
Abstract
Abstract
Background:
Although human milk (HM) is the recommended form of infant nutrition, the provision of HM feeding among infants with congenital heart disease in the cardiac intensive care unit is unknown. Therefore the aim of the study was to understand the prevalence of pumping initiation, HM feeding, and breastfeeding patterns of mothers and their infants born with congenital heart disease.
Subjects and Methods:
This was a prospective cohort study conducted a large children's hospital with a cardiac referral program and unit. All women with infants with congenital heart disease were approached for enrollment in order to document HM prevalence.
Results:
The majority of women (89%) initiated lactation via pumping for their infants. On average, mothers pumped five to six times per day, and mothers were able to achieve a milk supply of over 500 mL/day. Once infants received enteral feeds, over 70% of the infant diet was HM. Very few (13%) infants fed via direct breastfeedings; rather, they received HM via gavage or bottle. There was a significant difference in pumping initiation based on where the infant was born, with mothers delivering in the hospital having a significantly higher pumping initiation rate (96% born in this hospital, 67% born in an outside hospital).
Conclusions:
Mothers who have infants diagnosed with congenital heart disease should be encouraged to initiate pumping for their infants. Future research is warranted regarding the dose response of HM and specific health outcomes and the need for postdischarge services for these families.
Introduction
I
Understanding the lactation initiation and maintenance patterns of mothers of infants with CHD is of upmost importance. A diet of exclusive HM provides many benefits to the infant, including a reduced risk of infection and of developing necrotizing enterocolitis and a shortened length of stay in the hospital.5,6 Necrotizing enterocolitis among term neonates is rare (10–15% of reported cases occur in the term infant); the incidence of necrotizing enterocolitis among infants with CHD is cited to range between 1.62% to 7.8%.7–10
Subjects and Methods
Design
The study design was a prospective cohort study of all infants born or diagnosed with CHD and admitted to the CICU during the neonatal period at the Children's Hospital of Philadelphia (CHOP), Philadelphia, PA. Based on historical data, over 200 infants are admitted to the CHOP CICU each year. The institutional review board at CHOP approved the study protocol and informed consent documents. Following Institutional Review Board approval, mother–infant dyads were screened over a 12-month period. Inclusion criteria included all infants less than 6 months of age admitted to the CICU. Exclusion criteria included (1) human immunodeficiency virus–positive mothers, (2) mothers with a positive history of using a level 5 medication, 11 and (3) non–English-speaking mothers because of the study methodologies (fewer than 20% of all admissions). All mothers, regardless of pumping/breastfeeding intention, were enrolled in order to capture the prevalence of pumping/breastfeeding initiation.
Procedures
The researchers reviewed the admission log in the CICU every other day. When a new infant was admitted, the mother's chart was reviewed for eligibility into the study. The researchers approached all eligible mothers between 48 hours and 7 days of the infant's admission to introduce the study to the dyad. Following confirmation of the eligibility criteria, written informed consent was obtained.
Following enrollment, one of the study team's lactation research assistants (L.R.A.) met with the mother to review the necessary instructions to complete the maternal milk log book. The standard of care at CHOP includes encouragement of all breastfeeding and/or pumping mothers to keep the same log book that the researchers used in this study. Breastfeeding sessions were also documented in the log book. The pumping log has been extensively used at CHOP in order to monitor mothers' pumping patterns and milk volumes (in mL). The LRA met with mothers twice a week to ensure pump log accuracy and completeness in filling in the maternal milk log book. The information obtained from the maternal milk log book was used by the research team to capture and describe the daily milk volumes of each participant.
To document the provision of HM for the infants with CHD, a member of the research team collected daily infant feeding data. For each day of the infant's hospital stay, a member of the research team extracted information from the infant's bedside flow sheet (Table 1). From these data, the researchers were able to determine the percentages of HM provision for each infant during each day of the hospital stay and the mode in which the milk was delivered (breast, bottle, or gavage). The data were entered into an Excel® (Microsoft, Redmond, WA) workbook and stored on a password-protected computer on the hospital's secure network.
Measures
Demographics
Infant and maternal demographics were collected on all subjects upon enrollment into the study. For nonpumping or nonbreastfeeding mothers, study participation ended upon completion of demographics.
Pumping initiation
Data on the mother's plan to breastfeed, initiate pumping, or use formula were obtained from the nursing flow sheet at admission.
Milk supply
All pumping mothers were provided with a maternal milk log book and requested to record the date, time, and volume of milk expressed for their entire breastfeeding and/or pumping duration. Photocopies of the maternal milk log books were made weekly.
Infants' dose, exposure, and feeding method
Data on the provision of HM are detailed on all infants' records during hospitalization. Data on the dose and exposure of HM feeding were collected via chart review.
Dose was treated as the overall percentage of HM feeds recorded per feed. For gavage and bottle feeds, dose was recorded using the documented milliliter volume of the feed(s). For direct breastfeeding sessions, pre- and post-HM feeding weights were used. 12 If pre- and post-HM feeding weights were completed, the amount of milk transfer (in g) was documented on the bedside flow sheet.
Exposure was treated as the daily exposure of the infant to HM. Each day, exposure was recorded on a yes or no basis using the following format: (1) Did the infant receive any feedings today? (2) Of those feedings, what percentage was HM?
Feeding method was determined by the percentage of infants' feeds received by gavage, bottle feeding, or breastfeeding. All data were obtained from the cardiac center nursing flow charts.
Data analysis
Descriptive analysis was conducted for baseline characteristics, demographics, pumping initiation, milk supply, and infants' dose and exposure to HM and are presented as mean±SD or as median with interquartile range for continuous variables and as percentage for categorical variable (e.g., gender and mothers' success with pumping initiation). Mean milk volumes were calculated weekly during the cardiac center stay as well as mean number of pumpings per day and mean daily milk production (in mL) to allow for examination of variation of milk production in individual mothers over time. Mean daily milk volumes were compared with published average milk volumes for healthy term breastfeeding dyads. Exposure to HM was determined over the course of the infant's hospitalization.
Results
In total, 138 mothers were eligible and 62 mothers agreed to participate in the study (Fig. 1). Table 2 presents baseline sociodemographic characteristics of the mothers. The mothers classified themselves as predominately white (48%), with the majority of mothers having a college degree (47%) or higher (15%). The majority of mothers were multiparas (61%); primiparity accounted for 39% of mothers. Maternal gravidy was equally distributed between one (34%) and two (34%) pregnancies. An approximate equal distribution was also found between prior breastfeeding (48%) and no breastfeeding (52%) experience. Almost all mothers (85%) received a lactation consult during the infant's hospitalization period.
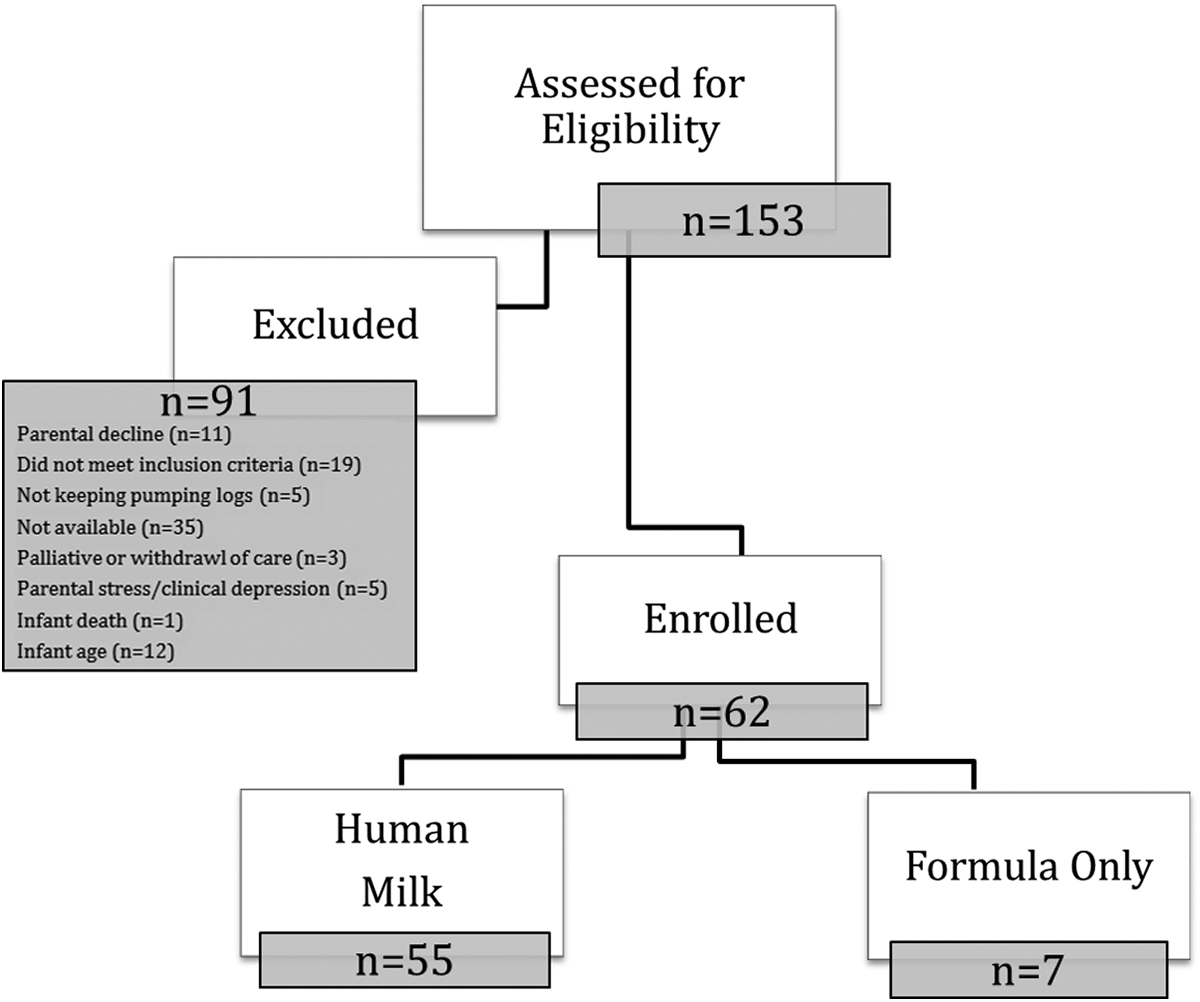
Study recruitment flowchart.
Most of the infants in the study sample (76%) were delivered in the Special Delivery Unit (SDU) within CHOP. The SDU is a delivery unit designed to care for mother and baby dyads when the baby has a known congenital anomaly. Of the total sample (n=62), all but seven infants carried a prenatal diagnosis. Mean gestational age was 38.54 weeks (SD=1.54 weeks) with a mean birth weight of 3,270 g (SD=648.27 g). Gender was approximately equal, with 32 males (52%) and 30 females (48%). Infant diagnoses are presented in Table 3. The most common diagnoses were hypoplastic left heart syndrome and transposition of the great arteries, accounting for 26% of the sample, followed by an equal distribution between transposition of the great arteries with an intact ventricular septum and tetralogy of Falot, representing 20% of the sample. The remainder of the sample consisted of various congenital heart defects.
Maternal pumping initiation and pumping pattern(s)
Of 62 maternal participants, 89% (n=55) of mothers planned to pump or breastfeed, and seven mothers planned to use formula (11%). For those mothers deciding to breastfeed and/or pump, a significant relationship was found between mothers delivering in the SDU and mothers pumping (p<0.0001) as well as mothers initiating pumping on the day of delivery (p=0.0071). In regard to initiation of pumping, 96% of the women who delivered in the CHOP SDU initiated lactation via pumping compared with 67% of the women who delivered at outside hospitals. Three mothers were excluded from the analysis: one infant died, and two mothers did not respond to calls from the researchers to copy maternal milk log books logs. Thus there were pumping and/or breastfeeding data for 52 mothers for the pumping data analysis.
Most mothers (75%) initiated pumping on the date of delivery. Mothers who delivered in the CHOP SDU initiated lactation using the Medela (McHenry, IL) Symphony breast pump, Preemie+® Pattern. The Preemie+ Pattern is a breast pump suction pattern designed for initiation of lactation. Meier et al. 13 tested this pattern with mothers of preterm infants and found that the pattern more effectively removed colostrum and helped mothers “come to volume” quicker compared with a standard breast pump suction pattern. In this study, all of the mothers delivered term infants; therefore our research adds data to demonstrate the effectiveness of this pattern for initiating lactation for all mothers who are separated from their infants (not solely mothers of preterm infants). On average, mothers pumped between five and six times per day (a 24-hour period) (Fig. 2). Maternal milk volumes approached 500 mL within the first week of pumping (Fig. 3).
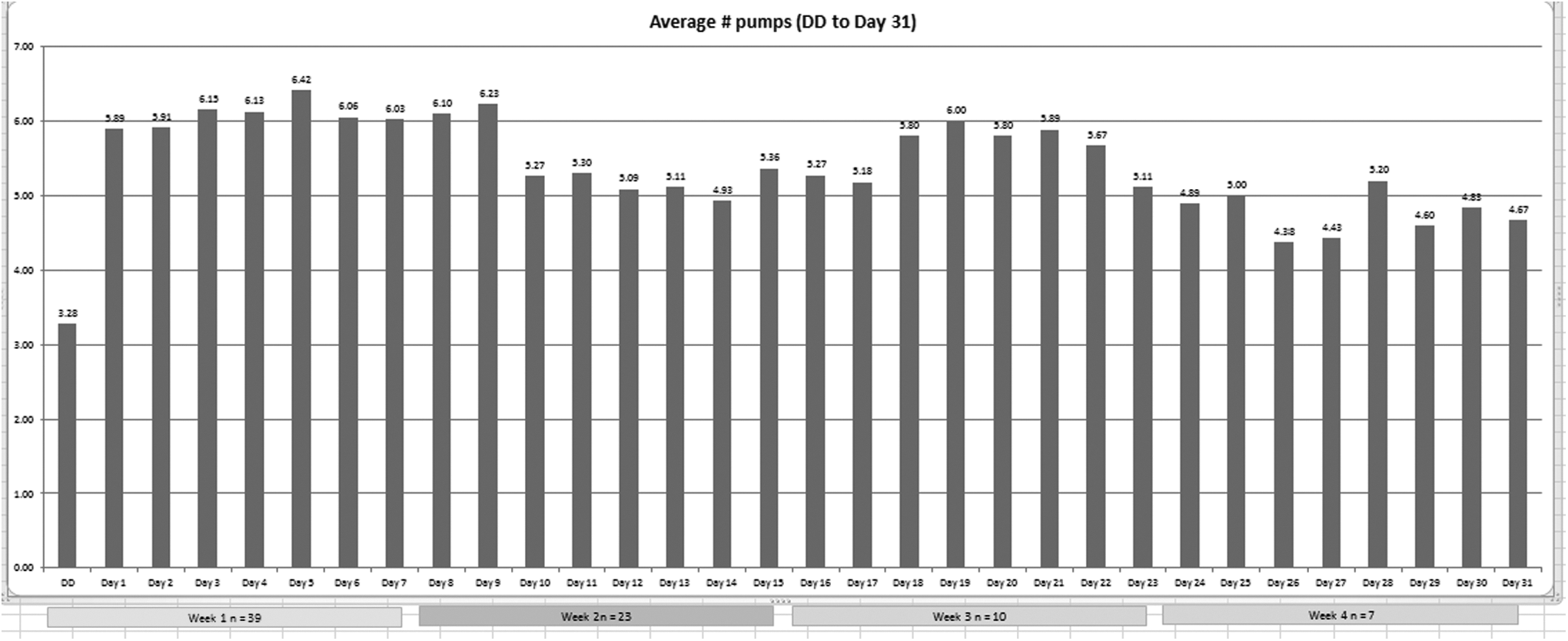
Average number of pumping sessions per day. DD, delivery day.
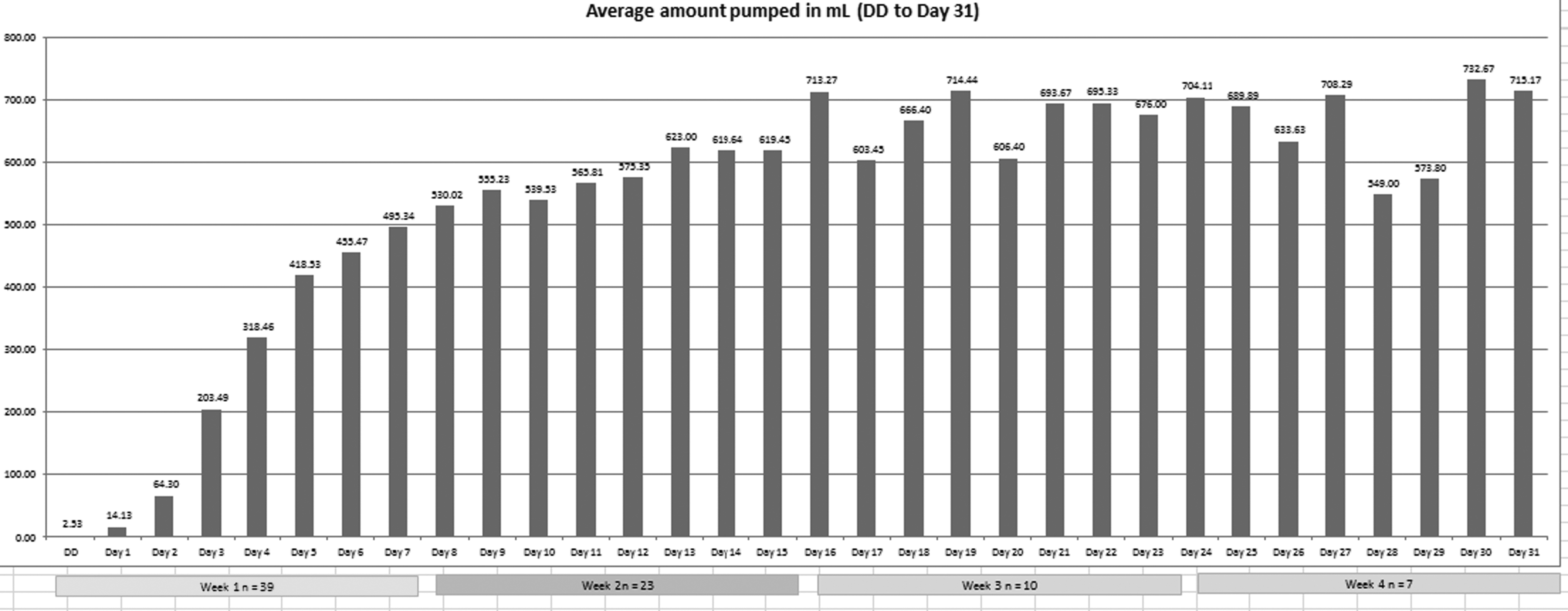
Average daily milk volume (in mL). DD, delivery day.
Infant dose and exposure to HM and method of feeding delivery
Infant feeding data were only collected on those infants who were receiving HM feedings. We examined the overall amount of HM received during the hospital stay as well as the route in which the feeds were introduced. The mean percentage of HM received per infant per day was 53.6% (n=55; SD=0.255; median, 0.536; lower quartile, 0.436; upper quartile, 0.717). Furthermore, 51.7% (SD=0.32) of all feeds were delivered via bottle, and 20.2% (SD=0.26) via gavage. Only 10.6% (SD=0.17) of all feeds were received via direct breastfeeding.
Many of the infants in the study spent several days on nothing per mouth status, meaning nil per os or that no HM or artificial nutrition was given to the infant on that day. Therefore, when the days spent nothing per mouth were removed from the analysis, the exposure to HM increased. The mean percentage of HM received per infant per day was 70.2% (n=53; SD=0.265; median, 0.7519; lower quartile, 0.546; upper quartile, 0.892). The routes of infant feeding also varied slightly: feeds via bottle, 63.3% (SD=0.36); via gavage, 30.5% (SD=0.389); and via direct breastfeeding, 13% (SD=0.211) (Fig. 4).
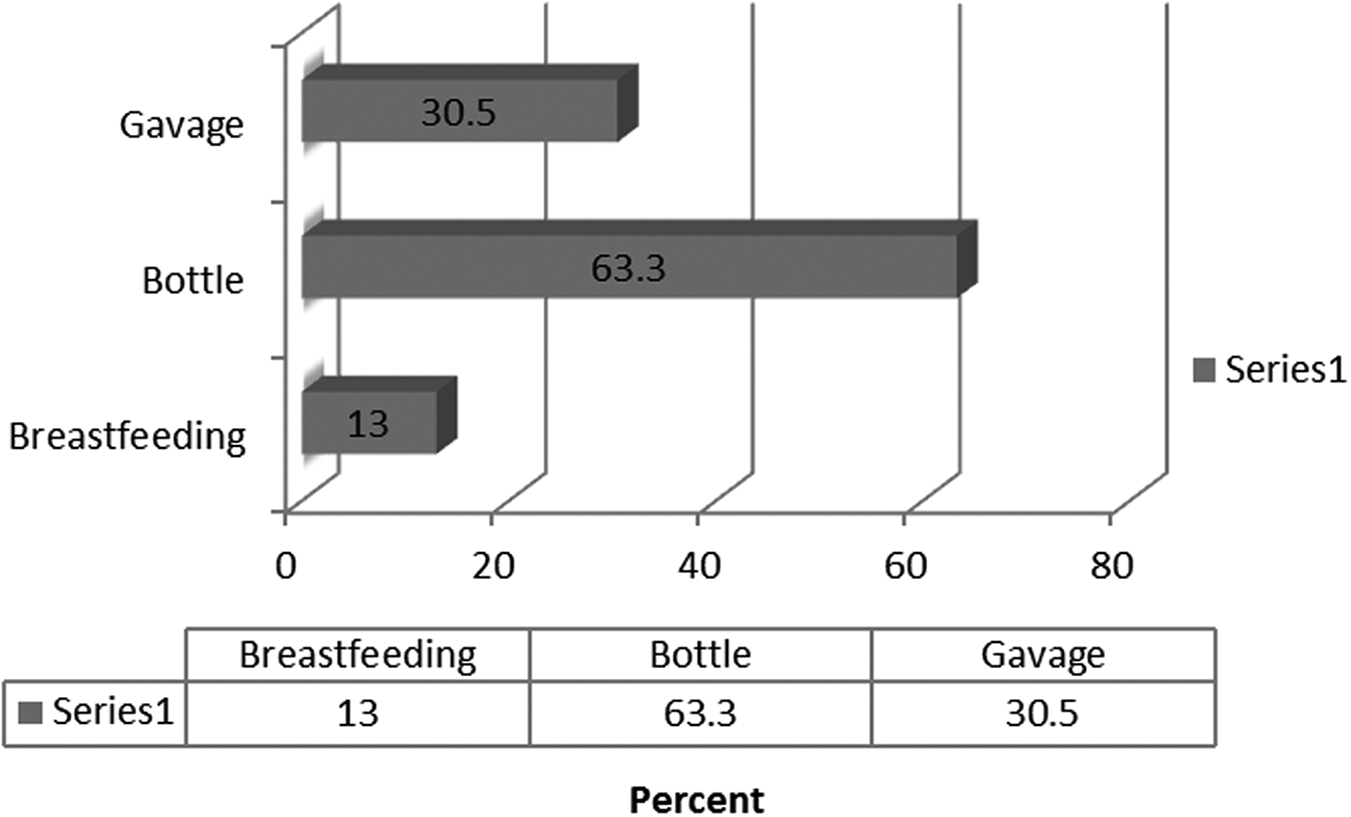
Percentage of feedings delivered by breastfeeding, bottle feeding, or gavage.
Discussion
One of the most important findings of this study is the role of institutional culture and informed decision on breastfeeding/pumping initiation. Mothers delivering in the CHOP SDU were significantly more likely to initiate pumping for their infant than mothers who delivered at outside hospitals (96% and 67%, respectively). Within CHOP, all mothers with a prenatal CHD diagnosis receive a prenatal lactation consultation focusing on the provision of HM (even if the mother had not intended on breastfeeding and/or pumping), resulting in virtually all mothers initiating lactation for their infants.
Anecdotally, many healthcare professionals hold beliefs that when infants are born critically ill, hospitalized mothers will be unsuccessful at maintaining lactation and/or breastfeeding. The research study sample clearly demonstrates that mothers who have infants with complex CHD are able to successfully initiate lactation, pump adequately, and come to volume (i.e., achieve milk supply reflective of mothers with healthy infants). Initiation and maintenance of milk supply are of paramount importance for mothers to achieve exclusive breastfeeding/provision of HM during the first 6 months of the infant's life (as recommended by the American Academy of Pediatrics). 4
Of particular concern is many infants with complex CHD have a relatively short length of stay, with the majority of them being discharged at ≤14 days. So even though the mothers were able to achieve a full milk supply, many infants were not directly feeding at the breast during the hospitalization period.
Limitations
There were several limitations to the study. The CICU is a research-intensive environment, with multiple research staff attempting to approach and consent parents within 72 hours of admission. Timing of surgical procedures in the neonatal period was variable and limited the research team's ability to respectfully access the parents in the preoperative period, especially in cases where infants who went to surgery within 48 hours of admission.
Almost all infants enrolled in the study were born with complex CHD. Having a newborn with CHD is overwhelming to parents, and the immediate postoperative period is a particularly stressful time. 14 Furthermore, infants with CHD may have associated comorbidities and increased risk for hemodynamic instability that posed additional challenges in the research team's ability to enroll subjects and copy maternal pumping logs. Mothers who had infants with poor prognoses (palliative care/extracorporeal membrane oxygenation support) or early mortality were a challenge.
The research team's ability to consistently collect accurate infant feeding data was also a limitation. Pre- and post-HM feeding weights (to measure milk transfer for direct breastfeeding) were not consistently documented, particularly among the hemodynamically stable infants. For example, two of the infants receiving HM did not have data available to include in the analysis of the percentage of HM feedings per day as milk transfer was not documented. In some cases, breastfeeding sessions were documented as “BF×1” versus actual documentation of milk transfer. Pre- and post-HM feeding weights were more consistently documented among hemodynamically unstable infants or those at risk for instability. Furthermore, if two signatures were not documented next to the feeding (co-signatures are required by two healthcare providers prior to the administration of HM enteral feeds per the hospital policy), or the enteral feeding documentation did not have the identifier “human milk” or “maternal breastmilk,” it was not recorded by the research team as such. Therefore, the prevalence of HM feedings may be underrepresented in the study findings.
Lastly, at the start of the study, feeding documentation was completed on a bedside paper flow sheet. Mid-enrollment, documentation transitioned to an electronic health record, creating a learning curve for nurses and the research team in both documentation and interpretation of feeding data. Maternal data collection was less challenging, with only a few mothers who did not maintain pump logs.
Conclusions
Implications
In the case of CHD, the periods of diagnosis and prognosis are of upmost importance. During the initial period before the birth of the infant and directly following the delivery, it is paramount to focus attention on the mother if she has made a decision to provide HM as the primary form of infant nutrition. The period of time following the birth of the CHD infant is very stressful for the mother and family. 2 However, support (including direct and continued follow-up on pumping and milk supply, provision of needed resources, and referral to one of the hospital's International Board Certified Lactation Consultants, if needed) from providers and clinicians will facilitate a mother establishing her milk supply. The study has demonstrated that women who deliver within CHOP and mothers of CHD infants transported to CHOP from outside hospitals can initiate and maintain milk supply during the period of their infants' hospital stay in the CICU.
Additionally, although it was not a large percentage of the study sample, many women were able to transition from breast pumping to direct breastfeeding prior to discharge from the CICU. If a mother has an intention or goal to eventually feed her infant directly from the breast, then the clinician needs to be cognizant of the mother's milk supply throughout the hospitalization period. The maternal milk supply needs to be at a level to provide the needed volume for the infant's daily feeds.
In moving forward, the study team recognizes the need to consider alternative forms for cataloging or tracking maternal milk supply. Some mothers in the study preferred to use applications over the paper log book. Hospitals and other care institutions should consider these technologies and discuss with the mother which means she finds most efficient.
It is important to acknowledge CHOP's established breastfeeding and HM culture within the hospital. CHOP values the provision of HM for infants less than 1 year of age, and this is evident through the availability of resources (breast pumps, pumping kits, scales for pre- and postfeeding weights, maternal milk log books, nipple shields, storage containers, and labels), facilities (refrigerators, freezers, and the Human Milk Management Center), and support (2 PhD-prepared nurse researchers as manager and supervisor of the lactation program, 4 International Board Certified Lactation Consultants, and Breastfeeding Resource Nurses at the point of care). The majority of women in the study sample were successful in coming to full milk volume because of their diligence and dedication to pumping and the established support frameworks of the institution.
Potential for new research directions
The study is a novel study that brings to light the potential for new research on the role of HM and breastfeeding in infants with CHD. Future research should focus on the dose-dependent relationships of HM on health outcomes, including but not limited to infection (gastrointestinal, necrotizing enterocolitis, respiratory, otitis media), length of stay, and hospital re-admission.
The study demonstrates mothers of CHD infants are able to initiate lactation and come to volume; however, additional research should focus on the time period postdischarge. Research should explore models of postdischarge support to enable mothers of CHD infants to sustain milk production, potentially to transition to direct breastfeeds, and to optimize the infant's exposure to HM while maintaining optimal growth.
Footnotes
Acknowledgments
The survey of the study was supported by the Center for Pediatric Nursing Research and Evidenced Based Practice, National Association of Pediatric Nurse Practitioners.
Disclosure Statement
No competing financial interests exist.
D.L.T., the co-Principal Investigator of record, participated in the conceptualization and design of the study, coordinated and supervised data collection, recruited and enrolled participants, drafted the methods and results sections of the manuscript, and is responsible for the review of the manuscript drafts rand for revisions to the manuscript. A.S. participated in conceptualization and design of the study, facilitated data collection, recruited and enrolled participants, participated in drafting the discussion and conclusion sections of the manuscript, and is responsible for review of manuscript drafts. E.B.F. participated in the conceptualization and design of the study, collected infant feeding data, organized participant data via database management, drafted the introduction, methods, and results sections of the manuscript, and is responsible for the review of manuscript drafts and for the revisions to the manuscript. D.L.S., the co-Principal Investigator of record, participated in the conceptualization and design of the study, recruited and enrolled participants, coordinated and supervised data collection, drafted the introduction, conclusions, and abstract sections of the manuscript, and is responsible for the review of manuscript drafts and for the revisions to the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.