
Abstract

T
The global statistics on the benefits of breastfeeding are quite striking. An increase in breastfeeding could prevent 800,000 child deaths each year. 1 Breastfeeding within an hour of birth could prevent 20% of newborn deaths.2–4 Breastfeeding also has a protective effect on death within the first 28 days, including all-cause mortality (44% lower risk), deaths from infections (45% lower risk), and deaths among low-birth-weight babies (42% lower risk).2,3 Infants who are exclusively breastfed are 11 times less likely to die from diarrhea and 15 times less likely to die from pneumonia 5 —the two leading killers of children under 5 years of age. Studies show that breastfeeding promotes cognitive development, resulting in improved school performance and academic outcomes. 6 Breastfeeding is also good for mothers 7 and good for the environment 8 and reduces healthcare costs. 9
Despite the evidence, the majority of new mothers do not breastfeed their babies exclusively (breastfeeding only, with no additional food, water, or other liquids) for the first 6 months. Worldwide, only 39% of children under 6 months of age are exclusively breastfed and there has been little improvement in the past 15 years (Fig. 1). 10
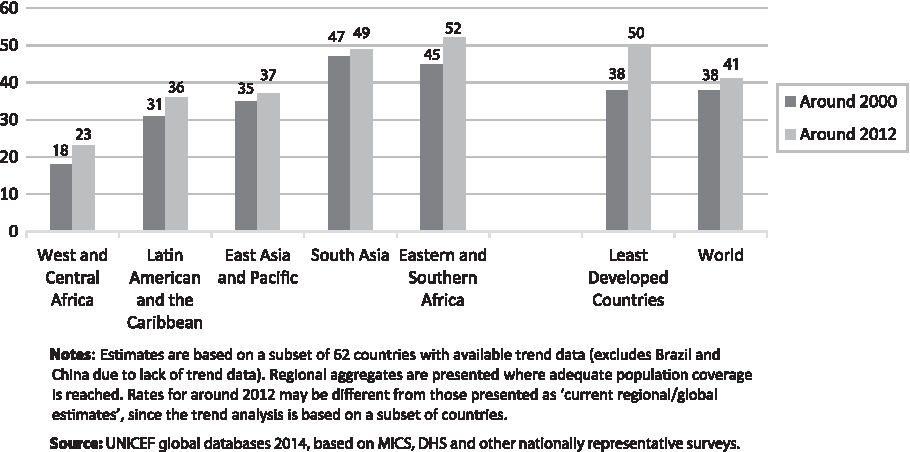
Percentage of infants aged 0–5 months that are exclusively breastfed, by region, around 2000 and 2012.
There is also slow progress on raising early initiation rates—more than half of newborns globally are not breastfed within the first hour of life. 10
The reasons for the lack of progress in increasing breastfeeding rates encompass a number of social, cultural, educational, political, and commercial factors (such as the aggressive marketing of infant formula and other breastmilk substitutes). With respect to culture, in some countries it is a long-standing cultural practice to give a baby water or herbal tea or to discard colostrum, which is perceived as dirty. There is also a financial factor—many women have to return to work and lack paid maternity leave. In addition, women may lack supportive workplace policies to enable them to continue breastfeeding.
Despite these challenges, 20 countries have significantly increased their breastfeeding rates by 15 percentage points or more in the preceding five years (11 countries [Fig. 2]) or have high achievement (more than 50% coverage; 9 countries, not shown).
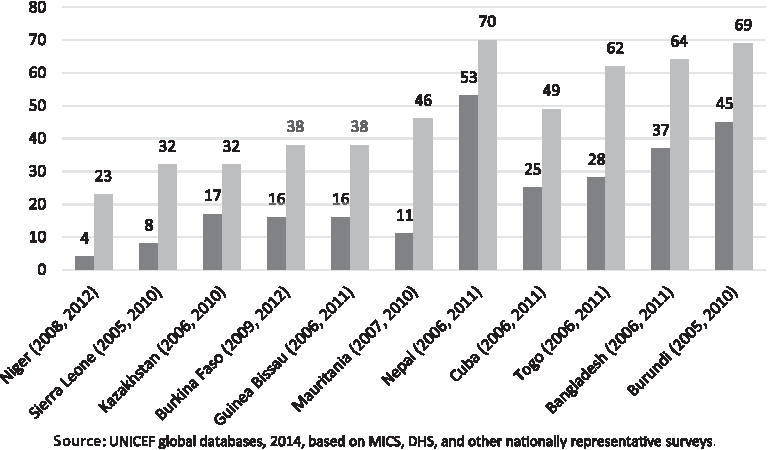
Twenty countries with significant increases in breastfeeding rates by 15 percentage points or more in the preceding five years (11 countries, shown in Figure 2) or have high achievement (more than 50% coverage; 9 countries, not shown).
How did this happen? It was a result of strategic programmatic efforts that included strong national leadership, counseling and support for mothers in health facilities and through peer support networks in communities, and mass communications efforts promoting breastfeeding in a culturally appropriate and relevant way. For example, in Cambodia, an analysis of the situation found that there was a widespread cultural practice to give water to babies. The government initiated a mass communications campaign through television advertisements spreading the message that babies should not be given water. The ads were coupled with extensive health worker training and the establishment of mother support groups. Breastfeeding rates increased significantly in the country—from 12% to 74% in less than 10 years. 11
A similar “no water” campaign was conducted in Vietnam through compelling advertisements. 12 Also in Vietnam, after research showing that only 20% of mothers were exclusively breastfeeding for the first 6 months, mainly because they were going back to work soon after giving birth, Alive and Thrive, UNICEF, and other partners engaged with local advocates, medical professionals, health workers, and government officials to strengthen policies to support breastfeeding. In 2012, the Government of Vietnam extended paid maternity leave to 6 months. It is yet to be seen if breastfeeding increases as dramatically in Vietnam as it did in Cambodia, but in just 2 years, exclusive breastfeeding rates have tripled in program areas. 13
Progress is possible and increases in breastfeeding rates can be achieved in a short period of time. But, the gains we have seen occurred in a small number of countries. What about the rest, especially those highly populous countries with low breastfeeding rates? Why are we not seeing systematic progress?
UNICEF conducted a stakeholder survey in 2012 to assess political commitment for breastfeeding, interviewing a number of nutrition and global health experts and advocates. 14 Stakeholders agreed that breastfeeding has not benefited from political and donor commitments in line with its potential to save lives. The report highlighted a number of challenges contributing to the low profile that breastfeeding has received on the development agenda, including (1) insufficient leadership for breastfeeding, (2) low prioritization and financial commitment by national policy makers and international donors resulting in a lack of implementation of breastfeeding programs at scale, (3) the influence and aggressive marketing of infant formula (and other breastmilk substitutes) by companies, (4) a lack of unified voice among breastfeeding experts and advocates, and (5) the lack of a compelling narrative and the need to elevate breastfeeding on the global development agenda.
As a result, UNICEF, the World Health Organization, and a number of partners have initiated a global advocacy drive to raise visibility and commitment for breastfeeding and have placed their institutional weight behind the issue. Partners have come together to develop an advocacy strategy to raise the profile of breastfeeding on the global development agenda. The initiative broadly aims (1) to raise the visibility of breastfeeding as a cornerstone of child survival, health, and development, (2) to secure new financial resources for national breastfeeding programs and supportive policies, (3) to strengthen political commitment to the issue, (4) to galvanize interest and excitement among internal and external stakeholders, and (5) ultimately to inspire a social movement that repositions breastfeeding as the norm.
The breastfeeding advocacy initiative has a number of strategic priorities, but one that is particularly urgent is to reframe the narrative and create new evidence-based messages to convey that breastfeeding is a crucial and smart investment to provide children the best start in life. Messages will emphasize the link between breastfeeding and positive effects on maternal health, brain development, cognitive ability, the environment, and savings for health systems and employers in order to reach a wide audience.
Audience research will be conducted to measure current awareness of breastfeeding, to identify specific target audiences for advocacy and develop messages that inspire audiences to become strong advocates for breastfeeding. Potential audiences are those who are in a position to increase political commitment, visibility, and resources for breastfeeding such as senior-level decision makers of United Nations agencies and international nongovernmental organizations, policy makers, donors, medical and health professional associations, human rights experts, and the media. Message testing will be conducted to determine what messages are most resonant and persuasive to various audiences that will compel them to action. Global-level messages that are developed would be tailored to specific targeted countries. The broad aim is to create a compelling case for breastfeeding and to tailor messages to specific audiences, as well as to align messages among advocates.
The way forward entails strong advocacy among partners and civil society actors using messages and stories that resonate with policy makers and other key audiences to spur action, engagement, and mobilization. The way forward also requires leveraging financial resources to strengthen policies and scale up programs, thus supporting and enabling more women to breastfeed.
Footnotes
Disclosure Statement
No competing financial interests exist.