reasons for breastfeeding difficulties, who also referred most of the infants. Data on breastfeeding difficulties in terms of nipple soreness, pain, or bruising were recorded, as well as visual anatomy of the frenulum and tongue and immediate outcome of the procedure (i.e., wound size, bleeding, and other complications). The procedure was performed as described elsewhere, 6 and all the mothers expressed their interest in continuing breastfeeding afterward. The procedure was performed by one of the authors (S.D. or E.B.), both with over 10 years of experience in this procedure. Parents were advised to give acetaminophen when pain was suspected. Descriptive statistics are given as median, mean, and standard deviation for ordinal and continuous variables and as frequency distribution for categorical variables. Relationships between ordinal or continuous variables were examined using the Mann–Whitney test. Relationships between categorical variables were tested by Fisher's exact and the chi-squared test as applicable. Statistical analyses were performed using SAS for Windows 9.2 software (SAS Institute, Cary, NC).
Results
During the study period, 7,679 infants were delivered in our hospital. Twenty of the 264 mothers were excluded from the study: 17 failed to fill out the informed consent form properly, two were not available for phone interview, and one declined to participate. There were 143 male infants and 101 females, all of Jewish parentage. Further demographic data are given in Table 1. Some questions were not answered by all mothers, so that results do not add up to 100%. The maternal reasons for referral for their infants' frenotomy were mostly maternal nipple soreness (203 mothers, 83%), with most mothers reporting severe nipple pain with bruising (152, 62%) or without (92, 38%) bruising. Latching difficulties were described by 134 mothers (55%), mostly in the form of repeated, frequent detachments of the infant from the breast (64%). Inability to feed (7%), falling asleep on the breast (7%), and other latching problems were also reported. Frenulum description according to the Coryllos classification 3 revealed that types I, II, and III were more prevalent in male infants, whereas type IV was similar between the genders (Table 1).
Average±standard deviation pain score by visual analog scale (from 1 to 10)=7.3±2.1.
Visual analog scale from 1 to 10.
F, female; M, male.
All 244 study infants underwent the frenotomy procedure with minimal discomfort and minimal bleeding. It is interesting that there were no significant correlations between the Coryllos type of frenulum 3 (type 1, at the tip of the tongue; type 2, behind the tip if the tongue; type 3, mid-tongue; type 4, against the base of the tongue) and the reasons for performing the procedure.
Two weeks following frenotomy for breastfeeding difficulties, an improvement was reported by 180 of the mothers (75%), of whom 131 (54%) considered the improvement as being significant. There was no improvement according to 48 mothers (20%), and seven (3%) reported worsening of the breastfeeding problems, causing cessation of lactation. Of the 130 mothers who had nipple wounds, 50 (38%) reported wound disappearance by the fourth day after the frenotomy. Our study was not powered to test the age of the infant at the time of frenotomy and its effect on breastfeeding success. The mothers reported that fibrin deposition over the wound disappeared within a median of 9 days (range, 2–14 days).
Most of the infants (217 of 244, 89%) who underwent lingual frenotomy for breastfeeding difficulties were still being breastfed at the 2-week follow-up: 160 (74%) were fully breastfed, 28 (13%) received more than half of their meals as breastmilk, and 29 (13%) were fed half or fewer of their meals as breastmilk. Twenty of the 27 mothers who stopped breastfeeding reported doing so because of difficulties that were not solved by the frenotomy (e.g., nipple pain or bruises, latching problems, breast engorgement, etc.). Thus, around 90% of the original breastfeeding problems were alleviated by the frenotomy.
At the 3-month follow-up, 165 of the study population (68%) were still breastfeeding, of whom 134 (81%) were fully breastfed. Of those who stopped breastfeeding during this period, about half reported unresolved breastfeeding difficulties as the reason. Slightly over one-half of the infants (137 of 244, 56%) were still breastfeeding after 6 months. Despite lower rates of breastfeeding initially, longer-term changes in rates of breastfeeding for the study population were better in comparison with the general Israeli Jewish population (Fig. 1). We could not demonstrate any statistically significant predictor in terms of history of breastfeeding of siblings, symptom (e.g., pain, bruising), or anatomy (e.g., Coryllos type and thickness of the frenulum) for improvement in breastfeeding at any of the examined time points.
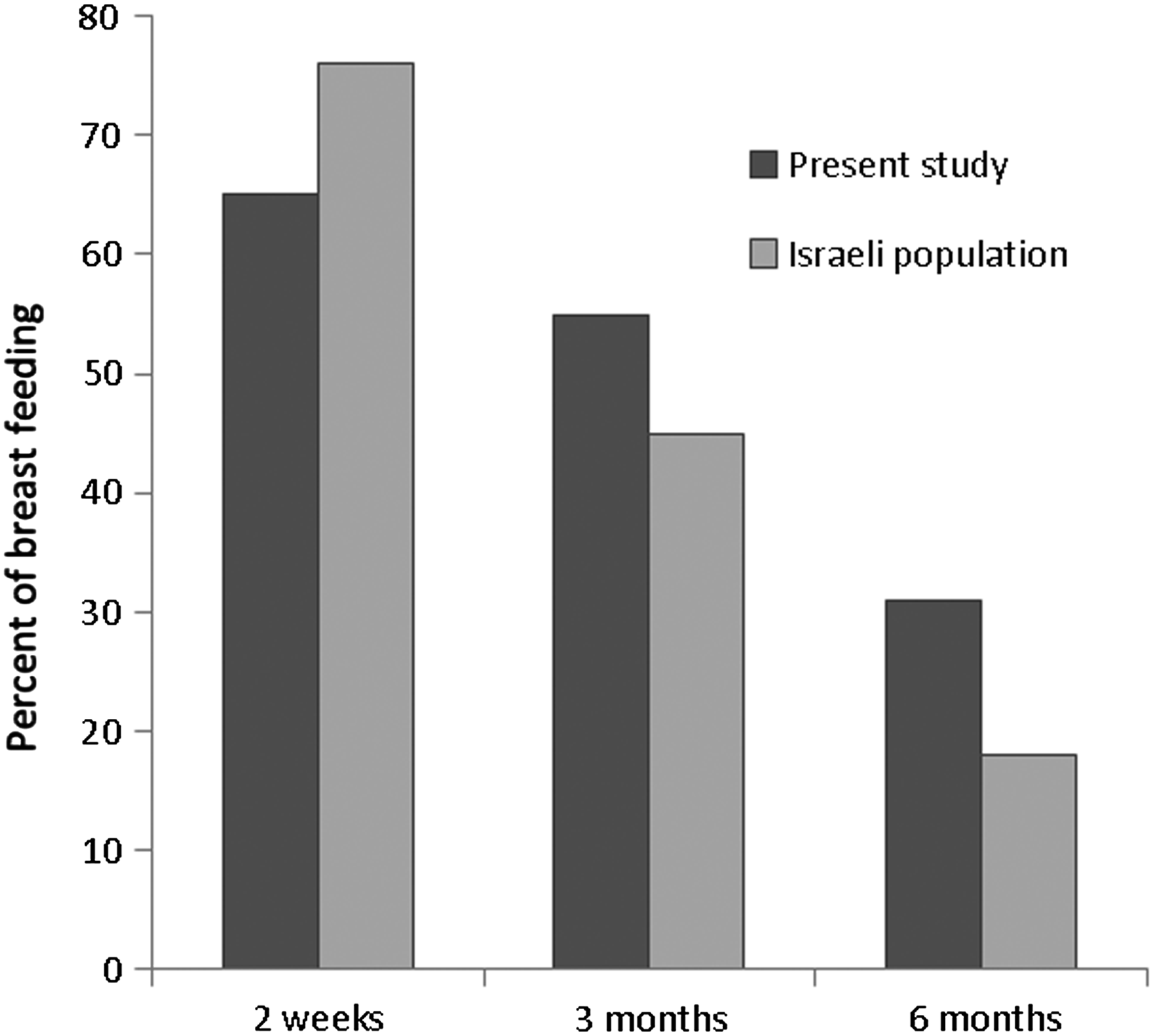
Breastfeeding rates of the study population compared with the general Israeli Jewish population for fully breastfed infants. Note that data for the general Israeli Jewish population are age of infants, whereas data for the present study are time after frenotomy.
Discussion
The results of this study showed an improvement in nipple pain and latching difficulties in 75% of the mothers of infants with breastfeeding difficulties who underwent lingual frenotomy. Moreover, 89% of infants were still breastfeeding at 2 weeks post-frenotomy, 68% at 3 months, and 56% at 6 months. The procedure itself was regarded by both the mothers and the physician as essentially nontraumatic, with minimal bleeding or pain and without noticeable complications. Difficulties in breastfeeding may be influenced by the breastfeeding technique, 7 anatomy of the infant's mouth (e.g., tongue-tie), and the anatomy of the maternal breast and its match to the neonatal mouth. 8 Despite vast experience in performing lingual frenotomy for breastfeeding difficulties, it is well accepted that some frenotomies do not result in significant improvement of breastfeeding.2,6 Each of our study participants was followed up for over 6 months after frenotomy. Around 10% of the mothers discontinued breastfeeding because of difficulties not resolved by the frenotomy, and 3% reported worsening of breastfeeding difficulties to a degree that they stopped breastfeeding completely. From the history of breastfeeding of siblings, symptom of maternal nipple pain or bruising, or the Coryllos type and thickness of the frenulum, no predictor for improvement in breastfeeding was statistically or clinically apparent at any of the examined time points. A previous report on follow-up of infants undergoing lingual frenotomy was published by Griffiths. 6 In his study, a follow-up of 3 months was conducted by telephone interview and, like in the present study, showed higher breastfeeding rates compared with the population and could not define predictors of success in performing frenotomies but reported somewhat lower rate of breastfeeding deterioration. The reason for this worsening of breastfeeding difficulties is not clear. It could be a complication of the procedure itself, following limited tongue movement secondary to the painful wound. Alternatively, it could result from a failure of the frenotomy to solve the breastfeeding difficulty, which could worsen with the increasing demand of the infant for more breastmilk as he or she continues to grow.
Figure 1 gives the comparison of full breastfeeding rates at each of three follow-up points between our study group and the general Israeli Jewish population. 9 Despite the lower rates of breastfeeding initially, perhaps attributable to the breastfeeding difficulties in our study infants, the rates of full breastfeeding at both 3 and 6 months of age were markedly higher (Fig. 1).
We are aware of several limitations to this study. Much of the data were obtained by interviewing the mother, which may introduce a bias in reporting. In addition, our population was not randomly selected but rather consisted solely of mother–infant dyads with breastfeeding difficulties and highly motivated mothers. A limitation of the comparison between the rates of breastfeeding in our population and Israeli data is that the Israeli data are derived from age-related information, whereas our study population was evaluated at three time points after frenotomy. This difference is in a magnitude of about 14 days, as this was the median time of frenotomy. However, similar results reported at 3 months by the study of Griffiths 6 support the validity of our results.
Conclusions
From our data we conclude that there are favorable long-term effects of frenotomy upon the prevalence and length of breastfeeding in a population of infant–mother dyads with breastfeeding difficulties. Additionally, subjective reports by the mothers after 2 weeks testified to an improvement in breastfeeding experience. Lingual frenotomy does not always alleviate breastfeeding difficulties, and worsening of those problems can occur, albeit rarely. We could not find any predictor for successful breastfeeding after frenotomy in our population. We suggest that because the procedure was reported as being minor by the infants' mothers, in symptomatic babies, following review and support from a trained lactation consultant, frenotomy of tongue-tie will improve breastfeeding rates with minimal morbidity.
Footnotes
Acknowledgments
Esther Eshkol is thanked for her editorial assistance. Carmit Golan, BSc, is thanked for her research assistance.
Disclosure Statement
No competing financial interests exist.