
Abstract
Abstract
Introduction:
Although children with attention-deficit/hyperactivity disorder (ADHD) were reported to have insufficient breastfeeding, consequences and oropharyngeal implications of this finding have not been studied. In this case-control study, we aimed to investigate early feeding practices and parafunctional oral habits in children with ADHD.
Subjects and Methods:
The study group consisted of 200 children and adolescents, 7–17 years old, diagnosed as having ADHD at Marmara University Child Psychiatry Clinics in Istanbul, Turkey. The Conners Parent and Teacher Rating Scales were used to assess behavioral disturbances. A questionnaire was developed consisting of items pertaining to breastfeeding period, early feeding history, and parafunctional oral habits. The study data were compared with those for 175 healthy schoolchildren after exclusion of possible ADHD cases.
Results:
The children with ADHD were found to have insufficient exclusive breastfeeding (less than 6 months) (p=0.0001). The children with insufficient exclusive breastfeeding were more likely to have a history of bottle feeding, longer duration of bottle feeding, and early introduction of bottle feeding (p=0.01). Overall, significant differences were detected on the domains of duration of bottle feeding, introduction of bottle feeding, introduction of pacifier use, variables of nail and toenail biting, as well as pencil biting, bruxism, and snoring between the ADHD group and the control group.
Conclusions:
The present results indicate that early in life, children with ADHD are subject to insufficient exclusive breastfeeding, different feeding practices, and elevated parafunctional oral habits more often than typically developing children. For all professionals who provide healthcare to children, increased awareness and attention to these factors are suggested.
Introduction
A
Several studies have revealed environmental and biologic factors that may increase the risk of ADHD. 1 Absence or short duration of breastfeeding is among the postnatal risk factors found to influence the course of the disorder. 3 Breastfeeding offers many benefits like prevention of infant morbidity, mortality, and chronic diseases, increased mental development, improvement of maternal health, and better economic costs. According to the World Health Organization, breastfeeding should be initiated within the first hour of life and continued exclusively for the first 6 months and then, until 2 years of age, with adequate complementary foods. 4 Among the consequences of insufficient breastfeeding exist several parafunctional behaviors and oropharyngeal conditions; however, this dimension has not been studied in children with ADHD. 3
The less children are breastfed, the more they are bottle fed and engage in non-nutritive sucking habits, which negatively affect their dentofacial development. 5 When children satisfy their instinctive sucking urge with prolonged use of pacifiers or by sucking their thumbs, non-nutritive sucking habits occur. 6 Children with bottle feeding or complementary feeding show a higher risk of acquiring parafunctional oral habits after the first year of life, which are associated with a greater risk of malocclusions like crossbite, open bite, and Class II molar relationship. 7 Disordered dentofacial development is associated with further health problems, such as sleep-disordered breathing. 8 Of particular note is that the impact of sleep-disordered breathing specifically on “executive functions,” which include cognitive flexibility, task initiation, self-monitoring, planning, organization, and self-regulation of affect and arousal, may produce ADHD-like symptoms. 9
Because certain issues relating to insufficient breastfeeding have not been addressed in children with ADHD, we aimed to investigate them in this study.
Subjects and Methods
The approval of the local ethics committee of Marmara University Medical School was granted, and informed consent was obtained from parents who agreed to participate in the study.
The study group consisted of 200 children and adolescents, 7–17 years old, who were admitted to the Marmara University Hospital Child Psychiatry Outpatient Clinics and diagnosed as having ADHD. The mothers and children, receiving healthcare within the Social Security Fund, belonged to families of low to medium socioeconomic status. Data were collected from eligible consecutive cases over a 3-month interval. The mean age was 10.25±2.52 years; there were 150 boys (75%) and 50 girls (25%).
Psychiatric diagnoses were based on Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria. 10 Children with comorbid neurologic disorders, psychosis, pervasive developmental disorders, and mental retardation were not recruited into the study.
In order to establish a control group, permission was obtained to collect data from three elementary schools located in Istanbul. These schools were chosen from the shortlisted schools in the catchment area of the hospital with similar socioeconomic status. The control group consisted of Grade IV healthy schoolchildren matched for age of the study group. Of the 300 parents asked to complete the survey, the parents of 184 (61%) students responded. In order to exclude possible ADHD children, the 5% of children who scored highest on the Conners questionnaires were removed from the control group. The remaining sample consisted of 89 girls (51.9%) and 86 boys (48.1%), a total of 175 children. Control data were collected over a 2-week interval.
Questionnaires
A questionnaire was developed consisting of items pertaining to breastfeeding period, bottle feeding experiences, non-nutritive sucking habits, mouth breathing, and malocclusion problems. Exclusive breastfeeding was defined as an infant receiving only breastmilk from his or her mother or a wet nurse, or expressed breastmilk, and no other liquids or solids, not even water, except for necessary medications. 4 Complementary feeding was defined as the process initiated when breastmilk is no longer sufficient to meet the nutritional requirements of infants, and therefore additional foods and liquids are needed, along with breastmilk. 4
Conners Parent Rating Scale
The Conners Parent Rating Scale (CPRS) is a form of 48 items, rated by parents, that aims to evaluate the child's behavior across the domains of hyperactivity, inattentiveness, oppositional behavior, psychosomatic behavior, and irritability. 11 A valid and reliable Turkish version was used in this study. 12
Conners Teacher Rating Form
The Conners Teacher Rating Form (CTRF) is a form of 28 items, rated by teachers, to evaluate the child's behavior at school. 13 It consists of hyperactivity, inattentiveness, and conduct problems subscales. A valid and reliable Turkish version was used in this study. 14
Statistical analysis
Statistical Package for the Social Sciences software (version 11.5; SPSS, Inc., Chicago, IL) was used for statistical analysis. Chi-squared tests were used to compare categorical variables, and t tests were used to assess patterns involving continuous variables. Correlational tests were also performed to investigate relationships between certain variables. We also conducted logistic regression analysis to assess variables predicting ADHD diagnosis. A probability value of p<0.05 was taken as the significance level.
Results
Duration of exclusive breastfeeding in the ADHD group was 4.45±2.98 months, whereas it was 6.85±4.89 months in the control group (t=5.79, p=0.0001). The number of children who were never breastfed and breastfed less than 6 months was significantly higher in the ADHD group (n=103; χ2=14.53, p=0.0001). Figure 1 displays the percentages of the children who had insufficient early breastfeeding. Duration of exclusive and complementary breastfeeding together in the ADHD group was found to be 12.74±10.13 months, in contrast to 13.38±9.31 months in the control group, a difference that was not significant. No significant difference existed between boys and girls in both groups in regard to the variables explored.
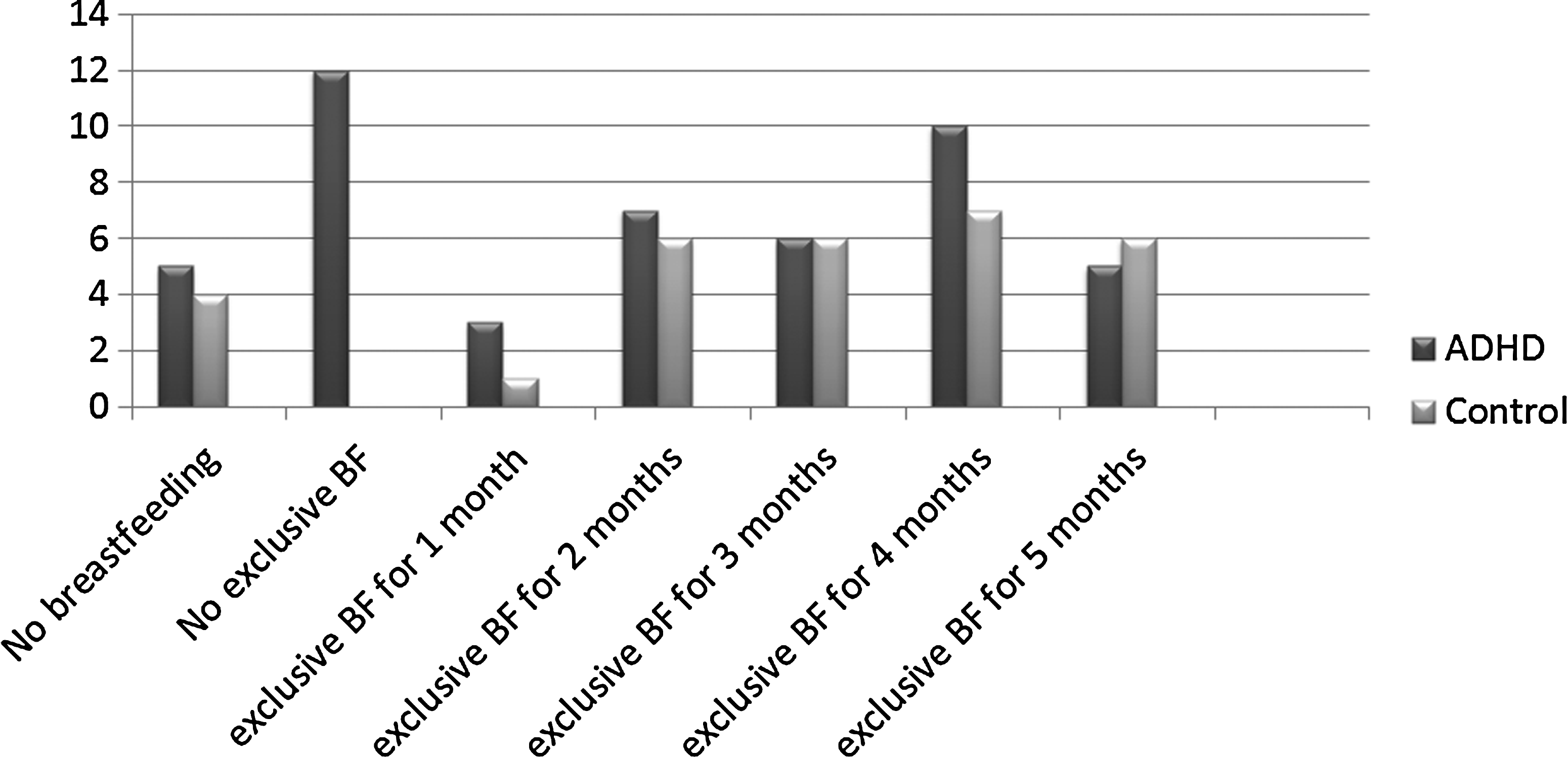
Percentages of absence of breastfeeding and exclusive breastfeeding (BF) of less than 6 months among attention-deficit/hyperactivity disorder (ADHD) and control groups.
In the ADHD group, 76 children (38%) presented with comorbid diagnoses. Children with pure ADHD were more likely to have a shorter duration of breastfeeding (p=0.03).
The mean CPRS scores of the ADHD and control groups were 44.50±21.04 and 19.25±11.42, respectively. On the CTRF, the mean scores were 33.57±13.35 and 18.86±14.23 for the ADHD and control group, respectively. The differences between two groups were significant on both scales (p=0.0001).
Two subgroups have been established from the ADHD group: one consisted of children with a history of insufficient exclusive breastfeeding (ADHD-IEB), which is less than 6 months, and the other with sufficient exclusive breastfeeding, which is 6 months or more. The ADHD-IEB subgroup consisted of 103 children (31 girls and 72 boys) who had a mean age of 10.57±2.57 years. The ADHD–sufficient exclusive breastfeeding subgroup had 97 children (19 girls and 78 boys) who had a mean age of 9.91±2.43 years. No significant difference existed between the two subgroups in regard to age, gender, and comorbidity. Also, the mean CPRS and CTRF scores were similar. Frequencies of the variables and comparison of parafunctional oral habits between these two groups are shown in Table 1. The ADHD children with absent or insufficient breastfeeding were more likely to have a history of bottle feeding, longer duration of bottle feeding, and early introduction of bottle feeding (correlations significant at the p=0.01 level). Pacifier use and nail biting were more common and longer in duration in these children (p=0.01). An important finding in the ADHD-IEB subgroup was that the duration of exclusive breastfeeding correlated negatively with the CPRS and CTRF scores (p=0.01). In both the ADHD and control groups, breastfeeding correlated negatively with bottle feeding and pacifier use (p=0.01).
ADHD, attention-deficit/hyperactivity disorder; NS, difference not significant.
Frequencies of the variables and comparison of parafunctional oral habits between the ADHD group, ADHD-IEB subgroup, and control group are given in Table 2. Several variables have been identified as significant. Duration of bottle feeding, introduction of bottle feeding, introduction of pacifier use, variables of nail and toenail biting, as well as pencil biting, bruxism, and snoring emerged as significantly different in the ADHD group in comparison with the control group. In addition to these significant findings, frequency of bottle feeding and pacifier use and duration of pacifier use were found to be higher in the ADHD-IEB subgroup relative to controls.
ADHD, attention-deficit/hyperactivity disorder; NS, difference not significant.
In the logistic regression model, duration of exclusive breastfeeding, duration of total breastfeeding, early introduction of pacifier use, and early start of finger sucking was found to be predicting ADHD diagnosis (Table 3).
Unstandardized coefficients.
SE, standard error.
Discussion
In the present study, we aimed to ascertain breastfeeding practices and, in relation to this, parafunctional oral habits in a sample of children with ADHD. To the best of our knowledge, this is the first study that explores this dimension in ADHD. In previous research, different patterns of insufficient breastfeeding have been reported,15–17 and in our study, exclusive breastfeeding has emerged as particularly insufficient, rather than the whole duration of breastfeeding. From a developmental point of view that emphasizes the importance of earlier factors, there is ground to say that exclusive breastfeeding represents a crucial period in the life of the newborn.
It is highly remarkable to find shorter duration of breastfeeding in children with pure ADHD because comorbidity is very common in ADHD. This raises the question of whether there is a subgroup of children with insufficient breastfeeding mimicking ADHD symptoms without having the genetic background suggestive of ADHD. More research is needed to support further comments.
Negative correlations between the CPRS/CTRS scores and duration of exclusive breastfeeding in the ADHD-IEB subgroup suggest a direct relationship between these factors. Our findings are in line with the earliest report by Stevens et al., 15 which noted similar correlations. Of particular interest is that similar correlations do not exist in the control group. A possible explanation of this finding may be the increased vulnerability of some children to the absence of natural feeding early in life. The subgroup question mentioned above surfaces again with this finding.
According to previous research, infants are more likely to be bottle fed as the practice of breastfeeding starts to decrease. 5 In this study, correlation results from both the ADHD and control groups confirm those reports. Thus, as exclusive breastfeeding is already insufficient in the ADHD group, elevated rates of bottle feeding (duration and earlier introduction relative to controls) may relate to this fact and emerge as a novel finding regarding infant feeding practices in ADHD. This indicates another dimension that children with ADHD may face the consequences of increased bottle feeding more commonly than normal children. Likewise, pacifier use started at an earlier age in the ADHD group than in the controls. Both frequency and mean duration of pacifier use were more pronounced in the ADHD-IEB subgroup, indicating the need to compensate the sucking urge that is unmet because of insufficient breastfeeding.
The results of logistic regression analysis further gives support to the hypothesis that ADHD is associated with both insufficient breastfeeding and consequent parafunctional oral habits.
Besides several associated disorders, a high rate of comorbidity has been reported between nail biting and ADHD. 18 In this study, previous significant findings have been confirmed, and no particular effect of breastfeeding has been noted. As a novel finding, toenail biting was explored, and it also emerged at a significantly high rate in the ADHD group. Likewise, pencil biting was more common in the ADHD group. So far as we are aware, the present report appears to be the first one that identifies a significant link between pencil biting and ADHD. Because of the associated oral habits, the ADHD children may show an increased tendency to display this habit. Cheek biting rates in ADHD children were found to be nonsignificant; however, we should keep in mind that this is a behavior less likely to be observed by the parents. We are unable to find any other previous report on this topic to further comment.
The higher prevalence of bruxism in the ADHD group is in line with previous studies.19,20 To date, no study has addressed a link between breastfeeding and bruxism. We should also keep in mind that medication-induced bruxism may exist in the ADHD group.
In this study, pica was not found to be associated with ADHD, and this also emerges as an original addition to literature.
Because there are some aspects relating to oral habits, we explored snoring and mouth breathing in the ADHD group and determined significant results for snoring. This is a confirmation of earlier results. 3
Insufficient breastfeeding, increased rates of bottlefeeding and pacifier use, and more common oral habits may affect dentofacial development. 7 Prevalence of treatment need for malocclusion indicated by a dentist in the ADHD group was not different from that of the control group. Because accurate diagnosis of malocclusion necessitates evaluation by a dentist, parent report of treatment need reflects only an aspect of malocclusion. Further research is required in this understudied area.
As can be seen in Table 1, oral habits found as significant in the ADHD group in comparison with the control group are not affected by the factor of insufficient exclusive breastfeeding. A larger sample may be required to explore the causative effects. Another point that merits attention is that, although maternal recall of breastfeeding information is an acceptable method,21,22 correlating this information with earlier health records may provide more accurate data.
In summary, the ADHD group was found to have different early feeding practices and increased rates of parafunctional oral habits. The present study sheds light on the course of the early years in ADHD, which is an under-researched period. As ADHD runs in families, strict adherence to World Health Organization recommendations on breastfeeding 4 is of crucial importance for babies born to families with a diagnosed member with ADHD. Awareness and attention to the issues associated with increased bottle feeding and pacifier use as well as parafunctional oral habits are recommended to professionals who provide child health care.
Footnotes
Disclosure Statement
No competing financial interests exist.