
Abstract
Abstract
Background:
Severe breast engorgement can cause substantial discomfort for mothers and interfere with an infant's ability to feed at the breast. This study explored the possibility of prediction of pathological postpartum breast engorgement in lactating women in relation to intense breast engorgement at the end of the luteal phase of the menstrual cycle and the possibility of prevention and resolution of postpartum breast engorgement with expression with a breast pump of colostrum before the appearance of transitional milk.
Subjects and Methods:
The first group included 70 women with pathological postpartum breast engorgement. The second group included 52 postpartum women, with 24 women having colostrum extracted by the breast pump from each breast once or twice for a duration of 20–25 minutes sequentially in the first 2–3 days after delivery in addition to the removal of colostrum by the baby, before engorgement developed. Twenty-eight women had colostrum removed only by the baby. The degree of breast engorgement was assessed using the previously published Robson four-level scale.
Results:
Of the 70 patients with severe postpartum engorgement studied in the first group, 90% showed intense breast engorgement in the late luteal phase of the menstrual cycle. Expression of colostrum milk in the first experimental group from each breast eliminated excessive breast engorgement in breastfeeding mothers.
Conclusions:
Presence of intense breast engorgement at the end of the luteal phase of the menstrual cycle may be one of the most important indicators useful for predicting severe postpartum breast engorgement. Extraction of colostrum before the appearance of transitional milk lowers the risk of excessive engorgement in breastfeeding women.
Introduction
N
At the same time, for some postpartum women the engorgement process does not lead to complications; for others, the engorgement may become pathological. Mammary glands may become very hard and painful. The skin on the breast surface becomes red, the temperature increases, the areola becomes tense and hard, and the nipple is sometimes flattened out. The baby encounters serious nursing difficulties and in most cases refuses the breast. As a result, intense pain caused by engorgement forces some women to give up breastfeeding and switch to an easier way of feeding the baby, with milk formula from a bottle. 3
Clinical observations indicate that the main reason for and the severity of the engorgement are associated primarily with a total volume of secretory substances in lactiferous ducts (i.e., the transitional milk that has come in and the nonexpressed antenatal colostrum 4 ). Here it should be noted that a phenomenon similar to postpartum breast engorgement may occur in women in the late luteal phase of the menstrual cycle. It is related to the increase in parenchymal and stromal breast tissue and the filling of alveolar buds and ducts with secretion that compositionally resembles colostrum, under the influence of the increased concentration of prolactin during the second half of the luteal phase.5,6 In addition, vascularization and blood velocity in mammary glands increase at the end of the luteal phase. 7 All this leads to an increase in the size and density of the gland before menstruation. 8
By analogy with postpartum breast engorgement, this state of the mammary gland is sometimes called “premenstrual engorgement,” which is also a normal physiological process. However, the degree of “premenstrual engorgement” as well as postpartum engorgement varies among women.
Clinical examinations show that in some cases there is only a slight increase in mammary gland density. In other cases, women experience a feeling of bloating and heaviness in the mammary gland; palpation of the gland may reveal lumps, while the process itself is sometimes accompanied by painful sensations. Intensity of sensations, perhaps, just like in the case of postpartum engorgement, will primarily depend on the degree of secretory accumulation in lactiferous ducts and alveolar buds and, therefore, on the stretching of the duct walls and stimulation of afferent nerve endings 9 located close to lactiferous ducts. Probably, with a different volume of secretion produced by the end of the luteal phase, women with larger amounts of secretion will experience more intensive stretching of the duct walls and, accordingly, increased stimulation of mechanoreceptors, and, in the case of duct walls being sufficiently stretched, pain receptors will be activated. If secretion is not intensive, lactiferous ducts will be stretched insignificantly, and thus the unpleasant sensations will be slight or absent. 10
Here it is possible to make two assumptions. First, women with intense “premenstrual engorgement” associated with genetic, physiological, and anatomical properties of their mammary glands will also experience more intense postpartum breast engorgement. Second, as the main cause of breast engorgement is difficulties in removing milk from lactiferous ducts “blocked” with colostrum, 4 additional preventive extraction of colostrum in the first days after delivery will eliminate the risk of intense engorgement for these women. Results of the research aimed to verify these assumptions are presented in this article.
Subjects and Methods
The study was conducted at the postnatal unit of the D.O. Ott Institute of Obstetrics and Gynecology, St. Petersburg, Russian Federation. In the first part of the study, investigators examined 70 patients from the postnatal unit of the D.O. Ott Institute of Obstetrics and Gynecology who sought medical advice in connection with severe postpartum breast engorgement. Fifty-four of them were primiparous breastfeeding mothers, and 16 were multiparous mothers. Infants of all patients were exclusively breastfed. Simultaneously with the 70 women with severe postpartum engorgement, 76 women without severe engorgement were surveyed (the control group). In patients with vaginal birth, the child was applied to the breast within the first hour after birth, and in patients with cesarean section, the infant was shown to the breast on the second day after birth. The delay in first feed for women with cesarean delivery was caused by the women's fatigue due to surgery. This procedure is among the rules of the D.O. Ott Institute clinic. Infants were breastfed six to eight times within a day. Information about the women participating in the study and their babies is shown in Table 1.
The difference between the first day of occurrence of engorgement in women with vaginal delivery and cesarean section in both groups was insignificant (p≥0.05).
Four women in the group of nulliparous women with cesarean section had twins.
One woman in the group of multiparous women with vaginal birth had twins.
The second part of the study included examination of 52 patients also from the postpartum unit of the D.O. Ott Institute of Obstetrics and Gynecology. Among these, on the first or second day for 24 women who had vaginal delivery and on the second or third day for women who had cesarean delivery, milk was extracted by a breast pump once or twice for a duration of 20–25 minutes from each breast sequentially in addition to the extraction of the milk by the child. The patients were randomly selected for the pump intervention. The control group included 28 postpartum women who had milk removed only by nursing babies. Information about the women participating in the second part of the study and their children is provided in Table 2.
Two of the women in the control group had twins.
The informed consent of the women was obtained in accordance with the Declaration of Helsinki. The study was approved by the Ethical Committee of the D.O. Ott Institute of Obstetrics and Gynecology.
In order to prevent or resolve breast engorgement, milk was extracted with the use of a special hospital-grade electric breast pump. Unlike breast pumps that use only vacuum for milk expression, this pump stimulates the areola with both vacuum and compression stimuli similar to removal of milk by the baby, 11 which increases the efficiency of milk expression. 12 The pump includes a control unit and a removable cup placed on the mammary gland. Vacuum and overpressure stimuli were supplied to the removable cup from the control unit through air hoses in a definite sequence with a frequency of 60 pulses/minute. The pump first applied vacuum stimulus, which reduced the atmospheric pressure by 18–20 kPa inside a transparent elastic conical tube inside which the nipple and areola of the breast were placed. When the maximum vacuum has been achieved, an overpressure stimulus was supplied to the air chambers for compressing the areola. The pressure of the membranes of the air chambers was transferred to a lever mechanism, which directly compressed the conical tube and the areolar part of the mammary gland with mammary sinuses that it enclosed. The amplitude of the pressure stimuli applied to the breast areola was regulated the patient herself. It was usually within the limits of 35–40 kPa. The time of action of the vacuum and compression stimuli lasted 0.5 second; the stimuli were then switched off, followed by a 0.5-second rest period.
The degree of breast engorgement was assessed using a four-level scale developed by Robson 13 (Table 3). In the first part of the work 70 patients were enrolled; a survey on the extent of premenstrual engorgement was conducted immediately after the women went to the doctor because of a severe postpartum engorgement. Direct assessment of the degree of postpartum engorgement (according to the criteria of Robson 13 ), as well as assessment of premenstrual engorgement (as per the reports of the patients), was carried out by the same doctor. In the second part of the work, in order to get more objective data from an experimental and a control group of patients, a survey on the degree of premenstrual breast engorgement was also conducted by the same doctor after postpartum breast engorgement occurred in patients (3–5 days).
Average data are given with standard deviation. Student's t test was used for statistical analysis.
Results
In the first part of the study, the examination did not reveal any differences in breast engorgement between postpartum women who had vaginal delivery and those who had cesarean delivery. Patients who had a cesarean delivery showed a tendency for later development of breast engorgement than patients who had vaginal delivery, but this difference was insignificant (Table 1). Breast engorgement observed in the patients could be classified as Level 3–4 on the Robson scale 13 (Table 3). The additional survey found that the entire breast or its separate parts became hard and painful, and significant hyperthermia and hyperemia of the skin covering the gland were reported. The areola became stiff and lost elasticity. The nipple was sometimes flattened out. In most cases, the breast experienced a 1.5–2.0 increase in size compared with its size prenatally.
A survey among nulliparous women showed that before pregnancy in the late luteal phase of the menstrual cycle, the majority of women experienced hardening of mammary glands and breast pain on palpation (Table 4).
Data are number of women (%).
The postpartum engorgement in multiparous women is of great interest, as the medical literature contains statements that the engorgement process in multiparous women is less painful than in primiparous women. A survey among multiparous women concerning the degree of breast engorgement after the first birth and also the degree of engorgement before the first pregnancy in the late luteal phase of the menstrual cycle (Table 4) produced data similar to that of engorgement in the second birth.
Simultaneously with 70 women with severe postpartum engorgement, 76 women without severe engorgement were surveyed. According to the Robson scale, their engorgement can be defined as Level 1–2. Only 34 women had premenstrual engorgement, which manifested itself in the hardening inner part of the breast.
All postpartum women participating in the study experienced difficulties in breastfeeding in connection with breast engorgement. The main reason was the increased stiffness of the areola and retraction of the nipple. The presented data allowed the assumption that preventive partial removal of colostrum would reduce breast engorgement and help the infant to extract milk from the mammary gland more efficiently. Therefore, the second part of the study dealt with the influence of preliminary preventive expression of colostrum on development and severity of breast engorgement.
Patients were divided into two groups: an experimental group and a control group. In the experimental group, in addition to the removal of milk by the baby, breastmilk was extracted with the breast pump; in the control group breastmilk was removed only by the baby.
In the experimental group of patients (n=24), colostrum was expressed with a hospital-grade electric breast pump from each breast once or twice for a duration of 20–25 minutes sequentially, following the regular breastfeeding, on the first or second day after birth. At that time, none of the patients yet showed any breast engorgement. Based on the dynamics and the amount of colostrum extracted, patients could be divided into two subgroups.
In the first subgroup (n=14), at the beginning of milk extraction by the breast pump from both breasts for 5–6 minutes, only a few drops of colostrum would be removed. Later on, the flow of colostrum would become more intensive. The first portion of colostrum was the thickest and the most viscous. The total amount of colostrum extracted by expression ranged between 2 and 10 mL. In the second subgroup (n=10), patients did not experience any delay in the removal of colostrum. Colostrum appeared after 1–1.5 minutes, and its removal rate was sometimes as high as 3–4 mL/minute. Colostrum was less viscous than in the first subgroup. The total amount of colostrum extracted by expression ranged between 10 and 70 mL.
Women from the experimental group who had had vaginal delivery experienced breast engorgement on the third or fourth day. Women who had had cesarean delivery showed a tendency for later breast engorgement (on the fourth or the fifth day). Based on the properties, breast engorgement could be classified as Level 1–2 (Table 3) (Fig. 1A), when mammary gland density increased but there were no painful sensations. There was no change in skin color, or slight hyperemia was reported. Temperature remained normal or was slightly elevated but did not exceed 37°C. The baby could easily make a “teat” out of the areola and the nipple and remove transitional milk.
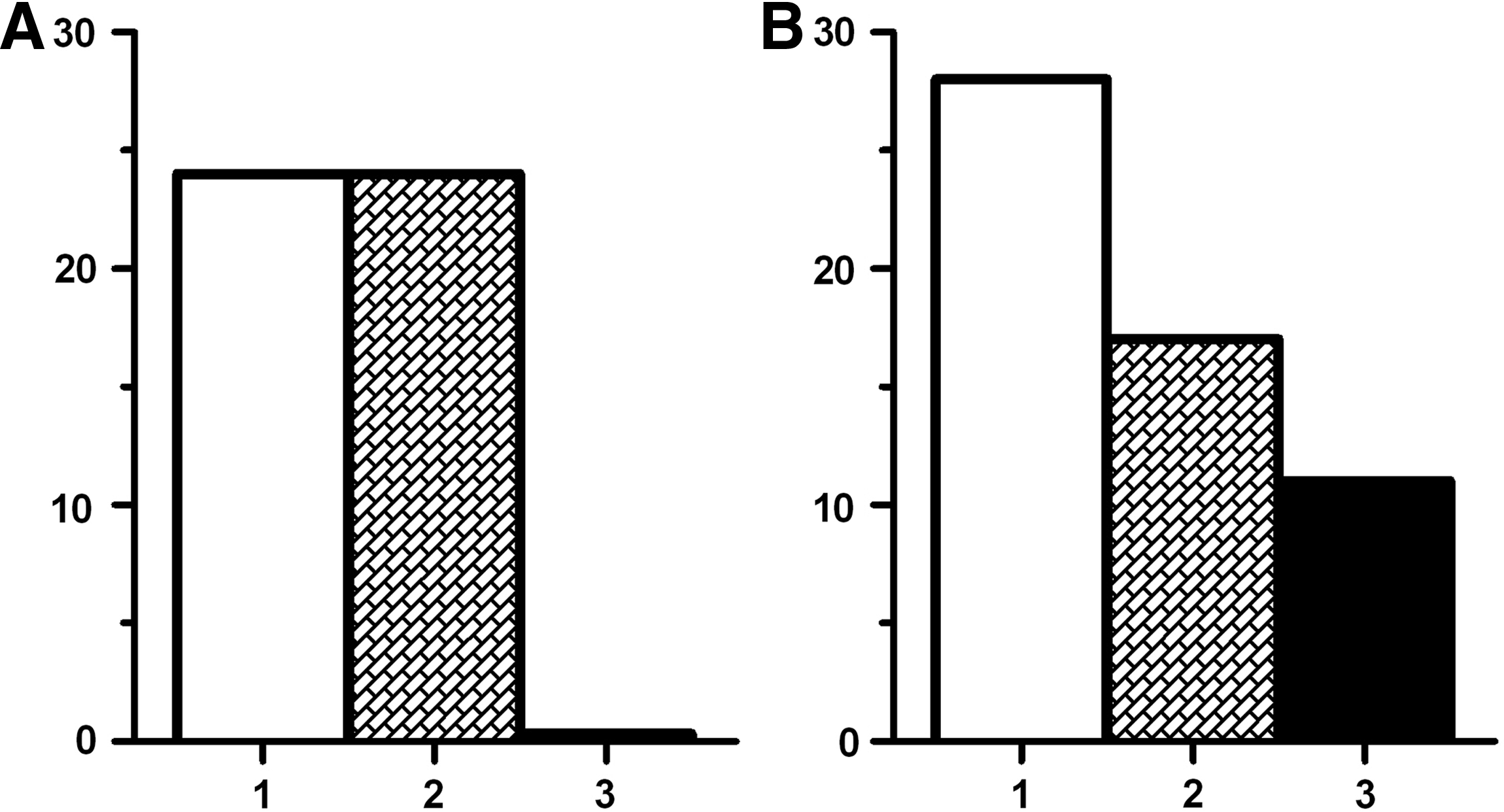
Effect of preliminary pumping of the breasts on the occurrence of a pathological postpartum engorgement:
Three multiparous women reported severe breast engorgement after previous births. For them, the development of lactation process was painless after preliminary colostrum expression.
In the control group (n=28), 11 patients (40%) showed excessive breast engorgement (Fig. 1B), which could be classified as Level 3–4 (Table 3), with four patients reporting abnormal breast engorgement after the first birth as well. The entire breast or its separate parts became hard and painful and also showed significant hyperthermia and hyperemia of the skin covering the gland. The areola became stiff and lost elasticity. The nipple was flattened out. The baby encountered difficulties when removing transitional milk and in most cases refused the breast. In these cases, breast engorgement, just like it was the case with patients in the first part of the study, was resolved by extracting colostrum with a hospital-grade electric breast pump. Complete resolution of breast engorgement usually required two extraction sessions with the hospital-grade electric breast pump.
Discussion
With the occurrence of puberty and the onset of ovulatory cycles in women, the entire reproductive system, including the mammary glands, which are an integral part of it, every month gets into a state of readiness for reproduction of offspring. The ovulatory menstrual cycle is accompanied by significant changes in hormone levels in women's blood: gonadotropic and steroid hormones as well as prolactin and oxytocin.4,5,14–17 Influenced by the high concentration of steroid hormones, branching of the mammary gland intensifies. Lobules increase in volume because of the development of additional primary ducts with alveolar buds that structurally resemble the alveoli of a lactating mammary gland. The increased prolactin levels and decreased levels of progesterone 5 in the second half of the luteal phase enhance secretory activity in alveolar buds and lactiferous ducts. As a result, cavities in milk ducts and alveolar buds are filled with secretion and become significantly dilated, while the duct walls expand. The number of alveolar buds formed by the terminal duct increases, and the size of lobules increases accordingly.
During the luteal phase, distinct changes in the arrangement of collagen fibrils in the intralobular stroma take place. This is due to the increased water content in the intercollagen space, induced by steroid hormones and prolactin. 18 Besides, there is increased vascularization and blood velocity in mammary glands at the end of the luteal phase. 7 All this causes an increase in the size and density of the mammary gland before menstruation. 8
Clinical examinations show that in some cases there is a slight increase in mammary gland density, whereas in other cases painful sensations appear. In clinical practice this phenomenon became known as cyclic mastalgia. 19 It should be noted that the feeling of fullness and pain can occur only when the cerebral cortex of the woman receives nervous impulses from afferent receptors located in the inner part of the breast. 9 With a different volume of secretion produced during the luteal phase, women with larger amounts of secretions will experience more intensive stretching of the duct walls and, accordingly, increased stimulation of mechanoreceptors, and in the case of duct walls being sufficiently stretched, pain receptors will be activated. It appears that 90% of postpartum women participating in our study can be included in this group; these women—probably because of their physiological and genetic characteristics—had a higher rate of secretion, and the filling of mammary ducts in the late luteal phase of the menstrual cycle was accompanied by pain. At the same time, if secretion is not intensive, lactiferous ducts will be stretched insignificantly, and thus the unpleasant sensations will be slight or absent. 10
These assumptions are consistent with the results of research that examined connection between painful sensations in the breast and the diameter of milk ducts in women during the second half of the menstrual cycle. Because the degree of accumulation of secretory product in the ductal system is mainly determined by the level of prolactin in the blood, it can be assumed that the decrease in prolactin level will reduce the accumulation of secretory material in the ductal system and hence will reduce painful sensation in the breast. Indeed, clinical data demonstrate that taking bromocriptine or cabergoline, both of which effectively block the release of prolactin from the central nervous system into the bloodstream, during the second half of the cycle, eliminates breast pain. 20
During pregnancy, concentrations of prolactin and steroid hormones in women's blood increase, and by the time of delivery they becomes dozens of times higher compared with the luteal phase. As a result, parenchymal tissue expands, and the space occupied by the stroma decreases. Alveolar secretory cells begin to produce and fill alveolar and ductal cavities with secretory material known as colostrum. Here it should be noted that the amount of colostrum removed by antenatal expression varies greatly among women, 21 and it most likely is the largest in those postpartum women who, because of their physiological and genetic characteristics, experience more intensive filling of the ductal system in the late luteal phase.
After delivery, on the third or fourth day, when a large volume of transitional milk comes in, lactiferous ducts may still be filled with antenatal colostrum, which has greater viscosity and prevents removal of transitional milk. Postpartum women with a high level of milk secretion, a group that supposedly includes women with severe engorgement during the luteal phase of the menstrual cycle, experience congestion of alveoli and lactiferous ducts if the milk is not extracted in sufficient quantities. Thus, the presence of intense breast engorgement at the end of the luteal phase of the menstrual cycle may be one of the most important indicators for predicting severe postpartum breast engorgement.
The primary cause of breast engorgement is blocked lactiferous ducts. Because of plugged ducts, the liquid phase of the milk additionally seeps through the duct walls into the surrounding space, thus causing edema in surrounding tissues. In addition, a significant increase in the size of the alveoli can partly or completely occlude the capillary blood circulation. 4 Congested blood vessels leak fluid into the surrounding tissue space, contributing to edema. Intensive stretching of lactiferous ducts and the presence of edematous liquid lead to sensitization of pain nerve endings that are located close to the walls of medium and thick milk ducts, as well as the walls of blood and lymphatic vessels. 9 Removal of milk becomes extremely difficult for the baby. The main reason is the increased stiffness of the areola and retraction of the nipple. In this case the provision that frequent nursing of the baby would reduce breast engorgement is hard to fulfill. Moreover, in some cases after frequent nursing the baby's gums rub too hard against the nipple's skin, making it sore and worsening the situation. In order to help the baby, lactiferous ducts need to be “unclogged” by the breast pump, which will preventively remove colostrum and a part of transitional milk, so that the areola would become soft and stretchable and the milk would easily pass into the baby's mouth.
Engorgement was eliminated by expressing transitional milk with a hospital-grade electric breast pump. When expressing milk, it was found that simultaneous use of vacuum and compression stimuli significantly reduces the pain of the process. Adequate mechanical stimulation of mechanoreceptors of the areola was necessary for efficient development of the milk ejection reflex. During the first minutes of pumping, glands expressed rather viscous transitional milk. Afterward, when the viscosity of the milk decreased owing to milk expression, the density of separate sections of the mammary gland where milk lobules filled with colostrum are located also decreased. As a result, the density of the whole mammary gland would decrease, and the pain would stop. Pressure on the areola exercised by the compression elements of the breast pump during milk extraction effectively massaged the alveolar area, thus removing edema, reducing the stiffness of the region, and making it comfortable for milk extraction by the baby. As a result, when the baby latched onto the breast, he or she was able to make a “teat” out of the areola and the nipple and remove milk efficiently.
Here it should be noted that in medical literature one can find experimental articles dedicated to research of various methods and techniques aimed at resolving severe postpartum engorgement: acupuncture, cabbage leaves, cold gel packs, pharmacological treatments (protease complex, oxytocin), and ultrasound. Detailed analysis of these effects was carried out by Mangesi and Dowswell. 3 All these methods turned out to be ineffective because they were aimed not at addressing the main cause of breast engorgement (i.e., blocked lactiferous ducts) but at alleviating the painful symptoms arising from this condition.
Conclusions
The presence of intense breast engorgement at the end of the luteal phase of the menstrual cycle may be one of the most important indicators useful for predicting severe postpartum breast engorgement. Expression of colostrum before the appearance of transitional milk lowers the risk of excessive engorgement in breastfeeding women.
Footnotes
Acknowledgments
This study was supported by grant 29690 from St. Petersburg University.
Disclosure Statement
No competing financial interests exist.