
Abstract
Abstract
Objective:
This study determined the impact of breastfeeding on hypoestrogenic symptoms among women in the postpartum period and correlated these findings with the Estrogen Threshold Hypothesis, which postulates that the hypoestrogenic symptoms experienced are related to circulating estrogen levels.
Study Design:
Using a survey instrument that combined previously validated assessments of postpartum mood changes and menopausal symptoms, women were evaluated in the immediate postpartum period, prior to hospital discharge, and at 3 and 6 weeks postpartum. Each time period was analyzed independently, in a cross-sectional design, where women were categorized as “breastfeeding” or “bottle feeding.”
Results:
Of 236 women recruited, 171 (72.5%) intended to breastfeed, and 62 (26.3%) intended to bottle feed. At both the 3- and 6-week postpartum evaluations, a similar percentage of women in the breastfeeding and bottle-feeding groups reported hot flashes. However, breastfeeding women were more likely to report vaginal dryness than those who did not breastfeed: 20/150 (13.3%) versus 3/80 (3.8%) at 3 weeks, p<0.05; 25/143 (17.5%) versus 2/87 (2.3%) at 6 weeks, p<0.001.
Conclusions:
The Estrogen Threshold Hypothesis accurately predicts the findings of increased reported vaginal dryness but not hot flashes during lactation.
Introduction
I
Application of the Estrogen Threshold Hypothesis thus far has been with regard to situations in which hypoestrogenemia is therapeutically induced for the treatment of estrogen-dependent disease such as endometriosis. However, the most common situation during which a woman of reproductive age undergoes hypoestrogenemia is during lactation.
Maternal estradiol levels in pregnancy reach approximately 40 ng/mL at term. 2 Lactating women are known to be relatively hypoestrogenic. Multiple studies indicate that circulating estradiol concentrations are suppressed in postpartum lactating women.2–4 The hypoestrogenic state is first induced by delivery and subsequently continues secondary to lactation. Several studies have shown that in breastfeeding women, estradiol levels stay in the 30–40 pg/mL range, whereas they rise to normal levels more rapidly in women who are not breastfeeding.2,5 In the population of postpartum women who breastfeed, the elevated prolactin levels suppress pulsatile secretion of gonadotropin-releasing hormone, thereby maintaining a degree of gonadal suppression. The exact mechanism by which gonadotropin-releasing hormone secretion is suppressed is not known, but it is thought to result from a central inhibition by prolactin. 5 Other data suggest that prolactin may have a direct inhibitory action on the ovary.6,7
In 1997, the American Academy of Pediatrics increased their recommended duration of breastfeeding from 6 months to 1 year. 8 Although there are obvious nutritional benefits for the infant, the extent to which mothers are affected is unknown.
The purpose of this study was to elucidate the type, incidence, and severity of hypoestrogenic symptoms, including mood changes, experienced by the lactating and nonlactating population and to determine whether the hypoestrogenic symptoms could be predicted based on the Estrogen Threshold Hypothesis. Based on the Estrogen Threshold Hypothesis and previously demonstrated estradiol levels of around 30–40 pg/mL during lactation, our study hypothesis was that breastfeeding women are likely to experience vaginal dryness as the predominant hypoestrogenic symptom rather than hot flashes when compared with women who bottle feed in the postpartum period (Fig. 1).
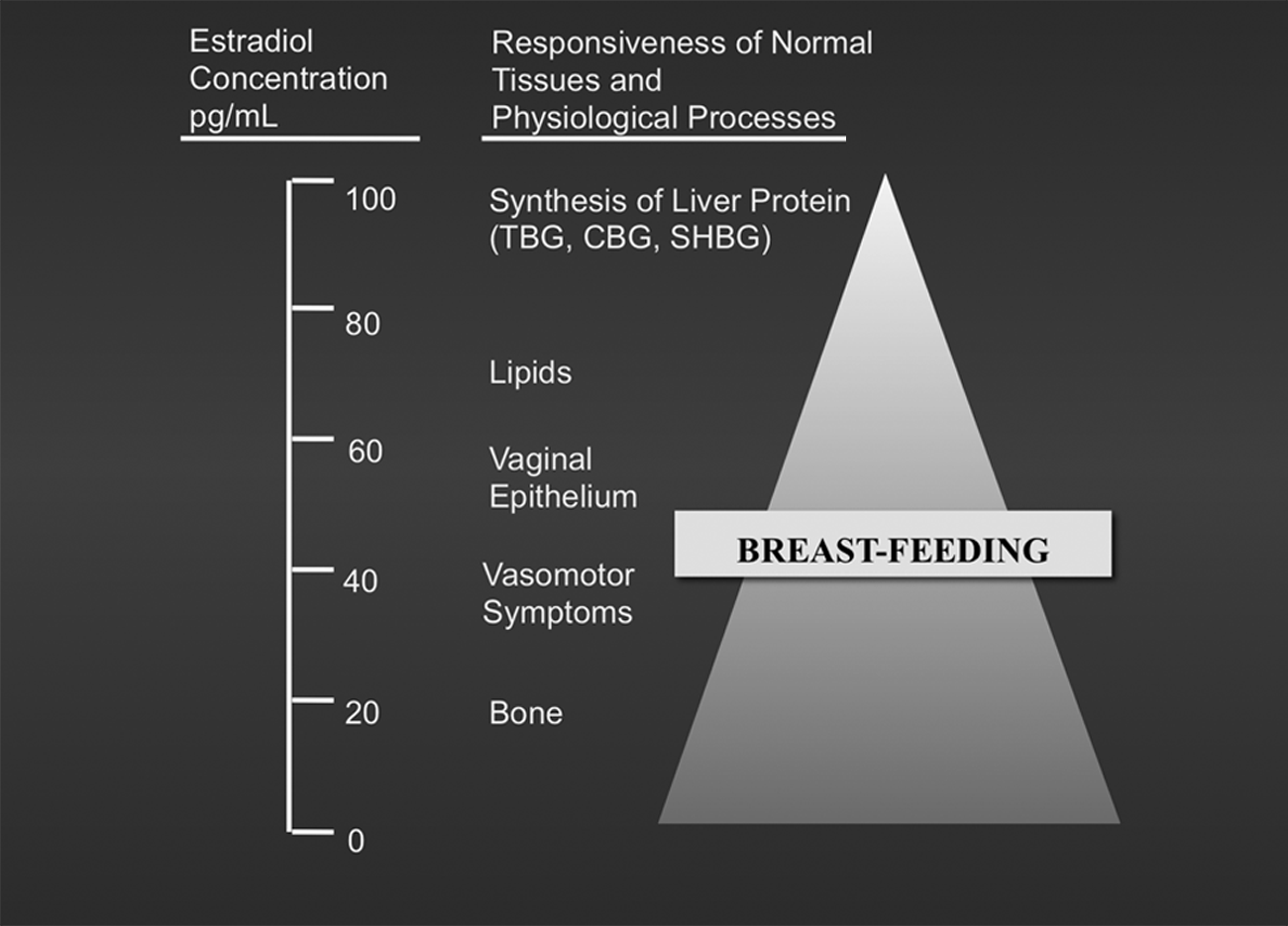
The impact of breastfeeding-induced hypoestrogenemia as predicted by the Estrogen Threshold Hypothesis modified from Barbieri. 1 CBG, corticosteroid-binding globulin; SHBG, sex hormone-binding globulin; TBG, thyroxine-binding globulin.
Subjects and Methods
After Institutional Review Board approval at Cedars-Sinai Medical Center (Los Angeles, CA) was received, consecutive postpartum women were recruited as unpaid volunteers. Eligible candidates were postpartum women who had delivered a healthy baby. Women were evaluated prior to hospital discharge and at 3 and 6 weeks postdischarge. Each time period was analyzed independently, in a cross-sectional design, where women were categorized as “breastfeeding” if they claimed to breastfeed at least two-thirds of the time, as “bottle feeding” if they claimed to bottle feed at least two-thirds of the time, and as “both” if they were intermediate between these extremes. Women who pumped and then bottle fed were classified as breastfeeders. The survey during hospitalization requested women's intent regarding feeding, and the survey at 3 and 6 weeks requested their experience of feeding over the prior week. Any subject who was categorized as intermediate between breastfeeding and bottle feeding was excluded from any comparative analysis at that time period.
Any subject with a history of a psychiatric disorder, current usage of beta-blockers or intravenous magnesium sulfate, current symptomatic thyroid disease, or fever during the postpartum period was excluded from the study population.
Data were collected through a supervised self-administered survey instrument prior to discharge, which was designed using previously validated questionnaires; further evaluations were performed at 3 and 6 weeks postpartum through telephone interviews using the same 26-item instrument. Serum hormonal profiles were not obtained.
Hypoestrogenic clinical symptoms were assessed with the Kupperman Index (KI), 9 and postpartum mood changes were assessed with the Stein Survey (SS). 10
The KI addresses the following symptoms: hot flashes, numbness, insomnia, sadness, dizziness, fatigue, joint aches/pains, headache, heart palpitations, and itching. The KI score was calculated by having the patient self-rank the severity of her symptoms on a 0–3 scale, with 3 being the most severe. The KI weights each symptom on a 1–4 scale depending upon the relative importance of the symptom. For each symptom, the self-ranked severity score was multiplied by the symptom weight to yield a final numerical score for that symptom. The sum of the scores for all symptoms was the total KI score. The KI score was then ranked: a score of 0–14 indicated none to mild symptoms, 15–20 indicated moderate symptoms, and >21 indicated severe symptoms.
The KI was modified slightly to accommodate the needs of the present study: terminology was updated (e.g., “formication” was changed to “itching”), and two additional questions were asked to determine the frequency and severity of hot flashes, a major symptom of hypoestrogenemia. The hot flashes were ranked as low frequency if one to five episodes occurred daily, the occurrence of six to 10 episodes was ranked as moderate frequency, and the occurrence of >11 episodes was ranked as high frequency. Hot flash severity was ranked on a 0–3 scale, with 0=no hot flashes, 1=mild hot flashes, 2=moderate hot flashes, and 3=severe hot flashes. In addition, patients were asked regarding the existence of another major hypoestrogenic symptom, vaginal dryness.
The KI has been criticized in the past with respect to its validity for recording mood changes related to low estrogen levels. 11 To compensate for this, an additional instrument for assessment of mood symptoms in the postpartum period, the SS, was used to identify postpartum depressive symptoms. The SS assesses for the presence and severity of the following symptoms: depression, tearfulness, anxiety, tension, restlessness, exhaustion, dreams/nightmares, and appetite changes. 10
The SS score is calculated by having the patient self-rank the severity of her mood symptoms on a 0–3 scale. The sum of the scores for all the symptoms provides the final score, which can range from 0 to 26. A score of 8 or more usually indicates that significant mood symptoms are occurring.
The survey instrument also assessed for the presence of potential confounders, including soy intake (average number of weekly servings) and birth control type and usage. Particular attention was paid to the type of contraception used.
The data were analyzed using SAS statistical software (SAS Institute, Cary, NC). Where applicable, data are shown as mean±SD with range. Statistical significance is defined as p<0.05 at each time period. Comparisons of categorical data were performed using chi-squared analyses with Yates's correction. Comparisons of continuous data were performed using Student's t test or the Kruskal–Wallis test, as appropriate. For each time period, multivariate logistic regression techniques were used to articulate the independent association of maternal age, hormone use, and soy intake with four outcomes: any hot flashes, vaginal dryness, KI score, and SS score. Odds ratios (ORs) and 95% confidence intervals (CI) were determined. No trend analyses were performed.
Results
The study population consisted of 244 postpartum women. Of these, eight women were excluded for the following reasons: loss to follow-up at one of the subsequent observations (n=5), development of postpartum fever (n=2), and discovery of a preexisting psychiatric disorder (n=1). Thus, in total, 236 women (97%) were followed up over a 6-week interval. Table 1 shows the categorization of study subjects by feeding method at each of the three time points, as specified by the survey instrument. Fifty-eight (24.6%) reported bottle feeding throughout the study, and 140 (59.3%) consistently reported breastfeeding. The remaining 38 (16.1%) were inconsistent in their feeding method. Of these, 21 (8.9%) initially indicated the desire to breastfeed but at both 3 and 6 weeks were bottle feeding. Another seven (3%) switched to bottle feeding at some point between the 3- and 6-week surveys.
Data are number of women (%).
As shown in Table 2, there was no difference in the mean age of the breastfeeding and bottle-feeding groups, as determined with cross-sectional analyses of all women at each of the three time periods. The large majority of women did not use a specific birth control method other than abstinence during the 6 weeks of study. Approximately 3% in each group used the progestin-only pill for contraception. Soy consumption was infrequent.
Age is given as mean±SD (range).
COCP, combined oral contraceptive pills; MPA, medroxyprogesterone acetate.
Hypoestrogenic symptoms are described in Table 3. Overall hypoestrogenic symptomatology as measured by the KI and SS was low and similar for both feeding groups at all time intervals. Hot flash frequency and severity are described in Table 4 and Figure 2. Although a slightly higher proportion of breastfeeding women mentioned the presence of hot flashes compared with bottle-feeding women, this difference was not great and was not statistically significant. Median SS scores were similar for both groups at all time intervals.
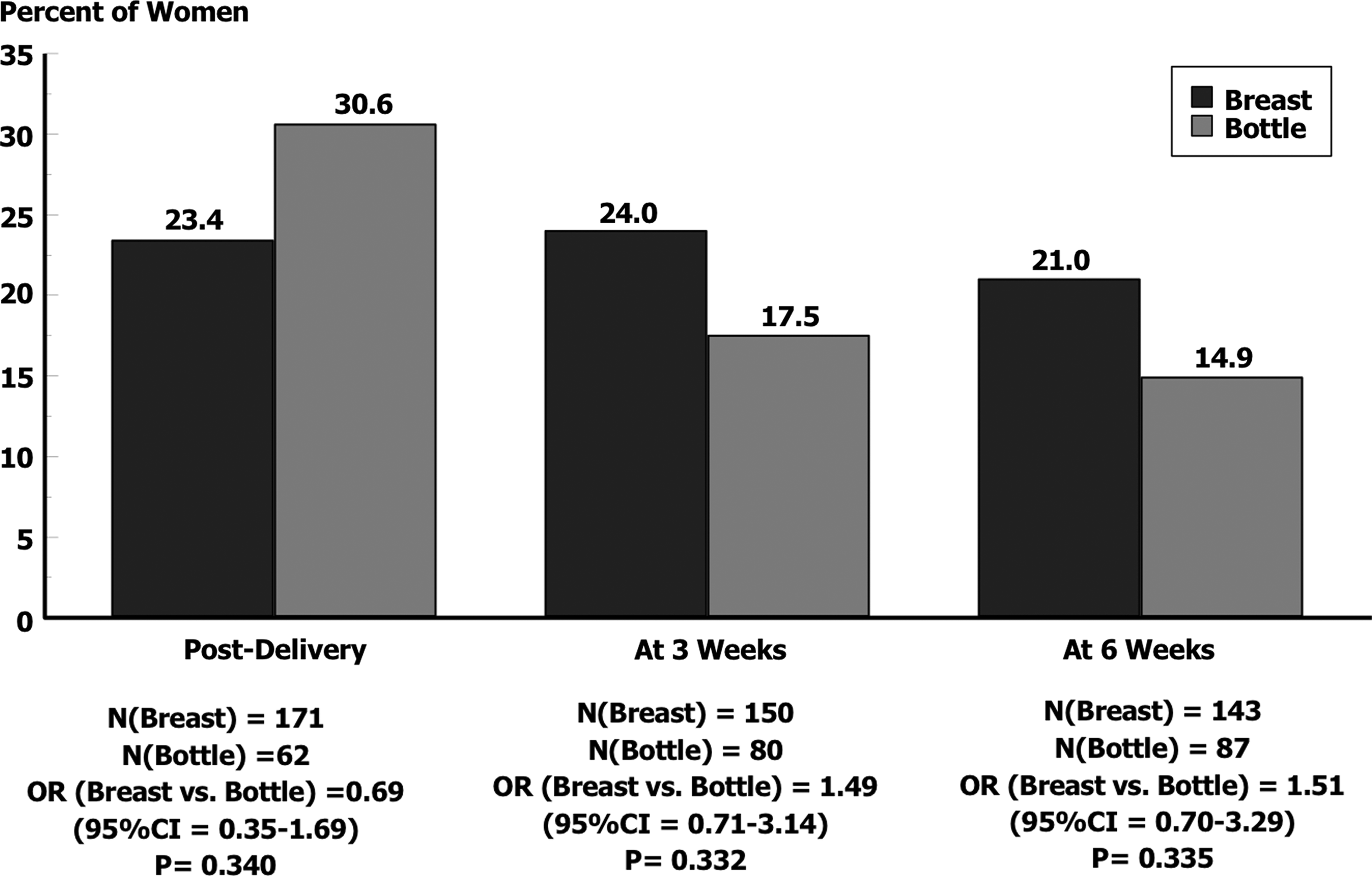
Percentage of breastfeeding and bottle-feeding women reporting the presence of hot flashes at each time point. CI, confidence interval; OR, odds ratio.
Women using both feeding methods were excluded.
Statistically significant at the ap<0.05, bp<0.01 level.
Kupperman Index (KI) and Stein Survey (SS) are given as median (range).
HF, hot flash occurrence; VD, vaginal dryness occurrence.
Vaginal dryness was the only variable measured that appeared to differ between the two groups (Fig. 3). In the immediate postpartum period, only one of the women with an intention to breastfeed had vaginal dryness, compared with two women in the group intending to bottle feed (p=0.356). At 3 weeks postpartum, 13.3% of breastfeeding women reported vaginal dryness, compared with only 3.8% of the bottle-feeding women (p=0.038). At 6 weeks, 17.5% of women who were breastfeeding and 2.3% of women who were bottle feeding reported vaginal dryness (p=0.001).
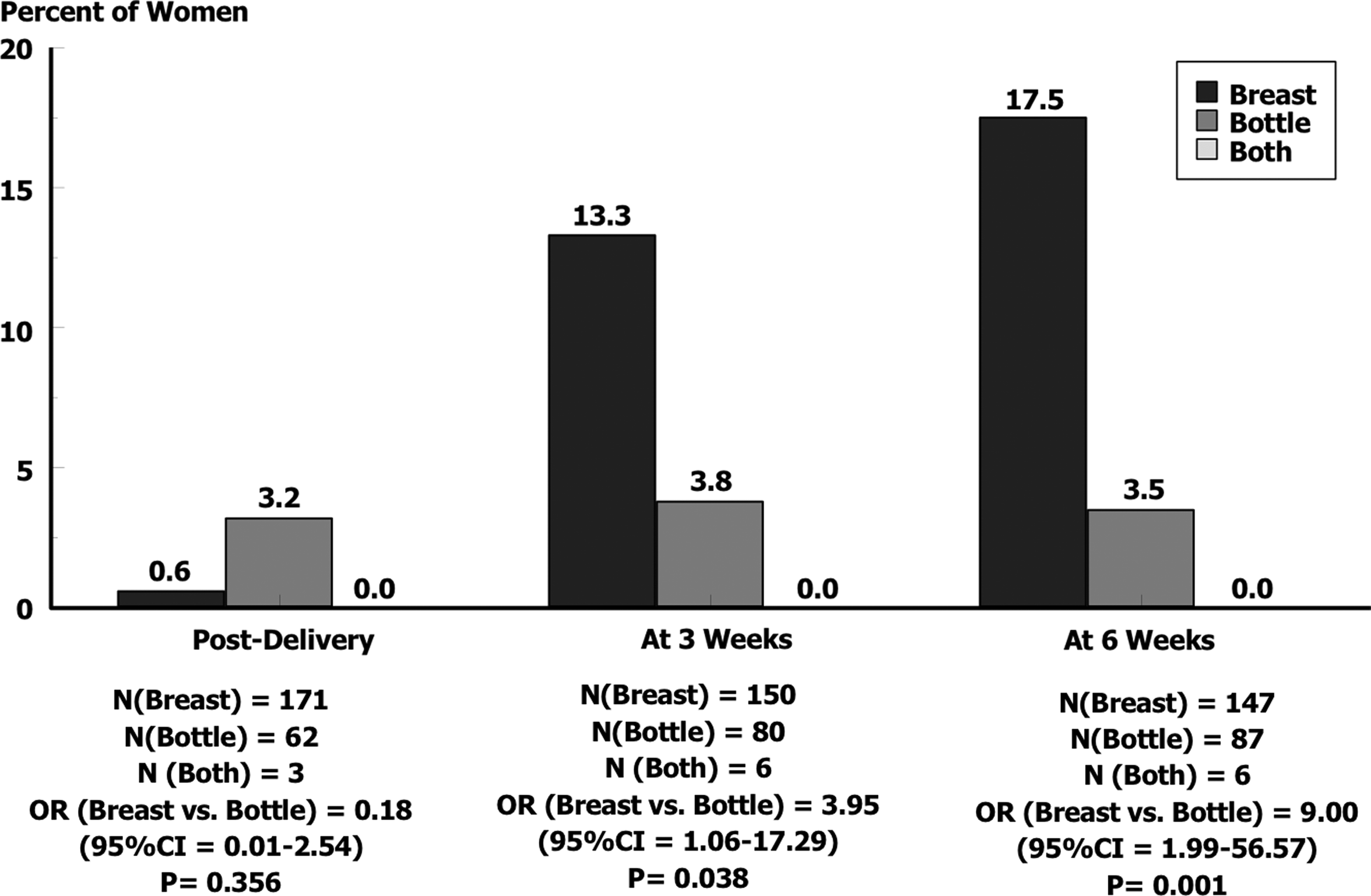
Percentage of breastfeeding and bottle-feeding women reporting the presence of vaginal dryness at each time point. CI, confidence interval; OR, odds ratio.
Because this was an observational study in which women reported their feeding behaviors and in which they might elect to change those behaviors at any time, an exploratory analysis of those women who chose only to breastfeed or bottle feed throughout the 6-week study period was conducted. Women were excluded if they belonged to the classification identified as “both” in Table 1. Such an exclusion yielded 140 consistent breastfeeders, 58 consistent bottle feeders, and 38 women with inconsistent feeding behavior, or a lack of preference for breastfeeding versus bottle feeding. These 38 women were overwhelmingly asymptomatic with respect to vaginal dryness (although they reported similar numbers of hot flashes) and were predominantly women who stated that they intended to breastfeed, but actually bottle fed. Nevertheless, analyses for each time period performed for this population yielded results that were similar to those previously presented in Figure 2: postdelivery report of vaginal dryness, 1/140 (0.71%) for breastfeeding versus 2/58 (3.45%) for bottle feeding, OR=0.20 (95% CI, 0.01–2.91), p=0.427; 3 weeks postpartum, 20/140 (14.29%) for breastfeeding versus 2/58 (3.45%) for bottlefeeding, OR=4.67 (95% CI, 1.00–29.96), p=0.050; and 6 weeks postpartum, 25/140 (17.86%) for breastfeeding versus 2/58 (3.45%) for bottlefeeding, OR=6.09 (95% CI, 1.33–38.58), p=0.014.
Multivariate logistic models using vaginal dryness as the dependent variable confirmed the univariate results reported above. Controlling for maternal age, hormone use, and soy intake yielded an OR (breastfeeding versus bottle feeding) of 3.35 (95% CI, 0.94–12.02), p=0.063 at 3 weeks postpartum, compared with an OR of 8.11 (95% CI, 1.84–35.70), p=0.006 at 6 weeks postpartum. No differences among the groups for the occurrence of hot flashes were noted. With respect to the KI scores, the KI was used as the dependent variable dichotomized between 0 and 1. The OR (breastfeeding versus bottle feeding) was 1.78 (95% CI, 0.99–3.19), p=0.056 for the 6-week postpartum evaluation. Also, the SS score (dichotomized between 0 and 1) appeared borderline elevated with OR=1.71 (95% CI, 0.99–2.98), p=0.056 among the breastfeeding group at the 6-week evaluation.
Discussion
The major findings from this study were that during the first 6 postpartum weeks, women who primarily breastfed their infants experienced (1) more vaginal dryness and (2) a similar number and intensity of hot flashes compared with women who primarily formula-fed their infants. In addition, there appeared to be a borderline significant difference (p=0.056) in mood between the two groups, although the statistical power of this difference was limited. These findings are consistent with the Estrogen Threshold Hypothesis and have importance when counseling women regarding the impact of breastfeeding on these quality of life parameters.
Although symptoms and clinical findings typically associated with postpartum hypoestrogenemia (i.e., postpartum mood changes and bone mineral density) have been investigated,12–14 other symptoms like vaginal dryness and hot flashes have not been well studied. A review of the literature for such symptoms revealed mostly anecdotal reports. A typical example is found in a breastfeeding textbook, which states, “As in menopause, lactation-related hypoestrogenemia, can cause vaginal epithelium to be very thin and to secrete little fluid during arousal. Dryness and pain are experienced during intercourse and vaginal tears are possible..,” yet the text does not provide any references to support this statement. 15 Overall, symptoms such as vaginal dryness and hot flashes appear to be uncommon in the postpartum population. However, vaginal dryness does seem to be significantly more prevalent in the breastfeeding population.
The vaginal dryness without significantly more hot flashes in the lactating group can be explained by the Estrogen Threshold Hypothesis. 1 The Hypothesis, which was derived from observations during menopausal hypoestrogenemia, is typically applied to the treatment of endometriosis. The underlying premise of this hypothesis is that tissues vary in their sensitivity to estrogen. According to the hypothesis, vaginal dryness would occur once estrogen levels drop below about 40–50 pg/mL, and when estrogen levels drop below about 30 pg/mL, hot flashes would be more notable. From previous studies, we know that postpartum lactating women have estrogen levels in the ranges in which vaginal dryness typically occurs.2,5 Estrogen levels tend to be lower in women who breastfeed more regularly and maintain amenorrhea. In this group, the degree of hypoestrogenemia is such that hot flashes are more likely.1,3
It is of note that our study population included a small number of women using hormonal contraception (Table 2). The use of these agents would be expected to reduce hypoestrogenic symptoms and thus decrease our ability to detect differences between groups. By including these women in our calculations, we have “washed-out” the effect of breastfeeding to some small extent and would be expected to have biased the reported OR toward the null. It is notable, therefore, that the effect of breastfeeding with respect to vaginal dryness still remained “detectable” despite the inclusion of hormonal contraceptive users. Our calculation provides a somewhat more conservative analysis of symptoms than would be suggested by a “pure” analysis that excluded women using hormonal contraception.
It is clear that vaginal dryness can lead to dyspareunia. Because the Estrogen Threshold Hypothesis refers to vaginal dryness rather than dyspareunia, we did not assess dyspareunia specifically. Our finding of increased vaginal dryness in breastfeeders supports data demonstrating increased dyspareunia in this group. 16
An interesting observation in Table 2 is that women that reported consuming soy-based products tended to have more hot flashes. It is known that that dietary soy contains chemicals (isoflavones) with weak estrogenic activity at some body sites and anti-estrogenic activity at others. 17 We speculate that because soy isoflavones lower estradiol levels in cycling women by 20–40%, 18 then in lactating women, a similar decrease would drop estradiol levels from approximately 50 pg/mL to about 30 pg/mL. According to the Estrogen Threshold Hypothesis, this further lowering in circulating estradiol levels would be sufficient to induce increased hot flashes.
The effect of hypoestrogenemia on postpartum psychological changes has been researched by various investigators.12,19 To date, the exact mechanism of action by which postpartum depression symptoms are affected by disturbances of the hypothalamic–pituitary–ovarian axis remains unknown. Although the present study did not detect significant psychological differences between lactating and nonlactating women, other investigators have found that depression symptoms were improved by hormone replacement therapy. 19 In a double-blind, placebo-controlled study of 61 women receiving transdermal estrogen for treatment of postpartum depression, the postpartum women receiving transdermal estrogen improved more rapidly and significantly compared with the control group. 19
A limitation of this study is that the study population was divided into just three groups—based on how they fed their infant the majority of the time. More detailed categorization of extent of breastfeeding may have allowed us to better discriminate between the symptoms that were and were not associated with breastfeeding. In addition, the frequency of nipple and areola stimulation for nonlactational purposes was not monitored. Because such stimulation can affect the degree of hypothalamic suppression, it may have had a confounding effect if it were more prevalent in one feeding group than the other.
The present study was able to detect a difference in vaginal dryness between the lactating and nonlactating populations. More studies are needed in order to confirm this phenomenon. Also, the results of future studies could help develop treatments that optimize the breastfeeding period for both mother and infant. We hope that this study will provide the basis for conducting a larger, more detailed study directly evaluating estrogen levels and associated hypoestrogenic and psychological effects in the lactating and nonlactating postpartum state.
Footnotes
Disclosure Statement
L.M.K. is an employee of Childbirth Research Associates. C.L.H. is an employee of Quintiles, Inc. S.K.A. and J.K. declare no competing financial interests exist.