
Abstract
Abstract
Aim:
This study investigated if a process-oriented training for health professionals will influence women's use and reasons for using a nipple shield, the baby's weight, and the duration of breastfeeding.
Materials and Methods:
An intervention was performed for health professionals that included a process-oriented training program on breastfeeding support. Primiparas living in either the intervention municipality or in a control municipality were asked to participate in a longitudinal study to evaluate the care given. Data collection for control group A (CGA) (n=162) started before the intervention was initiated. Data for control group B (CGB) (n=172) were collected simultaneously with those for the intervention group (IG) (n=206). The mothers responded to questionnaires at 3 days, at 3 months, and at 9 months postpartum.
Results:
The mothers' use of nipple shields related to the finding that if the women had a higher body mass index in the beginning of the pregnancy, the babies had difficulty in grasping over the nipple, and the mothers had pain or wound on the nipple. For the mothers in the IG group, there was no significant difference if they had used nipple shields or not in relation to breastfeeding duration. In contrast, the mothers in the control groups had a significant shorter breastfeeding duration if they had used nipple shields. In the IG, there were no significant difference between the use of nipple shields and the babies' weights at 3 or 9 months. The babies of women in the CGB who used nipple shields had a significantly lower weight at 3 months than the babies of those who did not use nipple shields (p=0.02).
Conclusions:
A process-oriented training in breastfeeding counseling prolongs the duration of breastfeeding for women with breastfeeding problems, where the problems are remedied by the use of nipple shields.
Introduction
I
Obesity in women and large breasts have both been shown to be associated with more breastfeeding problems. 5 One study shows that overweight or obese women with a body mass index (BMI) of ≥26 kg/m2 before pregnancy have decreased prolactin (the milk-secreting hormone) levels from 48 hours to 7 days after delivery, compared with normal-weight women. 6 Baker et al. 7 reported that women with a higher BMI before pregnancy stop breastfeeding earlier than normal-weight women. Women's obesity is associated with shorter breastfeeding duration, and many overweight women also have large breasts. 5 The difficulty increases with obesity and will be most extreme if the woman is both overweight and has large breasts. Both obesity and large breasts, often with flat nipples, make it harder to create a good position for the baby when breastfeeding.4,5 The most common cause of breastfeeding problems is that the baby does not get a good grasp of the nipple. 8 According to Bodley and Powers, 4 nipple shields help 88% of women with this kind of problem to succeed with breastfeeding.
The most common reasons for the use of nipple shields are as follows: inverted, short or flat nipples, such that the child has difficulty getting a grasp of the nipple; disorganized sucking; sore nipples; swollen breasts; premature babies; and the baby having tongue-tie.4,9 Sealy 10 reported that breastfeeding problems can cause pain and suffering for the woman, which often results in the baby crying and possible difficulties in getting into a good breastfeeding position.
Women with these breastfeeding problems are often advised to use a nipple shield to protect the nipple. When a woman starts to use a nipple shield, the baby often increases in weight and then follows the normal weight curve. Brigham 8 showed that it is most common to start using a nipple shield between Day 1 and Day 42 after birth; of the women in this study, 86% believed that nipple shields had helped them to continue breastfeeding when breastfeeding difficulties arose. None of the women in this study reported an insufficient milk supply, inadequate weight gain, or that breastfeeding reduced lactation. Of the women who were helped by using the nipple shields, 37% stopped using it after a while. Pincombe et al. 11 showed that when women already started using nipple shields in the maternity ward, there was a 2.1 times greater risk that they would stop breastfeeding earlier than those women who were able to breastfeed their babies without nipple shields. The most common comment from many health professionals is that women who use nipple shields find it helpful and that it is pleasant and comfortable. However, in a contrasting study by Eglash et al., 12 the professionals frequently thought that nipple shields were not helpful and often caused problems. The women in this study using nipple shields were often poorly followed up, and furthermore they found the shields troublesome and uncomfortable. Maybe health professionals are not recommending nipple shields because of limited research in this area.3,4
Women all too often experience that health professionals give contradictory advice about breastfeeding. 13 When breastfeeding problems occur, the woman wants a midwife to understand her own unique needs; otherwise, she may feel uncertain about the situation. Women want more time, understanding, and more follow-up from the health professionals. 14 Ekström et al.13,15 showed that health professionals' attitudes can be improved through training in how to provide breastfeeding support. Furthermore, professional support can positively influence the woman's relationship with her child and her feelings about herself as a mother. 16
Midwives who have a supportive and listening attitude strengthen the woman's confidence and thereby facilitate breastfeeding. 17 Support is central to the relationship between the midwife and the woman around the time of childbirth. 18 In the case of difficulties with breastfeeding, the role of the midwife and the partner is to support the woman so that she feels capable, regardless of whether the child is breastfed or not. 19 The aim of this study is therefore to investigate if a process-oriented training for health professionals will influence women's use and reasons for using nipple shields, the baby's weight, and the duration of breastfeeding.
Materials and Methods
Hypothesis
The following hypothesis was tested: through process-oriented training for midwives and child health nurses, a changed attitude toward providing more facilitative support will positively influence women's use of the nipple shield, the baby's weight, and the duration of breastfeeding.
Study design
This is a longitudinal intervention study in which groups of women receive care around the time of childbirth from midwives and child health nurses, some of whom have gone through a process-oriented training program to provide support during childbirth and breastfeeding. The control group receives support from midwives and child health nurses who have not gone through the process-oriented training program, and this is considered to be a standard care group.
Setting
The study was performed in a county in the southwest of Sweden. The county consists of 13 municipalities with antenatal and child health centers and comprises urban, suburban, and rural districts, with 280,000 inhabitants. Approximately 2,500 births occur annually at the county maternity clinic. The woman and her partner will meet a midwife approximately eight to 11 times during her pregnancy. Almost all women give birth in a hospital, and care in the hospital is provided by midwives who are not previously known to the woman. The length of hospital stay is between 6 hours and 4 days, and a child health nurse makes a home visit 7–10 days after the birth and remains in contact until the baby is old enough to start school at 6 years of age.
At the time of the study, the National Board of Health and Welfare defined breastfeeding as follows: exclusive breastfeeding was defined as breastfeeding with occasional use of water, breastmilk substitutes (not more than a few times), and/or solids (not more than 1 tablespoon per day). Partial breastfeeding was defined as infants who received breastmilk and breastmilk substitutes (every day) and/or solids (more than 1 tablespoon per day). Total breastfeeding was defined as the duration of both exclusive and partial breastfeeding. 19
Intervention
Phase 1: randomization and the process-oriented training program for the midwives and postnatal nurses in parental support and breastfeeding
Based on the findings of a baseline study,20,21 the 10 largest municipalities in the selected area were grouped into pairs according to their size and the duration of breastfeeding in those municipalities. The paired municipalities were randomly designated to intervention (five municipalities) or control (five municipalities) by a person not involved in the study. The randomization was done before any data collection began. Furthermore, antenatal midwives and postnatal nurses were allocated to either intervention or control, depending on whether their work site had been randomly selected as an intervention municipality or as a control municipality. A process-oriented training program 20 in professional support in childbearing was conducted for the midwives and postnatal nurses from the intervention municipalities from September 1999 through to March 2000. The teaching program was composed of evidence-based lectures with collegial discussions on professional stance, reflective processes, problem-solving processes, and practical skills in relation to the provision of support during childbirth and breastfeeding, in line with the World Health Organization's recommendations about breastfeeding support 21 (see Appendix). This process-oriented training program resulted in more facilitating and less regulating attitudes among participating antenatal midwives and postnatal nurses. 15
Phase 2: the sample of women and the data collection procedures
The women included in this study had been cared for during their pregnancies either by health professionals in one of the five intervention municipalities or by health professionals in one of the five control municipalities. None of the women knew whether their antenatal midwife and child health nurse had been through the process-oriented training program (intervention group [IG]) or not (control group). During their stay in the delivery and maternity ward at the hospital, all the women met midwives who had not participated in the process-oriented training program on giving support during childbirth and breastfeeding.
Inclusion criteria
Swedish-speaking, healthy, first-time mothers who gave birth to single, healthy, full-term babies delivered spontaneously, by vacuum extraction, or by cesarean section were eligible. The women had been cared for either by health professionals in the intervention municipality, as described previously, or by health professionals in the control municipalities.
Exclusion criteria
First-time mothers who had given birth to babies with life-threatening diseases or malformations, for example, very severe asphyxia, were excluded.
Participation
All women who fulfilled the inclusion criteria and had been cared for at the antenatal and child health clinics in the municipalities selected for this study were consecutively identified from the hospital register and asked to participate in the study (n=584). Of those, 480 gave their informed consent to participate in the study, which translates to a response rate of 82% (Fig. 1).
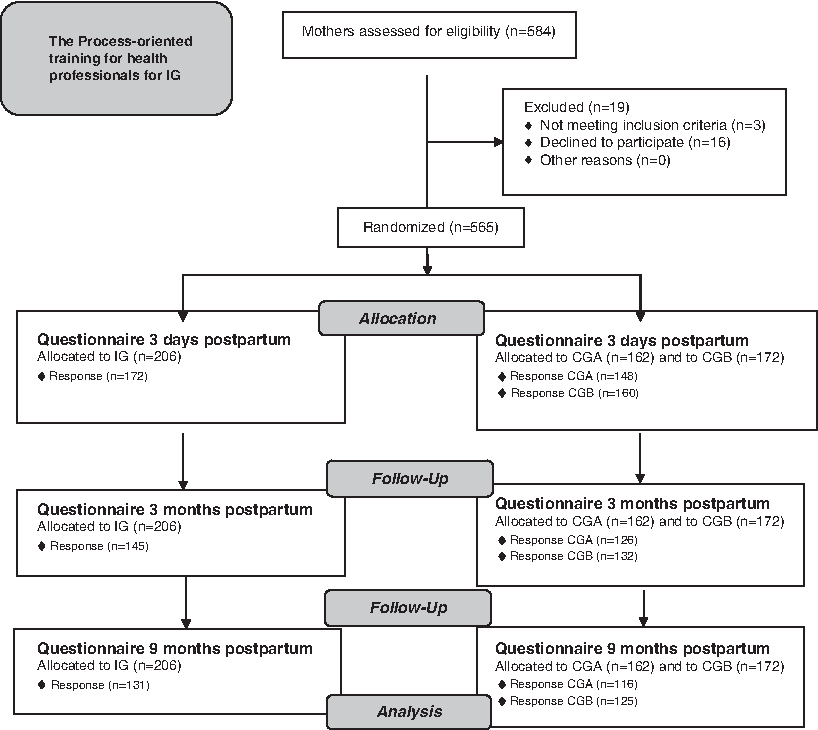
Flow diagram, CGA, control group A; CGB, control group B; IG, intervention group.
Questionnaires
Three questionnaires were developed for this longitudinal study. Demographic background data and BMI (before pregnancy) were collected in the first visit at the antenatal care. Obstetric data were collected from birth records. Demographic background data were also collected when the first questionnaire was administered. Maternity staff members distributed the first questionnaire to the women, who were asked to answer this questionnaire 3 days after birth. Follow-up questionnaires were posted to the women 3 months and 9 months after birth (Fig. 1). Questions about breastfeeding duration were taken from the questionnaires or by a telephone call, if the breastfeeding rate was longer than 9 months.
The questionnaires were distributed to the women at 3 days, 3 months, and 9 months after the birth. Questions about breastfeeding included the following: “Have you used a nipple shield for breastfeeding?” (no, yes but not anymore, yes still); “If you use a nipple shield, for what reason do you?” (open question); “How long have you breastfed, exclusively, and in total?”; “If you use nipple shields, at whose initiative was it?” (open question); “If you use a nipple shield, has it had the desired effect?” (yes, no, do not know, partially); and “What is the baby's weight at 3 days, 3 months, 9 months?” One reminder was sent at each time point to women who did not respond to the questionnaire.
The three questionnaires developed for this study were pilot-tested on 20 women for acceptability and face validity. In addition, an expert group of midwives and child health nurses was consulted to establish the content validity of the questionnaires. A few minor corrections to the wording were made before the data collection began.
Sample size
The sample size was based on results from the mapping baseline study20,21 to detect a difference between the IG group and the controls of 1 month in duration of exclusive breastfeeding with β=0.8 and α=0.05. Before the process-oriented training program commenced, data were collected for a baseline group called control group A (CGA) (n=148). Data from CGA were collected before any effects of the intervention could be measured. Data for control group B (CGB) (n=160) and IG (n=172) were collected simultaneously. This design allowed detection of changes over time and any spill-over effects of the intervention. The same five municipalities provided the sample population for CGA and CGB.
Statistics
For the statistical analyses of the data, we used Statistical Package for the Social Sciences software (SPSS version 19.0; SPSS, Inc., Chicago, IL). Central measurements were presented as a mean, and dispersion was shown by standard deviation (SD). To test for the differences between groups, one-way analyses of variance (ANOVAs) and Tukey's highly significant difference (HSD) test for post hoc comparisons were performed. Chi-squared tests were performed on category data. Values of p≤0.05 were considered significant. 22
Ethical considerations
The study was approved by the Ethics Committee of the Medical Faculty of Gothenburg University, Gothenburg, Sweden.
Results
Response rates and demographic and obstetric data
Response rates for the three questionnaires were quite high, even at 9 months after birth, and are presented in Table 1. The demographic and obstetric data for the participants and the external dropouts did not differ significantly among the groups (data not shown). With regard to demographic and obstetric data, no significant differences existed between the women in the IG compared with the women in the CGA or CGB (Table 2). There were no significant differences regarding background data or breastfeeding duration between the mothers who had answered just the first questionnaire compared with those who had answered all three questionnaires.
Data are number of women (%).
CGA, control group A; CGB, control group B; IG, intervention group.
1 kg=2.2 pounds.
Data are mean (standard deviation) values.
Data are number (%).
CGA, control group A; CGB, control group B; IG, intervention group; NS, not significant.
Duration of breastfeeding
Data were analyzed for the duration of exclusive breastfeeding for IG (mean 3.9 months, SD 2.2 months), for CGA (mean 3.2, SD 1.7 months), and for CGB (mean 3.5, SD 2.0 months). There was a significant difference between IG and CGA (p=0.02). Data were also analyzed for the duration of total breastfeeding for IG (mean 7.5, SD 4.7 months), for CGA (mean 7.1, SD 4.6 months), and for CGB (mean 7.0, SD 4.5 months). At 9 months, 23% of all the mothers had stopped breastfeeding (IG, 29%; CGA, 22%; and CGB, 17%). There was no significant difference among the groups with regard to the duration of total breastfeeding.
Number of women using nipple shields
Overall, the number of women using nipple shields at 3 days was 81 (18%), at 3 months it was 40 (10%), and at 9 months only two women (1%) were still using nipple shields. There was no significant difference (by chi-squared tests) among the three groups regarding the use of nipple shields (Table 3).
Data are number (%).
CGA, control group A; CGB, control group B; IG, intervention group.
Reasons for using nipple shields
The most common reasons for the use of nipple shields (in the first questionnaire) at 3 days after birth were that the baby had difficulty in grasping the nipple (62%), wounds of the nipple (29%), and pain (7%). At 3 months (in the second questionnaire), the most common reasons were wounds of the nipple (50%), that the baby had difficulty in grasping the nipple (36%), and pain on the nipple (10%). At 9 months (in the third questionnaire), the most common reasons were wounds of the nipple (56%), that the baby had difficulty in grasping the nipple (24%), and pain on the nipple (16%). There were no significant differences (by chi-squared tests) among the groups regarding the reasons for the use of nipple shields at any time.
Relationship between the use of nipple shields and breastfeeding duration
For the women in the IG, there was no significant difference (by one-way ANOVAs and Tukey's HSD test) between those who used a nipple shields, whether at 3 days, 3 months, or before the baby was 9 months, and those who never used a nipple shield, in relation to the exclusive or total breastfeeding duration (Table 4).
Data are mean and standard deviation (SD) months.
CGA, control group A; CGB, control group B; IG, interventional group.
In the CGB, those women who did not use a nipple shield at 3 months had a significantly longer total breastfeeding duration than those who did use nipple shields (p=0.05). Women who by 9 months had not used nipple shields had a significantly longer total breastfeeding duration than those who had used nipple shields earlier (p=0.05). However, there were no other significant differences (one-way ANOVAs and Tukey's HSD test) between women who used nipple shields and those who did not.
In the CGA, those women who did not use nipple shields at 3 days had a significantly longer exclusive breastfeeding duration than those who used nipple shields at 3 days (p=0.01). The women who had not used nipple shields at 3 months had a significantly longer exclusive breastfeeding duration than those who by 3 months had used nipple shields earlier, but not anymore or who still used nipple shields (p<0.001). Those women who had not used shields had also a significantly longer total breastfeeding duration than those who used nipple shields (p=0.004). Women who used nipple shields earlier than 3 months, but not anymore, also had a significantly shorter total breastfeeding duration than those who did not use nipple shields (p<0.02). However, there were no other significant differences (by one-way ANOVAs and Tukey's HSD test) between the women who used nipple shields and those who did not.
Initiative for the use of nipple shields
For women in all the groups, there was no significant difference regarding on whose initiative women used nipple shields at 3 days (IG, 13%; CGA, 21%; and CGB, 16%). In all groups, the initiative came from the midwife in the first place, and subsequently it came from the woman herself (by chi-squared tests).
Mothers' experiences of whether the nipple shields had the desired effect
There were no significant differences (by chi-squared tests) among the groups concerning whether the nipple shields had the desired effect on breastfeeding problems. At 3 days after birth, in total, 85% of women using them said that they had a good effect, 11% said they had not had a good effect, and 4% said they did not know. At 3 months after birth, in total, 61% said they had had a good effect, 34% said they had not had a good effect, 5.0% said they did not know, and 1% said that using a nipple shield had had a partial effect. At 9 months, in total, 77% said they had had a good effect, 19% said they had no good effect, and 4% said they did not know.
Relationship between the women's BMI and the use of nipple shields
Women who used nipple shields during breastfeeding when the baby was 3 days old had a significantly higher BMI at enrollment into antenatal care, compared with women not using nipple shields: 25.6 (SD 6.1) kg/m2 (n=54) versus 23.4 (SD 4.3) kg/m2 (n=199) (p=0.01, by one-way ANOVAs and Tukey's HSD test).
Use of nipple shields and its relationship to babies' weight
For the IG women, there were no significant correlations if nipple shields had been used or not and the babies' weights at 3 or 9 months. In contrast, the CGB women's babies who had used nipple shields had a significantly lower weight at 3 months (n=17; mean 5.9 kg, SD 0.8 kg) than the babies of those who did not use nipple shields (n=109; mean 6.4 kg, SD 0.9 kg; p=0.02). At 9 months there were no longer any significant differences. Among the CGA women, there was no significant difference in the weight of the babies if the women used the nipple shield or not, at either 3 or 9 months (Fig. 2) (by one-way ANOVAs and Tukey's HSD test).
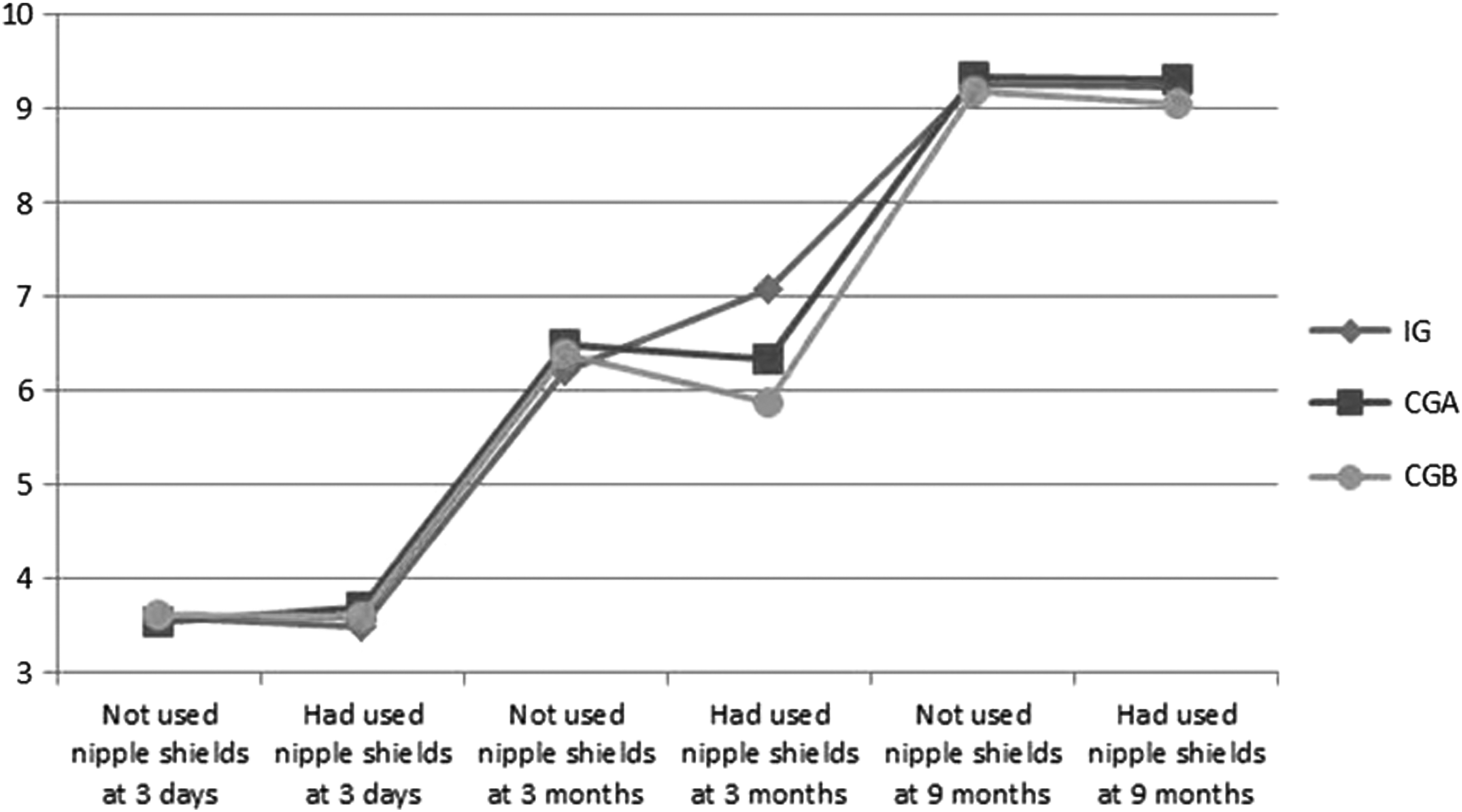
Growth trajectories for babies for whom nipple shields were not used or used during breastfeeding, at 3 days, 3 months, and 9 months after birth, in the intervention group (IG), control group A (CGA), and control group B (CGB).
Discussion
This study showed that a process-oriented training in breastfeeding counseling prolongs the duration of breastfeeding for women with breastfeeding problems where the problems may be remedied with the use of nipple shields. For the mothers in the IG group there was no significant difference if they had used nipple shields or not in relation to breastfeeding duration. In contrast, the mothers in the control groups had a significant shorter breastfeeding duration if they had used nipple shields. The mothers' use of nipple shields related to if the women had a higher BMI in the beginning of the pregnancy, if the babies had difficulty to grasp over the nipple, and if the mothers had pain or wound on the nipple. There was no significant difference among the IG, CGA, and CGB regarding their reasons for using nipple shields.
Furthermore, women who used nipple shields during breastfeeding had had a significantly higher BMI at enrollment into antenatal care, compared with women who did not later use nipple shields. Previously it has been reported that both obesity and large breasts make it more difficult to create a good position for a baby when breastfeeding. 5 Baker et al. 7 showed that women with a higher BMI before pregnancy end their breastfeeding duration earlier than women of a normal weight.
The most common reasons for using nipple shields, at 3 days, 3 months, and 9 months postpartum, was that the babies did not get a good grasp of the nipple and that the women had sore nipples. These results are in line with those of another study that found that the most common reason for women using nipple shields was having flat nipples, which means that the babies do not get a good grasp of the nipple. 4 Several other studies have shown that women have positive experiences in relation to the use of a nipple shield and that they receive help from it.4,8,23,24
Ekström et al. 13 reported that health professionals receiving process-oriented training in support during childbirth and breastfeeding changed their attitudes in a positive manner. In addition, the women in the study felt that they were offered better professional support by these trained professionals. 16 These results may be due to the professionals having greater competence in giving breastfeeding support to individual women. This is supported by another study that shows that it is a midwife's empathy that strengthens a woman's self-confidence and leads to her being less sensitive about receiving contradictory advice. 25 A study by Backström et al. 14 showed that when breastfeeding difficulties arise, the woman wants the midwife to understand her unique needs; otherwise, she may feel uncertain about the situation. Women want more time, greater understanding, and more follow-up from the professionals.
The results of the present study showed that there was no significant difference between the IG and CGA concerning the child's weight in relation to using nipple shields (or not) during breastfeeding. However, the CGB children whose mothers used nipple shields had a significantly lower weight at 3 months. Another study demonstrated that it may be useful to monitor the baby's weight more carefully when the infant is breastfed through nipple shields. 26 When previous studies examined milk transfer to the infant through nipple shields, the nipple shield was made of an older model of latex, which was thicker and less pliable than the thin silicone teat that is now available, and this may have resulted in a decrease in milk transmission. 27
The results indicate that women, already during early pregnancy, need to make informed choices about breastfeeding and how it can be facilitated, and this may lead women to feel stronger in themselves. In consequence, women are better prepared to make their own decisions in order to prevent and to solve their breastfeeding problems. Probably it is not the nipple shields themselves that affect breastfeeding, but rather the combination of nipple shields with professional support that gives the most successful outcome for the duration of breastfeeding.
Conclusions
Support from health professionals is important for women during breastfeeding. The results from this study show that if women use nipple shields when breastfeeding problems arise, it does not affect the duration of breastfeeding negatively. A process-oriented training in breastfeeding counseling prolongs the duration of breastfeeding for women with breastfeeding problems where the problems may be remedied with the use of nipple shields.
Footnotes
Acknowledgments
This study was supported by the Skaraborg Institute for Research and Development, School of Life Sciences of the University of Skövde, Sweden, and by the Primary Care Unit in Skaraborg and the Science Committee, Central Hospital, Skövde, Sweden.
Disclosure Statement
No competing financial interests exist.
All authors were active in the design, data collection, analysis, and writing up of the study. All authors also read and approved the final manuscript.