
Abstract
Abstract
Background:
Few data are available on the number of stools in exclusively breastfed infants. Two studies aimed to assess the stool pattern in exclusively breastfed infants and to evaluate the reactions of mothers in the case of infrequent stools and the decisions of healthcare providers.
Materials and Methods:
Infrequent stools were defined as an interval of >24 hours between bowel movements. Study 1 concerned 198 infants. Mothers responded to a questionnaire where they described their knowledge and attitude toward infrequent stools. Study 2 was performed using the Internet with 85 French-speaking mothers worldwide responding to a questionnaire on bowel movements and reactions of mothers and healthcare providers. Using the scale provided, mothers evaluated their anxiety and the discomfort of their infants.
Results:
In Study 1, 37% of exclusively breastfed infants experienced at least one episode of infrequent stools that occurred at <1 month of age in 19% of cases. Mothers who were aware of infrequent stools intervened less frequently (17%) than mothers who were unaware of this condition (79%) (p<0.0001). In Study 2, the median duration of all combined episodes of infrequent stools was 10 weeks (range, 1–34 weeks) with a maximal duration of 28 days. The most frequent action for infants was abdominal massage (79%), whereas in mothers it was consumption of fruit juice/mineral water rich in magnesium/vegetables (73%). There was a correlation between the maternal anxiety score and the infant's discomfort score (p=0.0001).
Conclusions:
Parents/health professionals should be informed of the prevalence of infrequent stools in exclusively breastfed infants and adopt a wait-and-see attitude.
Background
B
Mothers are given many recommendations for themselves and their babies, for example, “drink orange juice,” “eat more vegetables and fiber,” “drink mineral water with laxative properties,” etc. Some breastfed infants with so-called constipation may even undergo medical examination including large bowel enema, rectal manometry, and rectal biopsy. It is surprising that very few data are available in the medical literature concerning the number of stools of healthy breastfed infants.
The objectives of the present study were as follows: (1) to assess the prevalence of the infrequent stools in healthy exclusively breastfed infants; (2) to study the characteristics of these infants (age at onset, duration, underlying medical conditions); and (3) to evaluate the reactions of mothers and the decisions made by healthcare providers.
Materials and Methods
Two studies were conducted consecutively. The first study aimed at assessing the prevalence of infrequent stools and mothers' knowledge of the condition and their reaction to it. The second study aimed at describing the characteristics of infants and evaluating the attitudes of parents and healthcare providers. Infrequent stools of the exclusively breastfed infant were defined as an interval of more than 24 hours between bowel movements.
Study 1
Mothers and infants were recruited for the study during La Leche League meetings. Mothers filled out a short questionnaire.
Study 2
Study 2 was based on a structured questionnaire on bowel movements and the reactions of mothers and healthcare providers. The study was performed using the Internet, based on information provided on the La Leche League France Web site www.lllfrance.org/ and other Web sites related to breastfeeding by 85 French-speaking mothers from Algeria, Belgium, Canada, France, Greece, The Netherlands, Singapore, and Sweden. Inclusion criteria were infant age from 10 days to 8 months, exclusive breastfeeding from birth, daily vitamin D and weekly vitamin K supplementation, and recovery of birth weight at a maximal age of 10 days. Growth was considered normal if consistent with the World Health Organization child growth standards. 3 All infants included in Study 2 had experienced at least one episode of infrequent stools during the month preceding the questionnaire. Mothers were responsible for evaluating their anxiety and the discomfort of their infants on a scale ranging from 1 (“relaxed” for the mother and “quiet” for the baby) to 6 (“very anxious” for the mother and “disturbed” for the baby).
Statistics
In this study, given the high number of included/analyzed subjects (n=198), we used parametric testing. Association between two groups was assessed using chi-squared tests. 4 A value of p<0.05 was considered significant. 5
Regulatory requirements
Because this study consisted of a retrospective evaluation and was both noninterventional and anonymous, in accordance with French medical research regulations it required no advance agreement from an independent ethical committee or any declaration to a competent authority concerning personal information technology data.
Results
Study 1
Of the 198 infants recruited during the La Leche League meetings (Fig. 1), 74 (37%) had experienced at least one episode of infrequent stools, which had occurred before 1 month of age in the case of 14 infants (19%). Seventy-two of the 74 mothers (97%) of infants with infrequent stools filled in the short questionnaire. Of 48 mothers (67%) who were aware of this condition, 40 (83%) did not intervene; these mothers said that they were not anxious and waited patiently for the next stool. Of 24 mothers (33%) who were unaware of this condition, only five (21%) did not intervene; the other 19 mothers sought additional information (for example, search for documentation, phone call to a breastfeeding association or healthcare provider, or consultation with a healthcare provider). Mothers who were aware of infrequent stools intervened less frequently than mothers who were unaware of this condition (p<0.0001).
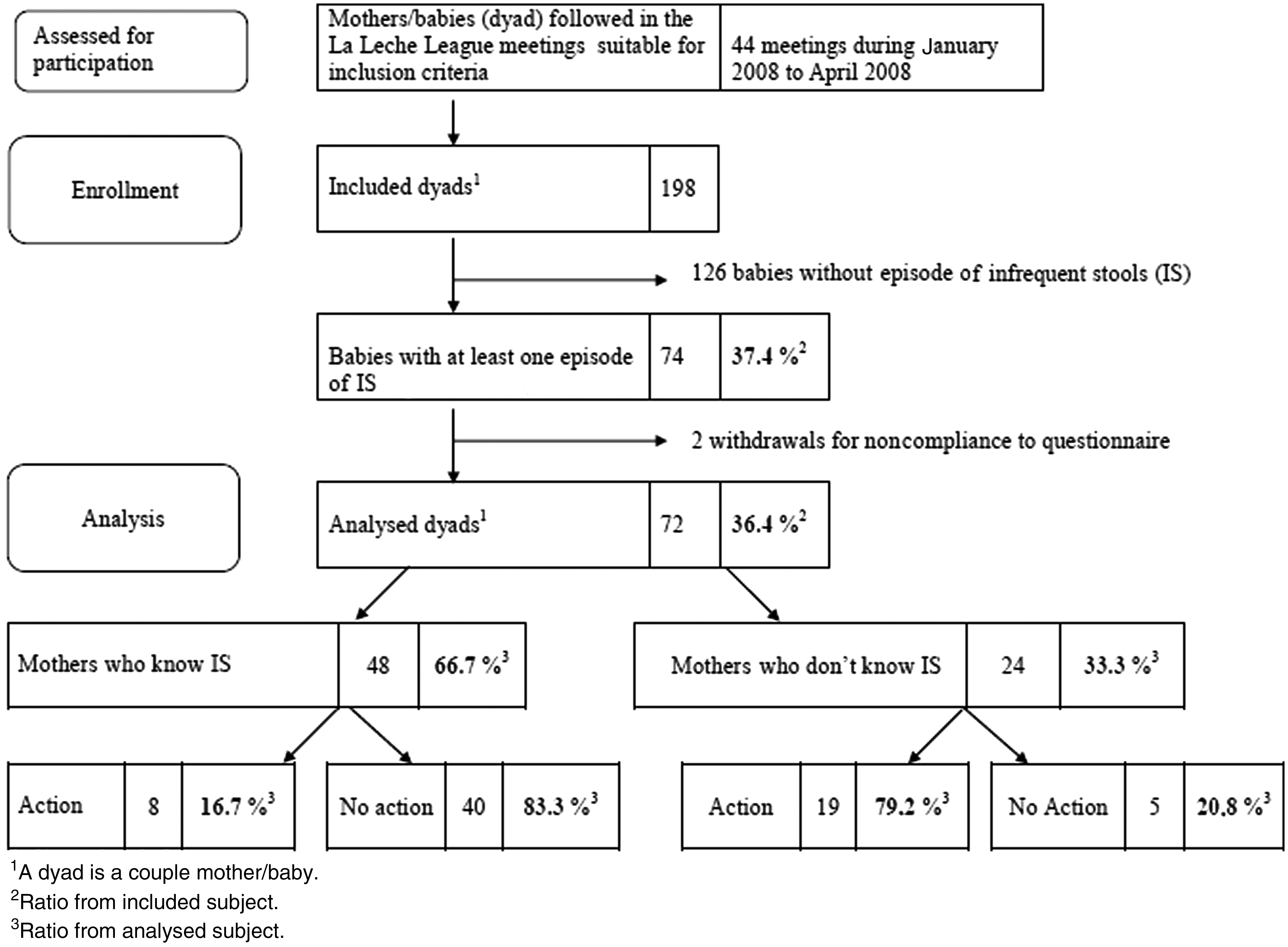
Flowchart of screening, inclusion, and analysis rate in Study 1. IS, infrequent stools.
Study 2
The median age of the 85 infants was 16 weeks, with a range from 10 days to 8 months. The median age at the first episode of infrequent stools was 6 weeks (range, 1–22 weeks). The median daily number of stools before the first episode of infrequent stools was three (range, one to eight). The median duration of the first episode of infrequent stools was 4 days (range, 1–10 days), whereas the median duration of the other episodes was 6 days (range, 2–28 days). The median duration of all combined episodes of infrequent stools was 10 weeks (range, 1–34 weeks). A few mothers spontaneously called the return of stooling “back stools.” The median number of diapers used for stool collection on the day when bowel movements returned was two (range, one to four), with the stools being most frequently described as soft, yellow, and large. No infant experienced hard “back stools.”
No specific action was undertaken in the case of 52 (61%) of the 85 infants, and stools returned to a normal pattern. Specific action was undertaken for 33 infants (39%). The most frequent action for infants (because there are several possibilities for the same infant, the total exceeds 100%) was as follows: (1) abdominal massage, n=26 (79%); (2) use of suppositories and/or anal stimulation and/or enema, n=21 (64%); and (3) consumption of fruit juice and/or mineral water rich in magnesium, n=11 (33%).
The most frequent action for mothers (several possibilities for the same mother) was as follows: (1) consumption of fruit juice/mineral water rich in magnesium/vegetables, n=24 (73%); and (2) miscellaneous (e.g., prokinetics, laxatives, homeopathy, osteopathy, foot massage), n=16 (48%).
The median anxiety score of the mothers during the infrequent stools episodes was 2 (range, 1–6), whereas the median discomfort score of the infants was 1 (range, 1–6). There was a correlation between the maternal anxiety score and the infant's discomfort score (r=0.0001). Mothers who took specific action for either themselves or their baby or both had a higher median anxiety score (3.65) than those not taking specific action (1.78) (p=0.001). Infants undergoing specific action had a higher median discomfort score (2.39±1.59) than those who did not (1.5±1.0) (p=0.02).
Discussion
Our first study showed a high prevalence (37%) of infrequent stools in the exclusively breastfed population. Awareness of this condition was associated with a lower rate of intervention compared with mothers who were unaware of it. Our second study allowed us to better characterize the epidemiological and clinical features of infrequent stools. It occurred as early as 10 days and as late as 8 months of age; the median duration of an episode of infrequent stools was less than 1 week with a maximum of 4 weeks. The median duration of all combined episodes with infrequent stools was 2.5 months with a maximum of 8 months. It is not surprising that the more anxious mothers were more prone to intervene than the less anxious mothers.
Weaver et al. 2 showed that breastfed infants had a higher mean frequency of defecation than formula-fed infants at 2, 4, and 8 weeks of age; by 16 weeks, the mean frequency of bowel movements per day was two for infants of both feeding groups. Breastfed infants passed larger, softer stools than formula-fed infants until the introduction of complementary foods. In their description of the feces patterns of breastfed infants, Lawrence and Lawrence 6 pointed out that after 1 month of age, a breastfed infant should have at least one stool a day. If this does not happen, the healthcare provider should determine whether growth and urine output are adequate (i.e., six to eight wet diapers a day and at least one that is heavily soaked). Other sources focusing mainly on parents state that, at around 6 weeks of age, some infants cease having the several daily bowel movements expected up to this point. Some start stooling once a day, whereas others wait several days, and still others may have a week of stool-free days.
There are very few data on the prevalence and characteristics of infrequent stools. Moreover, the definition of infrequent stools varies among studies and the names being used for constipation or intestinal pseudo-obstruction or infrequent bowel movements. We were unable to identify any study assessing the prevalence of infrequent stools, however defined, in a population of healthy exclusively breastfed infants.
Aguirre et al. 7 observed in Sao Paulo, Brazil, a prevalence of 9% among predominantly breastfed infants <6 months of age. Constipation was characterized by necessarily hard stools and by the presence of at least one of the following features: painful stools or difficult stool passage, scybalous stools, cylindrical stools with cracks or thick cylindrical stools, or intervals between bowel movements ≥3 days.
Choe et al. 8 observed that out of 416 children attending their tertiary referral center in Seoul, South Korea, for constipation (defined as the absence of stools on 3 consecutive days) during a 1-year period, 28 (6.7%) were exclusively breastfed and had no organic abnormality. In this study, mean age at onset of constipation was 1.9 months (range, 0.5–3.5 months), and the condition spontaneously resolved at a mean age of 3.9 months (range, 1–7 months).
In some cases, the absence of defecation can last up to 4 weeks as in our study, or even longer (45 days) (G. Gremmo-Féger, Brest University Hospital, Brest, France, personal communication). Weaver et al. 2 described a breastfed infant who passed no stools for 27 days between 7 and 11 weeks of age. The infant remained visibly well, displayed no clinical signs of gastrointestinal or systemic disease, and passed a vast stool at the end of this period. She had only 14 bowel movements during the first 16 weeks of life. The pathophysiology of the condition remains unknown and unresolved.
Our studies have several strengths and weaknesses. The strengths include the high number of children in the prevalence study, the strict definition of exclusive breastfeeding, weight gain consistent with World Health Organization growth standards, and exclusion of infants with hard stools or stooling problems. However, the weaknesses include the arbitrary definition of infrequent stools, the study samples of infants who are not necessarily representative of the general population of breastfed infants, and recruitment bias from the Internet.
Conclusions
Because up to 37% of exclusively breastfed babies may pass infrequent stools, parents and health professionals should be aware of this possibility. As there are no established standards regarding defecation, the term “infrequent stools” seems the most appropriate. In most cases infrequent stools are very well tolerated, and parents and health professionals have only to monitor infant growth and development. Because the priority is to do no harm, it is of paramount importance to avoid unnecessary tests. As Eggermont 9 has pointed out, “the clinical evaluation of these patients is of paramount importance. As a rule, the infant is happy and thriving. Abdominal ballooning is exceptional and rarely causes crying and flatus. Neither abdominal palpation nor rectal examination reveals retention of excessive fecal material.” 9 Health professionals need to learn when to do nothing, while adopting a wait-and-see attitude and bearing in mind the possibility of Hirschsprung's disease developing with the onset of complementary feeding.
Footnotes
Disclosure Statement
No competing financial interests exist.