
Abstract
Abstract
Background:
The benefits of breastfeeding to both maternal and infant health are vast and widely known. The aim of this study was to elicit the rates of exclusive breastfeeding, early initiation of breastfeeding, and colostrum feeding and to determine the attitudes, knowledge, and influences around breastfeeding in postpartum Vietnamese women.
Materials and Methods:
A cross-sectional study was conducted at the Hung Vuong Hospital in Ho Chi Minh City, Viet Nam, between December 2010 and January 2011. Postpartum women were randomly selected and interviewed within 48 hours of delivery.
Results:
Of the 223 women interviewed, 86% had initiated breastfeeding at the time of the interview. Modes of feeding included exclusive breastfeeding (7%), mixed feeding (79%), which included breastmilk and formula or water, and exclusive formula feeding (14%). Of the breastfeeding women, 14% had initiated breastfeeding within 60 minutes of delivery, 92% had initiated within 24 hours, and 8% had initiated after 24 hours of delivery. Of women who had initiated breastfeeding, 37% had discarded their colostrum. Factors that positively influenced breastfeeding were knowledge that breastfeeding is good for the infant, advice obtained from “public information,” and the influence of health professionals and family on the decision to breastfeed. Factors that influenced the decision not to initiate breastfeeding included pain or fever after cesarean section and perceived lack of breastmilk after delivery.
Conclusions:
The rate of exclusive breastfeeding at Hung Vuong Hospital in this study was lower than the national average of 17%. Specific interventions targeting this must be formulated to increase these rates.
Introduction
O
Although exclusive breastfeeding for 6 months has been shown to confer numerous maternal and child health benefits in a systematic review, the rate of exclusive breastfeeding in many developing countries is relatively low. 4 Approximately 40% of infants under 6 months of age in Asia are exclusively breastfed, and it is estimated that only 31% are fed breastmilk within the first hour following birth. 4 Although historically Vietnam has a high rate of initiation of breastfeeding, recording prevalence rates of up to 99%,5,6 only 58% of infants are fed within the first hour of delivery. 7 Furthermore, the rate of exclusive breastfeeding declines dramatically during the first 6 months postpartum, ranging from 21.3% in the first 4 months 5 to 15.5% in the first 6 months. 8 The median duration of exclusive breastfeeding in Vietnam is approximately 0.5 months. 8 Various reasons contribute to the practice of mixed infant feeding. These include cultural, socioeconomic, and common misconceptions about mixed feeding.9–17 The widespread social marketing of formula is also a driver of mixed feeding practices.14–16
The Hung Vuong Hospital (HVH) is one of two tertiary-level maternity hospitals in Ho Chi Minh City, Viet Nam, and is a referral center for 24 district hospitals in the surrounding provinces. It has the capacity for 800 inpatient beds and 40,000 deliveries per year, with a 40% cesarean section rate. The aims of the study were to determine the prevalence of early breastfeeding in postpartum Vietnamese women and to determine their attitudes, knowledge, and influences around breastfeeding.
Materials and Methods
Sample
A cross-sectional survey of postpartum women who had been admitted to wards of the HVH was conducted between December 13, 2010 and January 13, 2011. A computer was used to generate lists of women who had delivered in the previous 48 hours. This included women who had delivered by cesarean section and women who were in either the private and public wings of the Hospital. Using a random number table generated from the Internet, women were selected for inclusion into the study. These women were then approached to participate in the study. Those who consented were then interviewed using a structured questionnaire. Participation in the study was voluntary with no remuneration offered to participants.
Women who were human immunodeficiency virus positive were excluded from the study. This was because of a national program in which human immunodeficiency virus–positive women were provided with formula as a substitute for breastmilk. Women under 18 years of age or whose infant was in the neonatal intensive care unit were also excluded.
This was an exploratory study to determine rates of exclusive breastfeeding in women delivering in this hospital. We estimated that if rates of exclusive breastfeeding were 20%, for precision of 0.05 for 95% confidence intervals, sample size should be a minimum of 246 women.
Measures
A structured questionnaire was developed specifically for this study by the primary researchers to elicit both qualitative and quantitative data about breastfeeding practices in Vietnamese women. This questionnaire comprised a mixture of open-ended and closed-ended questions and had been translated into Vietnamese prior to the commencement of the study. To ensure the validity of the questionnaire, the Vietnamese version of the questionnaire was translated back into English by an independent translator. All interviews were conducted by five midwives in Vietnamese, and the results of the interviews were then translated back into English by the same person for analysis.
Demographic data such as personal characteristics of the interviewee (age, occupation, level of education, medical illnesses), family characteristics (size and constituents of families, primary caretaker), and previous obstetric history (parity, child birth weight, duration and type of infant feeding) were elicited.
Quantitative information such as the prevalence of breastfeeding at HVH and rates of initiation of breastfeeding, infant feeding patterns, timing of initiation, and feeding of colostrum was elicited. Exclusive breastfeeding was defined by feeding of breastmilk only (as per the World Health Organization), and mixed infant feeding was defined as feeding of both breastmilk and formula milk and/or water. Early initiation of breastfeeding was defined as initiation of breastfeeding within 60 minutes of delivery. Late initiation of breastfeeding was defined as initiation of breastfeeding after Day 1 (i.e., greater than 24 hours) of delivery. Qualitative information such as the influences on breastfeeding, opinions on colostrum, and opinions on breastfeeding versus bottle feeding were also elicited.
Statistical analysis
Women were compared in two groups: those who were exclusively formula feeding versus those who had performed any breastfeeding. Univariate comparison using the chi-squared test was performed to determine factors predictive of breastfeeding. A p value of <0.05 was considered statistically significant. All statistical analysis was performed using SPSS version 17.0 for Windows software (SPSS, Inc., Chicago, IL).
Common themes were identified, and responses from women were categorized and analyzed using ATLAS.ti™ Qualitative Data Analysis Program for Windows software (ATLAS.ti Scientific Software Development GmbH, Berlin, Germany).
Ethics approval
Approval from the HVH and the University of Sydney Ethics Committees was gained prior to commencement of the study (HREC number 13295).
Results
Sample size
Approximately 1,600 women delivered during the study period. In total, 252 women were randomly selected to participate in the study. Fourteen women had been discharged by the time of approach, 11 women were excluded from the study because of infant death or infant in the neonatal intensive care unit, and four refused consent. A final number of 223 women was included in the study, representing approximately 14% of all births and 89% of the random sample.
Demographics
Demographic and delivery characteristics for women in the study are shown in Table 1.
Primary school is from years 1 to 5. Secondary school is from years 6 to 9. High school is from years 10 to 12.
The age of women ranged from 18 to 43 years. Of 223 women interviewed, 117 women had a vaginal delivery (53%), 90 women delivered by cesarean section (40%), 11 women had a vacuum delivery (5%), and 5 women delivered by forceps (2%). Of the 223 women, 93 had delivered in the public wing (42%), and 130 women had delivered in the private wing (58%).
Prevalence of breastfeeding
Of the 223 women interviewed, 191 (86%) were breastfeeding at the time of interview. Of the women who were breastfeeding, only 7% were breastfeeding exclusively, with 79% feeding their infants a mix of breastmilk, formula, and/or water, and 14% exclusively formula feeding.
Demographic characteristics of mothers who performed any breastfeeding compared with those who artificially fed from birth were not statistically different, with the exceptions of mode of delivery and history of maternal medical disease (Table 2).
Primary school is from years 1 to 5. Secondary school is from years 6 to 9. High school is from years 10 to 12.
There was no difference in rates of breastfeeding between women who were privately or publicly insured. Women undergoing cesarean section were more likely to artificially feed (77% compared with 34%; unadjusted odds ratio=6.5; 95% confidence interval, 2.6, 15.9). The cesarean section rate in women privately insured was 44% compared with 33% in women publicly insured. Women who experienced medical illness in their pregnancy were also more likely to artificially feed (16% compared with 4%, unadjusted odds ratio=4.4; 95% confidence interval, 1.3, 14.5). None of the women who had delivered by cesarean section had performed exclusive breastfeeding.
In the women who were breastfeeding (including those who were exclusively and mixed feeding), factors that positively influenced their decision to breastfeed are outlined in Tables 3 and 4. Major influencing factors included the knowledge that breastfeeding is good for the infant (specifically, that it provides the infant with immunity), advice obtained from “public information,” which includes TV, newspapers, magazines and books, and the Internet, and the influence of health professionals and family (particularly the woman's mother).
Mothers could give more than one response.
HVH, Hung Vuong Hospital.
Mothers could give more than one response.
C-section, cesarean section; HBV, hepatitis B virus; IVF, intravenous fluid.
Of the 223 women interviewed, 31 (14%) stated they were not breastfeeding. The major factors that influenced their decision not to breastfeed are outlined in Table 5 and include pain after cesarean section, perceived lack of breastmilk after delivery, hepatitis B infection and risk of transmission of virus in breastmilk, and physical inability to move an arm due to intravenous fluid infusion.
Timing of initiation of breastfeeding
Of the women interviewed who were breastfeeding, 14% had initiated breastfeeding within 60 minutes of delivery, 92% of women had initiated breastfeeding within 24 hours, and 8% had initiated greater than 24 hours of delivery (Fig. 1). All the women with breastfeeding initiated after 24 hours had delivered by cesarean section.
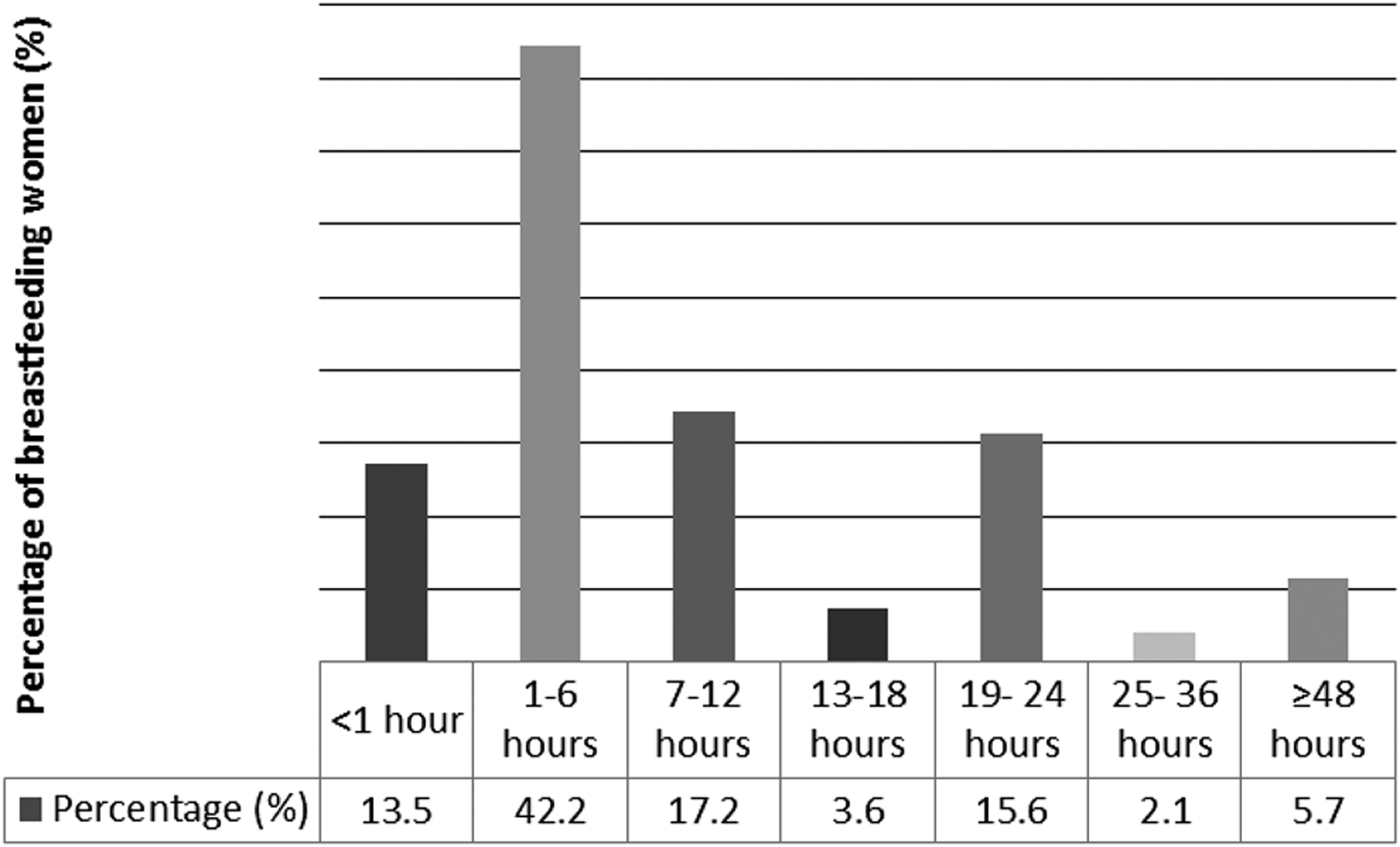
Time to initiation of breastfeeding (n=191).
Reasons for late initiation of breastfeeding included postoperative pain and inadequate or no breastmilk, postoperative fatigue, and attachment to an intravenous fluid or antibiotic drip.
Colostrum
Of 191 women, 140 women (73%) who were breastfeeding had fed their infants colostrum, 70 women had discarded their colostrum (37%), and 13 women (7%) were unsure if they had fed their infants colostrum.
Discussion
This study found that 86% of women who were interviewed had initiated breastfeeding, yet the rate of exclusive breastfeeding was 7%. Seventy-three percent of women who were breastfeeding had fed their babies colostrum. Fourteen percent of breastfeeding women had initiated breastfeeding within 60 minutes of delivery. All the women who initiated breastfeeding late (>24 hours) had delivered by cesarean section.
The strengths of this study are the prospective collection of cases and the random selection of women to attain a picture of the current breastfeeding practices and the barriers towards exclusive breastfeeding in this hospital. It is the most recent study in Ho Chi Minh City to attempt to determine the factors influencing a woman's decision on how to feed her infant and highlights the adverse effect of high cesarean section rates in preventing breastfeeding within the first hour of life. The weakness of this study is that it was limited to a hospital-based population. However, as rates of institutional delivery are very high (79%) in urban Vietnam (according to the 2002 Demographic Health Survey) 18 and by including both publicly and privately insured women, we feel that we have attained a representative sample of women.
Despite global initiatives to push for better breastfeeding rates worldwide, the prevalence of breastfeeding and, in particular, exclusive breastfeeding is still suboptimal in many developing countries. 4 Furthermore, there is evidence of a downward trend of exclusive breastfeeding in developed countries in the past 10 years. 4 Ho Chi Minh City is one of the fastest growing cities in Viet Nam. As the country becomes more affluent, it is postulated that breastfeeding rates will drop as formula and breastmilk substitutes become more affordable. 12 Therefore, strategies must be put into place now to mitigate this negative trend, and the benefits of doing so are many.
Although HVH is accredited as part of the Baby Friendly Hospital Initiative, the late initiation of breastfeeding, the wide use of formula feedings early in lactation, and the failure to use colostrum are contrary to the 10 Steps to Successful Breastfeeding. Recent research has established that later initiation of breastfeeding (2, 3, or more than 4 hours postpartum) is associated with a stepwise increase of feeding morbidity compared with initiation within the first hour after birth. 19 Initiating breastfeeding within the first hour of birth confers multiple benefits for both the mother and baby20,21 and has been shown to reduce infant mortality. A large study based in Ghana in 2003 revealed a 2.4 times increase in neonatal mortality rate if breastfeeding was delayed by 24 hours and estimated that 22% and 16% of neonatal deaths could be prevented if all infants were breastfed within the first hour and from Day 1, respectively. 22 This was echoed by a Nepalese study conducted between 2002 and 2006, which revealed a higher mortality rate in neonates who were breastfed after 24 hours (relative risk=1.41) and that approximately 19.1% and 7.7% of all neonatal deaths may be avoided with universal initiation of breastfeeding within the first hour and day of life, respectively. 23
The risk of introducing mixed feeding and prelacteal feeds as seen in HVH is that this will shorten the duration of lactation,24–26 with long-term implications. A national nutrition survey in Viet Nam revealed that approximately 23–35% of children are stunted.27,28 Reducing the rate of stunting can be achieved with exclusive breastfeeding and appropriate complementary feeding in the first 2 years of life. Conversely, obesity among young people in Ho Chi Minh City is now documented. 29 There is strong evidence that breastfeeding reduces the risk of overweight/obesity in children and adolescents by 20–50%.24–26,29 Moreover, in a dose–response relationship, more prolonged exclusive breastfeeding is associated with greater protection against childhood overweight. 7 Breastfeeding confers protection against overnutrition during early childhood by lowering the risk of developing obesity and thus hypertension, cardiovascular disease, and diabetes later in life. 7
Prominent barriers to breastfeeding in this study were perceived inadequate supply of breastmilk, promotion of breastmilk substitutes such as formula, and inadequate analgesia post–cesarean section. These barriers should be addressed, at both hospital and governmental levels. There is evidence to link maternal perceived insufficient milk supply to early cessation of lactation,30–33 with approximately 25–35% of lactating women reducing breastfeeding duration or level because of perceived breastmilk insufficiency.31–33 This perception may be perpetuated by a lack of education into the physiology of breastmilk supply and lactation (supply=demand). Increase in education beginning in the antenatal period and continuing throughout pregnancy, with further lactation support and reinforcement of breastfeeding in the postpartum period, may help change perception of inadequate supply of breastmilk.34–36 Mothers can be reassured that their infants are receiving adequate nutrition from breastmilk alone by regular monitoring (urine output) and tracking of growth of infants.
The cesarean section rate in tertiary units in Ho Chi Minh City is high and requires critical review. Women who have had cesarean sections in particular should be targeted to improve exclusive breastfeeding rates and promote early initiation of breastfeeding. At present, women who have delivered via cesarean section are monitored in the intensive care unit for an average of 6 hours postpartum. Their babies are usually handed over to the woman's relatives to be looked after during this time. Babies are fed with formula during this time and begun on breastmilk when reunited with their mothers. Lactation midwives need to be in the recovery ward ensuring mothers and babies are kept together during this important postpartum period, assisting with correct early attachment and positioning and suckling. In this study, pain is an important barrier to early initiation of breastfeeding, and adequate opioid analgesia should be provided to women who have undergone a cesarean section. This includes review of operative anesthesia and analgesia that maximizes beneficial outcomes for mother and baby.
Breastmilk, including colostrum, must be promoted as the best way of feeding babies and infants. Stricter laws and policies based around the International Code of Marketing of Breast milk Substitutes should be formulated and enforced more vigorously, and harsh penalties must be upheld if these policies are violated. Change should start at a governmental level and permeate through all levels of the health system. Messages that breast is best must not be ambiguous. There are currently strict policies on the blatant endorsement of formula companies at HVH, yet formula is readily available from the hospital canteen. This sends mixed messages to women. The process of legislative change has already begun in Viet Nam. A law on advertisement banning the promotion of breastmilk substitutes for children up to 2 years of age was passed by the National Assembly on June 21, 2012. 37 Paid maternity leave was also extended from 4 to 6 months. 37 Although this is a good first step, the changes in marketing of formula milk and maternity leave will only be beneficial if early initiation of exclusive breastfeeding is encouraged, supported, and established in hospitals from the time of birth, as highlighted in this study. Factors such as indication for and adequate analgesia after cesarean section also need to be addressed at a hospital level. At a community level, enforcement of this new legislation and education of mothers on the benefits and importance of breastfeeding by trained health workers is of utmost importance. 37
Conclusions
The rate of exclusive breastfeeding at HVH in this study was 7%, lower than the national average of 17%, with early initiation rates of 86%. Change in exclusive breastfeeding rates and rates of early initiation of breastfeeding is possible in Vietnam, and it is hoped that the recent multilevel commitments and targeted interventions will ensure that the benefits of exclusive breastfeeding can be shared by all.
Footnotes
Acknowledgments
We thank the Australia Vietnam Hoc Mai Medical Foundation, the University of Sydney, the Director of Hung Vuong Hospital, Dr. Nguyen Van Truong, Dr. Thach Son Tran, and Dr. Dang Le Dung Hanh, who facilitated this study, and the mothers who so willingly gave their time for interview. The study was supported by an international public health scholarship for S.R. from the Hoc Mai Australia Vietnam Medical Foundation of the University of Sydney.
Disclosure Statement
No competing financial interests exist.