
Abstract
Abstract
Safe handling and preparation of breastmilk within the hospital setting are often taken for granted, and the process may not be scrutinized until problems arise. Areas of concern focus on both risk of contamination of breastmilk feedings due to handling and fortification and risk of a breastmilk misadministration. In two phases, Children's Hospital of Orange County (Orange, CA) implemented centralized breastmilk handling and breastmilk bar code scanning. As a result of these process changes, reports of breastmilk administration errors decreased to zero. However, bar code scanning allowed for the tracking of near misses. During the first 6 months of breastmilk bar code scanning, 55 attempts to feed the wrong breastmilk to the wrong patient and 127 attempts to feed expired breastmilk were prevented. Our findings are consistent with current practice recommendations that support the use of centralized breastmilk handling and systems for proper identification of breastmilk.
Introduction
S
Materials and Methods
Between May 2010 and May 2012, Children's Hospital of Orange County (Orange, CA) reported 45 breastmilk handling errors (Table 1). As a result of these errors, some immediate steps were taken to reduce risk, and a failure mode effects and analysis (FMEA) on breastmilk handling was initiated.
PI, Breastmilk Handling Performance Improvement Team.
A multidisciplinary FMEA team was formed that included representatives from each hospital inpatient unit, clinical nutrition and lactation services, risk management, transport, and neonatology. This FMEA team reviewed the entire breastmilk handling process, including collection, storage, transport, administration, and discharge, to identify all potential failure points. In total, 282 potential failure points were identified, which were then scored on a scale of 1 to 10 in three categories: severity, occurrence, and detectability. These three scores were multiplied together to obtain a risk priority number for each failure point. The risk priority number scores were then prioritized, and the root causes were identified for each of the top 85 potential failure points. Four primary areas of concern were identified. First, the process was unclear and cumbersome for the bedside registered nurse (RN). Second, there were inadequate double checks at key points in the process, including at the time a mother was provided with labels for her pumped milk and during the preparation process where an RN could be combining multiple bottles to prepare a feeding. Third, due to the frequency of breastmilk handling, there was risk of human error and confirmation bias. With approximately 7,000 individual breastmilk feedings per month, a nurse could handle breastmilk 12 times per shift, increasing the risk of error and reduced sensitivity to the risks. Finally, there was risk of contamination because the neonatal intensive care unit had no designated space to handle breastmilk other than the patient's bedside, and accounts of serious illnesses that have been traced to the improper handling of infant feedings within the hospital setting have been reported in the literature.1–4 Furthermore, of the 85 targeted potential failure points, 55% were unlikely to be detected.
The findings of the FMEA team led to the formal charter of a Breastmilk Handling Performance Improvement (PI) Team with the goal of redesigning the processes for breastmilk handling based on the identified failure points and underlying root causes.
Phase I (January 9–November 11, 2013)
During Phase I, centralized breastmilk preparation using dietetic technicians, registered (DTRs) was implemented. Quantities for 12 hours' worth of feedings were prepared twice daily and unit-dosed into enteral syringes for those receiving tube feedings or bottles for those receiving oral feeds. Orders were reviewed via the electronic medical record before each batch preparation time. The DTR would calculate the amount of breastmilk and each additive to make the desired 12-hour volume of feedings, which included a hospital standard overfill. This was documented on the individual patient's breastmilk preparation sheet, which also included patient information, the current order, and specifics as to what was prepared at each batch. Labels with the current breastmilk order were generated directly from the electronic medical record. To ensure proper identification, two DTRs were required to read aloud the patient's first and last name along with the medical record number from every bottle being used to prepare the current batch and compare this with the labels printed to be placed on the prepared feedings. Documentation of this double check was done at every preparation, with each DTR initialing the patient's individual breastmilk preparation sheet. The DTR would then prepare the feeding per the order, use the printed labels, and manually write in the correct expiration date and time on each label.
The other double check steps occurred either before feeding or at discharge. The existing policy required the RN to have another person validate the patient's identity using the name and medical record number prior to feeding breastmilk and prior to sending any breastmilk home with a family. To streamline the process for the RN at the time of discharge, two DTRs would provide a double check of each bottle for an individual patient and place the bottles into sealed bags. The sealed bags were then labeled on the outside with a patient label including the initials of the two DTRs who had conducted the double check. Upon releasing the bags of milk to the parent, the RN would then just double check the patient label on the outside of the sealed bag with another associate or the parent rather than having to double check each bottle.
The Breastmilk Handling PI Team determined that processes implemented during Phase I would address 63 of the top 85 potential failure points (74%).
Phase II (November 12, 2013–May 12, 2014)
At the time Phase I was implemented, the Breastmilk Handling PI Team was also pursuing a breastmilk bar code system to further improve patient safety. It was determined that bar code scanning would address 12 of the remaining 22 top potential failure points. The system chosen interfaced directly with the hospital electronic medical record, reducing risk and improving patient safety through three primary areas. First, the system automatically calculated the exact amounts of breastmilk and additives for each 12-hour batch, which eliminated the need to manually calculate, thus decreasing the risk of human calculation error. Second, it used bar code scanning to replace the two-person double check at the time of preparation, feeding, and discharge, again reducing the risk of human error and improving efficiency. Finally, it automated the labeling process, reducing the risk of error with regard to the handwritten expiration dates and times.
Results
The flow diagram shown in Figure 1 outlines the process improvement steps taken and results for each phase. Outcome data collection for the 10 months of Phase I (centralized breastmilk handling with a manual two-person double check) showed that total breastmilk errors dropped to seven: four breastmilk labeling errors and three breastmilk storage errors (Table 1). There were no incidents of the wrong milk reaching the wrong baby during Phase I.
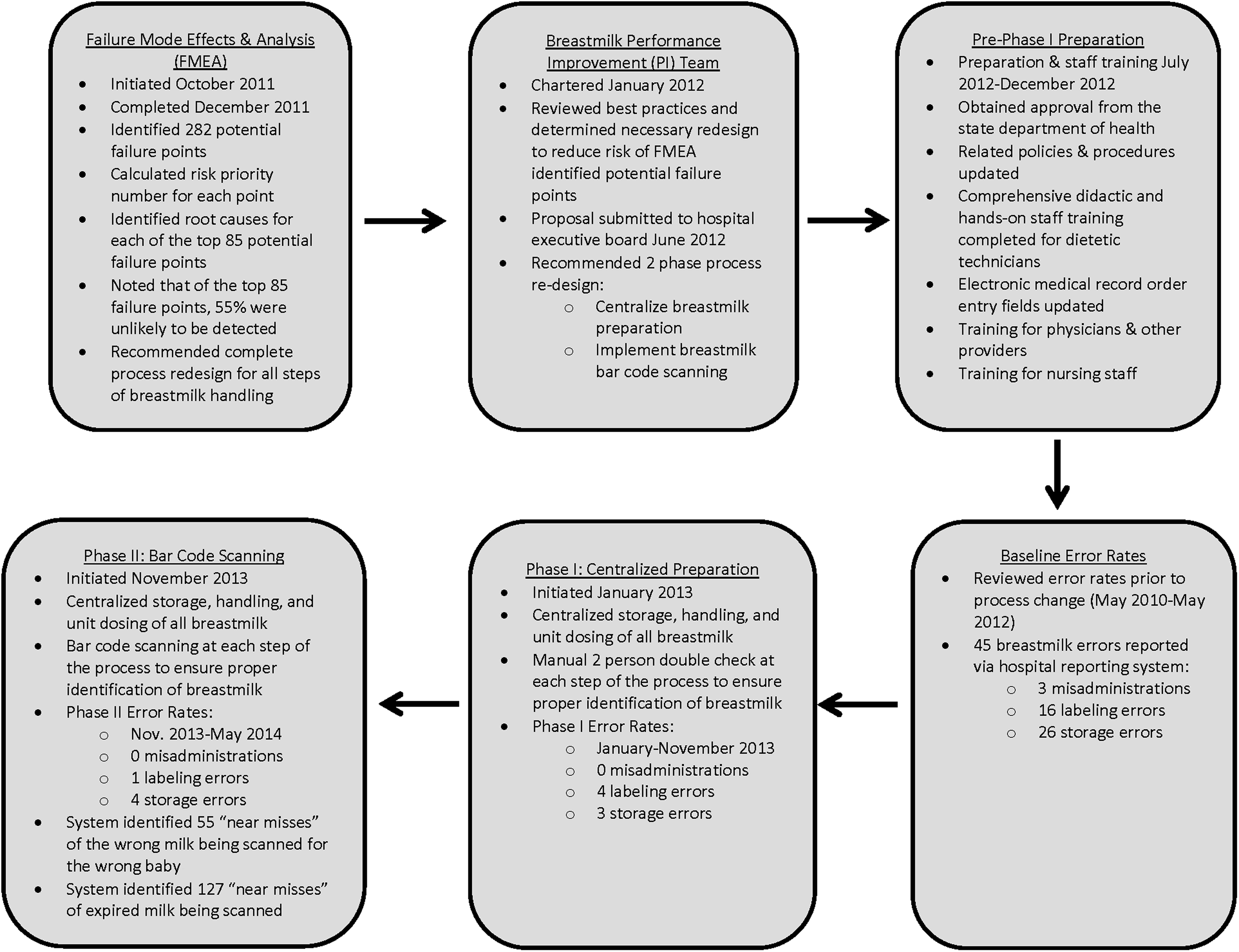
Breastmilk handling improvement steps and outcomes.
Six-month outcome data for Phase II (centralized preparation with breastmilk bar code scanning) showed that total breastmilk errors dropped to four (Table 1). Three were breastmilk storage errors, where correctly labeled milk was placed in the wrong patient's bin but not administered to the wrong patient. One was a breastmilk labeling error that was caught before the milk reached inventory or any patient. There were no incidents where the wrong milk reached the wrong patient. However, the system caught 55 near misses where the wrong breastmilk was scanned to the wrong baby. The system alerted the RN or DTR and prevented a misadministration from occurring. Additionally, the system prevented 127 incidences of expired breastmilk feeds from being administered (83 in months 0–3 and 44 in months 4–6).
Discussion and Conclusions
As noted in the original FMEA, the vast majority of potential failure points were unlikely to be detected with the prior systems. The centralization of breastmilk handling and use of bar code scanning provided a framework for closer scrutiny to the breastmilk handling processes and allowed for tracking of breastmilk administration errors and near misses.
Centralization of breastmilk handling allowed for greater emphasis on infection control measures and increased double checks at key points of the process to reduce the risk of misadministration. Bar code scanning further improved safety by eliminating manual calculations of additives and the potential for human error at each double check step.
In addition, bar code scanning reduced the risk of a patient receiving expired breastmilk, which could be an infection risk. Prior to bar code scanning, there were no reported incidents of expired breastmilk being administered; however, there were no monitoring systems in place to detect such issues. Thus, implementation of bar code scanning highlighted a potential problem area that was not adequately monitored under previous processes. This, in turn, brought awareness around the issue of using breastmilk feeds in designated order to prevent milk from expiring and being wasted. Such awareness was evident in the decrease in number of attempts to scan expired milk, which decreased almost in half between the first 3 months and the second 3 months of bar code scanning.
Current recommendations and reports of best practices suggest that centralized handling of breastmilk and use of bar code scanning improve patient safety.1,5 Our research supports such theories and highlights the importance of proper attention to breastmilk handling within the hospital setting.
Footnotes
Disclosure Statement
No competing financial interests exist.