
Abstract
Abstract
Although the American Academy of Pediatrics and the American Congress of Obstetricians and Gynecologists (ACOG) recommend exclusive breastfeeding for the first 6 months, only 14.6% of babies born in the District of Columbia (DC) reached this goal. Breastfeeding support from providers has been shown to increase exclusive breastfeeding. We aim (1) to describe breastfeeding knowledge and attitudes, (2) to determine the presence of breastfeeding in routine prenatal discussions, and (3) to determine the knowledge of facility adoption of the Perinatal Care (PC) Core Measure Set among DC ACOG members. A survey sent to DC ACOG members assessed knowledge, attitudes, and practices related to breastfeeding and evaluated participants' barriers to breastfeeding counseling, management of breastfeeding challenges, and awareness of facility adoption of the PC Core Measure Set. All 29 respondents reported breastfeeding as the best infant nutrition and that physicians should encourage breastfeeding. However, despite 75% reporting counseling most of their patients regarding breastfeeding, only 27% reported that most of their patients were breastfeeding at the postpartum visit. Participants scored 83% correct on knowledge-based questions. Perceived barriers to breastfeeding counseling included lack of time (66%), reimbursement (10%), and competence in managing breastfeeding problems (7%). Most respondents were unsure of both adoption of, and breastfeeding data collection for, the PC Core Measure Set (52% and 55%, respectively). Participants had knowledge gaps and identified barriers to discussing breastfeeding. There was limited awareness of hospital data collection about breastfeeding. These results indicate a need for more breastfeeding education among DC obstetricians-gynecologists and better outreach about the PC Core Measure Set.
Introduction
A
Despite improvements nationally, DC has continued to fall short of the Healthy People 2020 Breastfeeding Objectives of having 25.5% of infants exclusively breastfeed for 6 months. 4 Although the American Academy of Pediatrics and the American Congress of Obstetricians and Gynecologists (ACOG) strongly recommend exclusive breastfeeding for the first 6 months, only 14.8% and 14.6% of babies born in DC reached this goal in 2012 and 2013, respectively.5,6
In 2010, the Joint Commission introduced an evidence-based Perinatal Care (PC) Core Measure Set. This replaced the prior Pregnancy and Related Conditions Measure Set with expanded evidence-based objectives for institution data collection. This measure set prioritizes gathering information on the following: (1) elective delivery, (2) cesarean section, (3) antenatal steroids, (4) healthcare-associated bloodstream infections in newborns, and (5) exclusive breastmilk feeding during the birth hospital stay. 7 There is a paucity of literature regarding whether obstetricians are aware of this core measure or if their primary hospital has adopted it.
Research has shown that educating physicians about breastfeeding not only increases their knowledge but also improves their patients' breastfeeding rates. 8 However, there is a paucity of literature describing the knowledge, attitudes, and practices of obstetricians and gynecologists around breastfeeding. Studies from Freed et al. 9 and Howard et al. 10 revealed deficits in knowledge and formal training around infant feeding among obstetricians but may not reflect current attitudes and practices. Recent work from Demirci et al. 11 analyzed audio recordings of obstetrician visits for breastfeeding content and found that discussions on breastfeeding were both infrequent and, when they did happen, brief. Given that obstetricians have frequent prenatal contact with patients, they have a significant opportunity to discuss breastfeeding.
The purpose of this study is to better understand practicing members of the DC Section of ACOG's knowledge, attitudes, and reported counseling about breastfeeding. Given the role of the obstetrician in many of the indicators for the Joint Commission's PC Core Measure Set, an additional objective was to determine the proportion of survey participants who were aware of this hospital data collection quality measure set.
Materials and Methods
After Institutional Review Board approval was obtained through the Children's National Health System, Washington, DC, a 33-question electronic survey (the questionnaire is available by request from the authors) was developed and sent to members of the DC Section of ACOG Listserv using Research Electronic Data Capture (REDCap). A link to the survey was sent to members of the Section in December 2011 requesting responses be submitted by February 2012. With permission, we adapted an already modified version of the Breastfeeding Attitudes and Knowledge of Pediatricians-in-Training questionnaire originally created by Williams and Hammer 12 for use with our obstetric colleagues. An information sheet explaining the project and its associated risks was attached; answers were anonymous, participation was voluntary, and therefore completion of the survey implied consent. There were 100 members of the DC chapter of ACOG at the time of this survey, 86 of whom were actively practicing at the time of this survey. There are eight birthing facilities in Washington, DC with variable breastfeeding support. In order to maintain confidentiality, we did not ask respondents to indicate their institution.
Inclusion criteria comprised active members of the DC Section of ACOG who were currently practicing or in training. Fourteen DC ACOG members who were no longer practicing were excluded.
Participants were assessed on (1) basic knowledge about breastfeeding and ability to manage breastfeeding problems, (2) attitudes around breastfeeding, and (3) professional practices related to breastfeeding. In addition to demographic information, survey participants were also queried about their personal experience with breastfeeding their own children, if applicable. Questions were in “true or false” and multiple choice formats.
In total, 14 knowledge-based questions about breastfeeding were asked. Question topics included management of common breastfeeding problems (such as sore nipples, mastitis, or thrush) and contraindications to breastfeeding, including medication and maternal lifestyle (such as smoking status), as well as institutional and individual factors that inhibit successful breastfeeding.
In order to understand the professional practices of participating obstetrician-gynecologists, we asked the participants to estimate the frequency of their breastfeeding counseling during the month prior to the survey, as well as the percentage of their patients who were breastfeeding at the 6-week postpartum visit.
We also investigated barriers to both (1) discussing breastfeeding with patients and (2) exclusive breastfeeding of infants in the hospital. Lastly, the participants were asked about their knowledge of their facility's adoption of the Joint Commission's 2010 PC Core Measure Set.
Results
Demographics
There were, in total, 29 survey respondents out of the 86 practicing physicians (34% response rate). The respondents included residents (17%), fellows (17%), and practicing physicians (66%); 83% were women, and 17% were men. Over half (55%) were between 30 and 40 years old, and 28% were between 50 and 60 years old. Fifty-two percent of respondents were parents.
Knowledge
The average overall score for knowledge-based questions among participants was 83%. All participants were able to correctly identify that:
• breastfeeding is better for babies than formula feeding, • estrogen-containing oral contraceptive pills can affect lactation, and • breastfeeding should be initiated in the first hour after delivery for healthy term infants.
Other questions with high percentages of correct responses included:
• management of mastitis, particularly that milk does not need to be discarded (97% correct), and • improper positioning as the most common cause of sore nipples in a breastfeeding mother (93% correct).
The largest knowledge deficits involved management of a breastfeeding mom whose infant has thrush (i.e., correctly identifying that an asymptomatic mother need not be treated) (48% correct), prevention of early jaundice with frequent breastfeeding (48% correct), and that an artificial nipple should not be introduced until lactation is well established (62% correct) (Fig. 1).
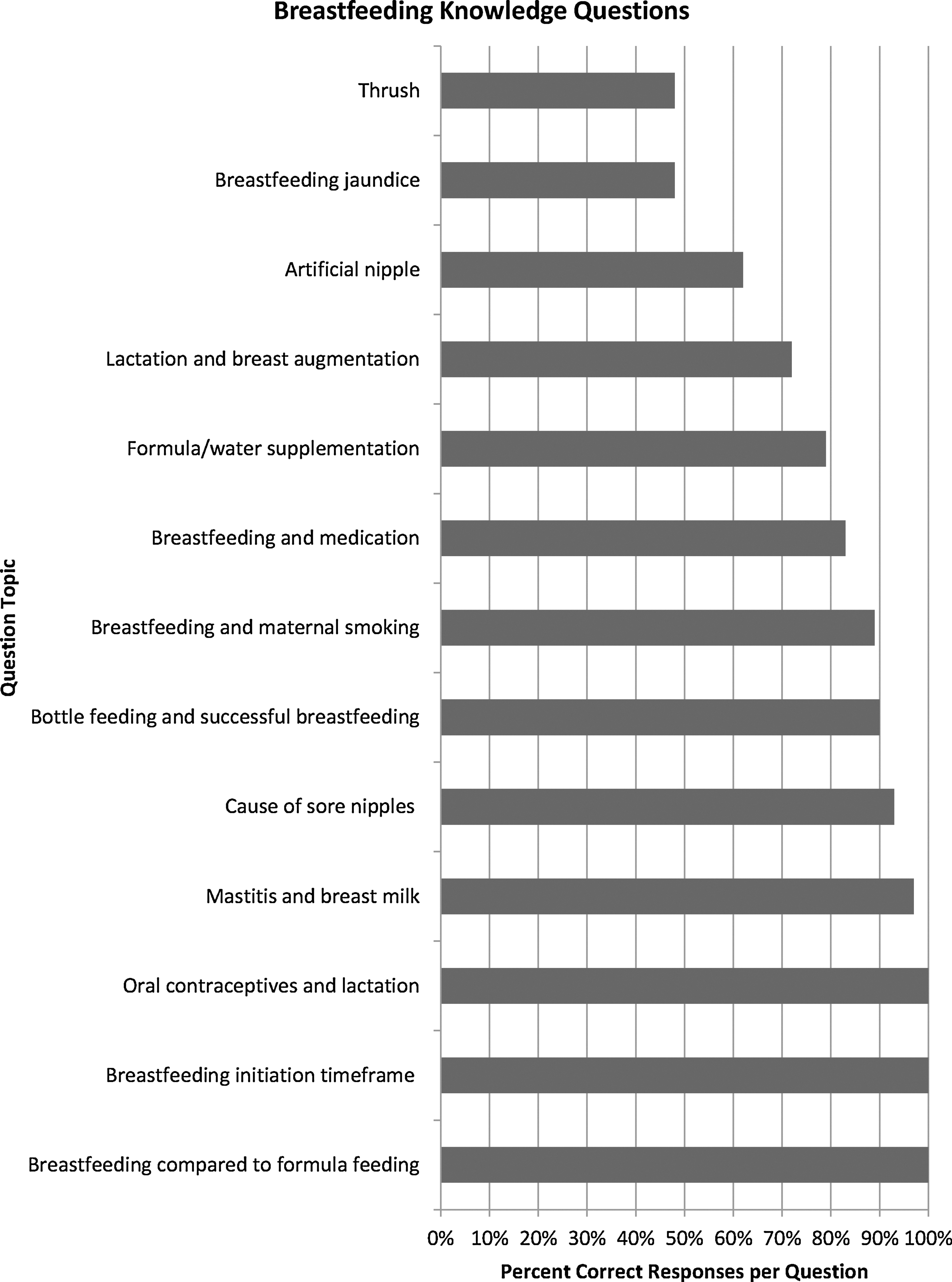
Breastfeeding knowledge questions.
Attitude
Respondents had an overwhelmingly positive attitude with regard to breastfeeding. All respondents felt that breastfeeding was better for babies than formula feeding and that physicians should strongly encourage mothers to breastfeed. Those surveyed were asked who is responsible for educating patients about lactation. Respondents were allowed to choose multiple answers: “obstetrician” and “OB nurse” were each chosen by 97% of respondents. Twenty-six respondents (90%) felt that this responsibility also belonged to the pediatrician.
Professional practices
All respondents reported that they routinely ask their antenatal patients how they plan to feed their infant. When asked to estimate the percentage of patients they counseled regarding breastfeeding in the past month, 18 respondents (75%) said that they counseled between 75% and 100% of their patients. However, only six responding physicians (27.3%) said that between 75% and 100% of their patients were still breastfeeding at the 6-week postpartum visit.
Personal practices
Fifty-two percent of our respondents were parents; 36% of their children were breastfed, and only 40% of these breastfed children were breastfed for 6 months or longer.
Management of breastfeeding challenges
Confidence level for managing breastfeeding challenges was assessed by responders' self-rating on a 4-point Likert scale (1=not very confident; 2=fairly confident; 3=confident; 4=very confident). Twenty-four percent felt very confident, 31% confident, 35% fairly confident, and 10% not very confident managing breastfeeding challenges.
Barriers
Respondents could choose multiple answers for barriers to (1) discussing breastfeeding with their patients (Fig. 2) and (2) successful breastfeeding within their institution (Fig. 3). The most commonly reported barriers for discussing breastfeeding included not enough time (65% of respondents), parent not interested (41%), not reimbursable (10%), and not competent in managing breastfeeding issues (7%).
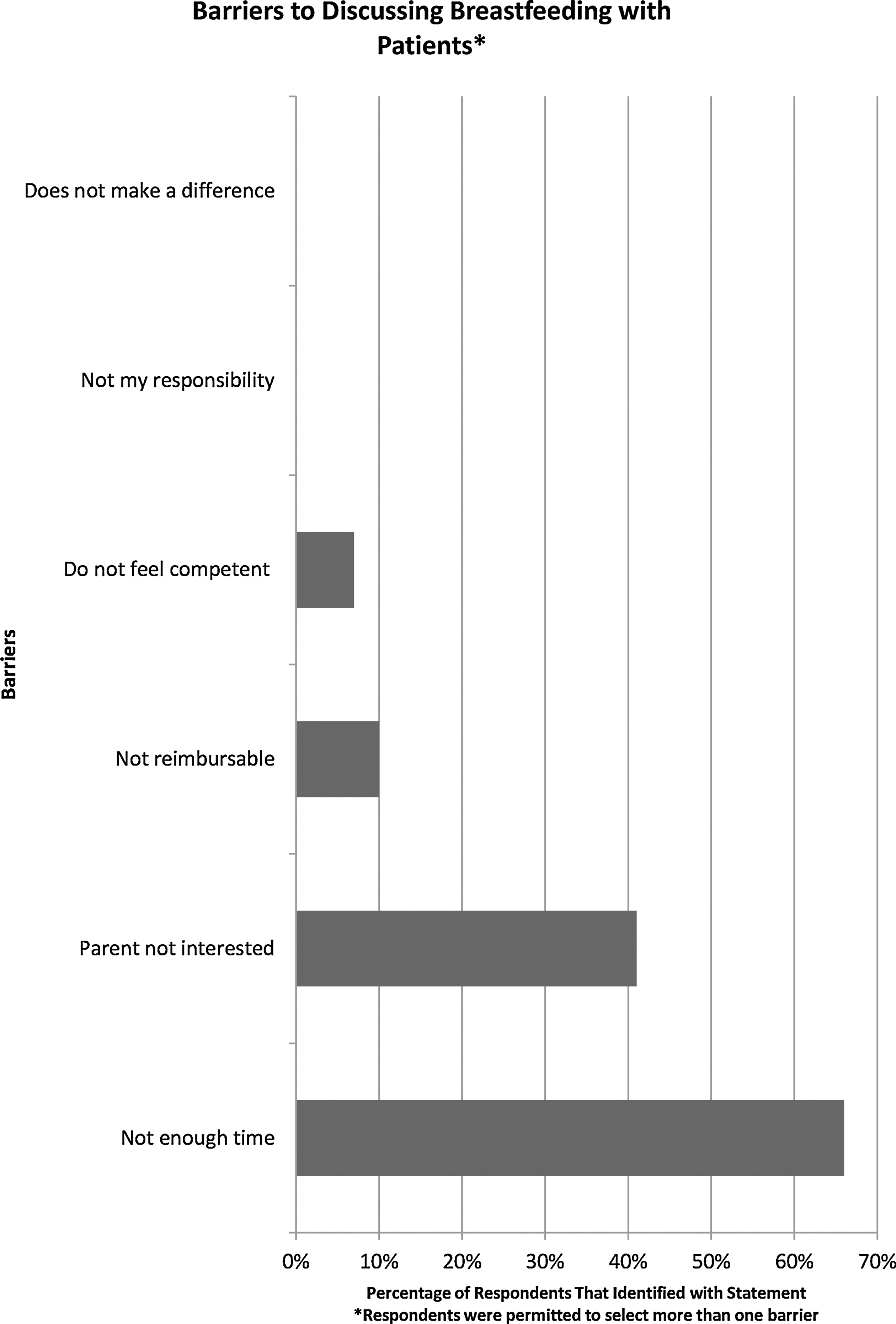
Barriers to discussion breastfeeding with patients. Respondents were permitted to select more than one barrier.

Barriers to exclusive breastfeeding in the hospital. Respondents were permitted to select more than one barrier. NICU, neonatal intensive care unit.
The identified institutional barriers to exclusive breastfeeding included families not being well informed (62%), families wanting formula (55%), recommendation for formula by nurses (35%), nursing staff not encouraging breastfeeding (35%), recommendation for formula by neonatologist (7%), physicians not encouraging breastfeeding (21%), and inadequate lactation consultation (38%).
Adoption of PC Core Measure Set
Over half of our respondents were unsure whether their institution had adopted the PC Core Measure Set (52%) or whether their facility was collecting data on exclusive breastfeeding (55%).
Discussion and Conclusions
Although participating obstetricians were aware that breastfeeding is the best infant nutrition and displayed positive attitudes, they had knowledge gaps and identified barriers to counseling the breastfeeding dyad. The results also point to systemic issues that inhibit both (1) individual breastfeeding counseling (including lack of time, lack of compensation for counseling) and (2) hospital-wide exclusive breastfeeding, such as inadequate lactation staffing and conflicting messages from providers. The majority of respondents were unaware of hospital data collection about exclusive breastmilk feeding.
This is the first study (based on an examination of Medline; 1966–February 2014; English language; search terms of “perinatal care core measure set,” “obstetricians breastfeeding”) to examine obstetrician knowledge of the PC Core Measure Set. Adoption of the Core Measure Set was voluntary during the time frame of our data collection; therefore their institutions may have elected not to participate, which could have contributed to the low number of respondents being aware of the Core Measure Set or their institution's data collection.
These results indicate that there is not only a need for more breastfeeding education among DC obstetricians, but also better outreach to staff obstetricians about the PC Core Measure Set. Increased knowledge of these performance measurement systems may lead to better adherence of data collection, yielding improved care.
Limitations of this study include a limited sample size and respondents from the same geographic area. Additionally, because of the level of anonymity in this survey, it is unclear how many of the eight birthing facilities in Washington, DC were represented among the respondents.
We propose the following recommendations: (1) work with ACOG chapters to implement effective education programs for their members regarding perinatal breastfeeding management; (2) develop strategies for incorporating and documenting breastfeeding counseling into routine prenatal visits, including the addition of breastfeeding counseling sections into electronic health records; (3) advocate for reimbursement for prenatal breastfeeding education through insurance companies; (4) increase provider familiarity with local lactation resources; and (5) provide formalized training for providers on The Joint Commission PC Core Measure Set, to better understand institution goals and data collection.
Obstetricians play a crucial role in increasing the rate of in-hospital exclusive breastfeeding because they are one of the few medical providers who can influence and provide support to women prenatally. Our survey of the DC ACOG chapter indicates that these obstetricians understand the importance of encouraging and supporting breastfeeding, but need better education regarding breastfeeding management and the PC Core Measure Set. Attention should be given to identifying efficient instruments for breastfeeding education because time was identified frequently as a barrier.
Footnotes
Acknowledgments
We thank Pamela D. Berens, MD, FACOG, FABM, Professor of Obstetrics and Gynecology, University of Texas, Houston, Constance Bohon, MD, FACOG, DC Fellow Section Chair, ACOG, and Jianping He, MS, Children's Research Institute of Children's National Health System.
Disclosure Statement
No competing financial interests exist.