
Abstract
Abstract
Acinetobacter baumannii is a Gram-negative coccobacillus that has emerged as a troublesome pathogen causing institutional outbreaks. Environmental contamination is a distinctive characteristic of this microorganism, which brings a further difficulty in infection control. During A. baumannii outbreaks in intensive care units, a common contaminated object can be found as a reservoir. Finding out this source by epidemiological investigations is of particular importance in order to develop effective interventions. We describe an outbreak of A. baumannii and the results of epidemiological investigations in a neonatal intensive care unit. The outbreak strain was isolated from the outer surface of a breastmilk pump. We have successfully controlled the outbreak by careful reviewing of our milk collection process.
Introduction
C
Acinetobacter baumannii is a Gram-negative coccobacillus that has emerged as a troublesome pathogen causing institutional outbreaks. 4 This microorganism in particular constitutes a problem for critically ill patients.5–7 It can cause bloodstream infections, pneumonia, meningitis, and catheter and wound infections, which are difficult to treat because most strains are multidrug-resistant.6,7 A. baumannii also results in environmental contamination, which brings a further difficulty in infection control. 8 Outbreaks are difficult to control using standard methods, and there are documented cases of institutional outbreaks that have lasted several year. 9 Various environmental sources have been reported in the transmission of outbreak strains, including room humidifiers, air conditioning equipment, mattresses, pillows, curtains, hygroscopic bandages, and ventilation equipment.7,10–13 We describe an outbreak of A. baumannii and the results of epidemiological investigations in a neonatal intensive care unit. The outbreak strain was isolated from the outer surface of the breastmilk pump.
Case Report
Characteristics of the patients
In July 2009, a 2-day-old term neonate (Patient 1) with respiratory distress was referred from a rural hospital. He was on a mechanical ventilator. Blood culture showed A. baumannii, which was the first time that any Acinetobacter species has been isolated in our neonatal intensive care unit since its establishment in 1998.
Two days day later, blood culture of a premature infant (Patient 2) with respiratory distress syndrome showed the same microorganism with a similar antibiogram. According to the directions of the hospital infection control committee, control measures and surveillance studies were planned (Fig. 1). To investigate the source of the infection, as well as blood cultures, nasopharyngeal aspirates from the patients, environmental cultures, air samples, and hand cultures from the healthcare staff were obtained.
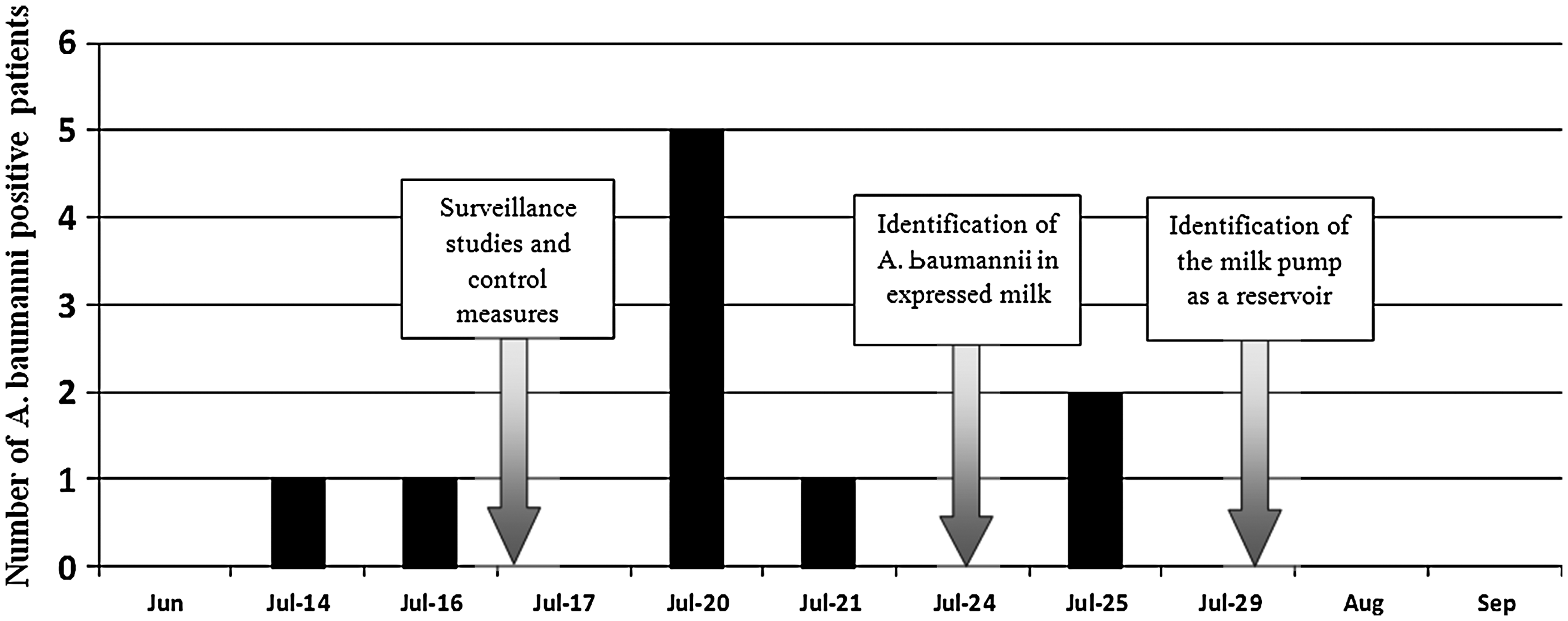
The timeline of the A. baumannii outbreak.
Microbiological studies and methods
Identification and susceptibility testing of Acinetobacter species were performed by the fully automated bacterial identification and antibiogram Phoenix™ kit (BD Diagnostic Systems, Sparks, MD) in the Medical Microbiology Laboratory. Susceptibility testing was carried out according to the manufacturer's specifications for this instrument and was performed in accordance with the methodology and breakpoints defined by the Clinical and Laboratory Standards Institute. 14 Multidrug-resistant A. baumannii isolates were defined as those resistant to more than three classes of antibiotics. 10 For tigecycline, minimal inhibitory concentrations were determined by the Etest® (bioMérieux, Marcy l'Etoile, France), and U.S. Food and Drug Administration susceptibility criteria were used. 15
Forty-five environmental cultures, including those from ventilators, incubators, floors, walls, an open bed, phones, keyboards, computer mouse, ultrasonography devices, sinks, desks, cabinets, and chairs, showed negative results for A. baumannii, whereas nasopharyngeal aspirates from Patients 3–7 were positive. The infection control team offered to review the formula preparation procedure. However, at that time, there were eight patients in the intensive care unit (Table 1), and all of them were being fed by expressed breastmilk. We decided to take cultures from expressed breastmilk, and, surprisingly, all but one showed positive results for A. baumanni. The negative culture belonged to a mother who had her own electric breast pump, and a culture from nasopharyngeal aspirate of her newborn was also negative (Patient 8). We then obtained a culture from the breastmilk pump, and this culture showed A. baumanni. All of the isolates had the same antibiotic susceptibility results and were considered to be a multidrug-resistant strain.
Not obtained.
PDA, patent ductus arteriosus; PPHT, persistent pulmonary hypertension; RDS, respiratory distress syndrome.
Pulse-field gel electrophoresis
Pulsed-field gel electrophoresis was performed for nasopharyngeal aspirates of the above-mentioned seven patients and isolates from the breastmilk pump, using a CHEF DR® III system (Bio-Rad, Hercules, CA). Chromosomal DNA was digested by the ApaI restriction enzyme, as described previously. 16 Pulsed-field gel electrophoresis profiles of the isolates were interpreted according to the criteria of Tenover et al., 17 and all of them were considered to be derived from a common ancestor.
Control measures
During this outbreak, our neonatal intensive care unit was providing Level 3 care with seven incubators and an open bed, and it was composed of just one room without any isolation unit. There was only one breastmilk pump in the service. This pump was also being kept in this room near the open bed. Patient 1 was followed up on this open bed. We noticed that the mother of this patient was expressing milk while she was touching her child.
The milk pump in our service is a hospital-grade pump, which is designed to be safe for multiple users. We were cleaning it daily with a surface disinfectant that is approved by the U.S. Environmental Protection Agency. The mothers were using disposable milk collection kits and were being informed about hand hygiene and handling of their kits; however, hand washing and milk expression practices were not being monitored.
After a positive culture from the pump was obtained, we have started to clean the electrical unit and the outer surface of the equipment after each individual use. Strict adherence to hand hygiene protocol was established. New milk collection kits were provided, and the mothers were informed about proper cleaning and storage of their kits after each use. We also obtained cultures from sterile packs of collection kits against the risk of contamination, which revealed negative results.
Mothers were examined for mastitis, but none had any sign of infection. Cultures were negative from nipples and manually expressed milk samples of the mothers. Baby bottles and lids were discarded, and the refrigerator was cleaned. Because there was no isolation room in our unit, we temporarily transferred the newborns into an available patient room for a few days. Terminal disinfection of the unit was carried out with sodium hypochlorite.
Three patients with positive blood cultures were considered as having infections and were treated with high-dose sulbactam, ampicillin, and meropenem. The other patients were considered as having colonization and managed with close monitoring for infection. One newborn with pulmonary hypoplasia (Patient 7) died because of respiratory failure in the first week of his life; others successfully recovered.
Discussion
Hospital-grade breastmilk pumps are designed to operate in a closed system so that they can be used by more than one mother with their own milk collection kits.18,19 The collection kit should be sterile before each use, and using disposable collection kits enables prevention of cross-infection between different mothers.2,20 In most hospitals mothers are initially given their own kits and the kit is discarded when the infant leaves the hospital.18,20
There is also risk of bacterial contamination of the milk, when a kit is undergoing repeated use by the same mother.2,18,20,21 Because it is not feasible to discard the material each time, proper reprocessing of a disposable kit is a critical step for infection control in neonatal intensive care units. Disinfection of the items after each use can be provided by means of autoclaving, steam-producing devices, or chlorine-releasing agents. 20 However, there are certain drawbacks about safety and practicality of these methods. According to Gilks et al., 2 the most applicable method is thorough washing, rinsing, and drying. After each use, breast pump kits should be dismantled into separate parts, and the equipment parts that have come into contact with the breast and milk should be rinsed in cold water after a warm water detergent wash. Subsequent drying by paper towels or by allowing the items to dry in air is also of vital importance in order to prevent bacterial overgrowth in moist areas. Proper storage in a container with access to air would enable evaporization of the remaining moisture, and labeling is required because mixing up the kits would result in cross-infection. 2
We do not know the exact source of this organism; however, seeing that the blood culture of Patient 1 was the first time that any Acinetobacter species has been isolated in our neonatal intensive care unit and that the mother of this patient was expressing milk while she was touching her child, we speculate that this mother might be responsible from contamination of the pump. During the outbreak, we found out several deficiencies regarding our milk collection process. One of the main problems was keeping the pump within the intensive care unit because of physical limitations. After this outbreak, our intensive care unit was moved to a new hospital building in which the breastmilk pump was kept in a separate room.
Our second intervention was assigning a nurse to be responsible for monitoring the milk collection process. In neonatal intensive care units, social characteristics and the educational level of the population dealt with may vary, and the compliance of mothers may be suboptimal. We have seen that continuous guidance during hand washing, the pumping session, and reprocessing of the kits is critical. Mothers were supported to clean their kits effectively and taught to store and label them properly. Labeling of the milk bottles and placing them in the refrigerator are also essential steps to be monitored.
And lastly, because the electrical unit and the battery are not autoclavable, proper cleaning of the outer surface is of pivotal importance. If hand hygiene is suboptimal, the pump can easily be contaminated on the operating rate and cycle buttons. Cleaning of the pump machine after each use is provided.
Unlike most other Gram-negative bacteria, Acinetobacter species can survive in a dry environment for long periods of time. 7 It is well documented that the mean survival time of outbreak strains of A. baumanni on a dry surface is almost 1 month. 22 This ability gives two distinctive epidemiologic behaviors to this microorganism: environmental contamination and resistance to desiccation, which prolongs the outbreaks.5,7 During A. baumanni outbreaks in intensive care units, a common contaminated object can be found as a reservoir.10–13 Finding out this source by epidemiological investigations is of particular importance in order to develop effective interventions.
Conclusions
Physicians should be aware that breastmilk pumps can serve as reservoirs during A. baumannii outbreaks. Adherence to hand hygiene, monitoring of milk collection session, proper reprocessing of the collection kits, and cleaning the equipment after each use are critical steps for preventing outbreaks in neonatal intensive care units.
Footnotes
Disclosure Statement
No competing financial interests exist.