
Abstract

G
The MGRS resulted in the current WHO Child Growth Standards. 3 Those standards have been adopted by over 130 countries since their introduction approximately 8 years ago. The standards now cover over 95% of children under 5 years of age globally. The INTERGROWTH-21st Project, completed only months ago, was designed to complement the MGRS by providing comparable international standards for fetal growth from 9 weeks of gestation to birth and newborn size (weight, length, and head circumference) according to gestational age and sex. 4
The MGRS and INTERGROWTH-21st Project are expected to merge well and to present opportunities for the continuum of care from early gestation through the first 5 years after birth, amply covering the “first thousand days,” a period increasingly recognized as critical to child and subsequent adult well-being. Both efforts were based on the new paradigm referred to in the introductory paragraph. That paradigm is basically a prescriptive approach (i.e., both efforts describe how children/fetuses should grow regardless of time and place), rather than one limiting the description of growth to past approaches (i.e., to describe how children grew at a particular time and place). 1 The new approach expands the definition of health beyond “an absence of disease criterion” to include the adoption of recommended health behaviors and practices (e.g., breastfeeding as the best postnatal healthy start).
There were other design features common to both efforts. For example, both studies included multiple, diverse international sites, and both used community-based sampling to avoid biases such as those likely to emerge from hospital-based sampling frames. Both used real-time quality controls, which in my view contributed significantly to the high-quality data obtained by both studies.
What do these two sets of international growth standards represent? The new prenatal and postnatal “prescriptive-based” standards enable improved support and management of pregnancy and postnatal care, especially breastfeeding. For example, because of the new WHO standards, breastfeeding women and their physicians and other healthcare providers no longer have to counter the erroneous idea that exclusively or predominantly breastfed children cannot maintain expected growth trajectories past 2 or 3 months of postnatal life. 5 Both sets of standards should enhance the potential to improve maternal and child health policies and goals and open novel research opportunities, especially for the improved treatment and management of premature and small-for-gestational-age infants.
In brief, the MGRS included two components: a longitudinal one from 0 to 24 months that overlapped with a cross-sectional component that included children 18–71 months of age. It operationalized definitions for “optimal” nutrition, environments, and care with the goal of defining “optimal” growth, within constraints of studies conducted in community-based settings. The MGRS obtained data on growth trajectories from birth to 5 years in children enrolled from six different countries: Brazil, Ghana, India, Norway, Oman, and the United States. The study involved 8,440 children and their families.3,6
The INTERGROWTH-21st Project included three complementary components. 4 There was a cross-sectional study of all newborns in eight study sites in Brazil, China, India, Italy, Kenya, Oman, the United Kingdom, and the United States. A cohort of healthy women was also enrolled in a longitudinal component in the same centers to monitor fetal growth with ultrasound scans every 5±1 weeks from 9 to 14 weeks of gestation to birth. The cohort was followed to 2 years of age to assess health, growth, and neurodevelopment. In addition, in the third component, the postnatal growth of those infants in the longitudinal cohort who were born prematurely was monitored closely. Nearly 60,000 children and their families have been enrolled in the three study components.
The eligibility criteria used by the MGRS and the INTERGROWTH-21st Project were similar.3,4 They were designed to identify healthy populations seemingly free of disease, following current health recommendations, and living in environments highly unlikely to constrain growth. The goal of both studies was to describe how individuals in healthy communities grow, effectively setting the public health bar robustly in terms of expectations for healthy growth.
The specific contexts of healthy conditions necessarily differed among study sites because individuals from very diverse countries were enrolled (e.g., India, Italy, Kenya, and Norway), but all contexts shared at least one common feature: each was assessed to be non–growth-constraining. Other site/environmental/population characteristics were controlled across all sites (e.g., altitude, because of its documented impact on fetal growth). The MGRS limited its study populations to those living at less than 1,500 m; the INTERGROWTH-21st Project set its limit at 1,600 m so as to include a sub-Saharan site (Nairobi, Kenya) in a malaria-free region. Also, the longitudinal aspects of both studies required low mobility populations.
Among the key care criteria adopted by the MGRS and of particular interest to the Academy of Breastfeeding Medicine was that all enrolled children were to be breastfed exclusively or predominantly for 4–6 months with continued breastfeeding for at least 1 year. This was compatible with recommendations at the time the MGRS was designed, yet viewed by many as overly ambitious. As such, initial goals were tempered (e.g., evidence was sought from candidate MGRS sites documenting that at least 20% of enrolled mothers would be able to follow the study's feeding guidelines). Yet, the MGRS achieved a success rate of nearly 70% in terms of continued breastfeeding through 12 months, much higher than the initially expected rate of 20%. 7 That success was due in large part to the selection of sites with existing breastfeeding support systems that the MGRS could strengthen.
Other MGRS eligibility criteria were selected to help ensure the absence of growth-constraining conditions for individuals. Thus, in addition to the willingness of mothers to follow feeding recommendations, only infants of women who did not smoke before or after delivery were included; as for the children, only singletons and those born at term and free of any significant morbidity were enrolled. Similar but expanded criteria were used in the INTERGROWTH-21st Project (e.g., no relevant past medical history that could affect pregnancy adversely, and only singleton pregnancies achieved through natural conception were eligible). 4
The INTERGROWTH-21st Project plans to publish gestational age- and sex-specific newborn standards, as well as new phenotypic classification systems for the preterm birth and small-for-gestational-age/intrauterine growth restriction syndromes that are associated with distinct perinatal outcomes. The fetal growth longitudinal component will provide international standards for routinely obtained ultrasound measures (e.g., head and abdominal circumferences and femur length), and the preterm postnatal follow-up study will provide preterm postnatal growth standards (e.g., length, weight, and head circumference). 4
The WHO Child Growth Standards provide a unique set of international norms for attained growth and growth velocities.8–10 As a result, expectations for achievable healthy growth have been upgraded significantly, resetting the bar for ensuring the “best start” for all children. The INTERGROWTH-21st Project should provide similarly innovative international tools for the assessment of fetal growth and newborn status and the evaluation of relevant health policies.
Preliminary data from the INTERGROWTH-21st Project show strikingly similar fetal skeletal growth and newborn linear size across sites despite, as was the case in the MGRS, contextual and ethnic differences inherent to the project's intersite diversity. As was the case with the MGRS, similarities in growth patterns appear to hold despite disparities in parental stature across sites and support the view that intrauterine growth is similar across populations when mothers' nutritional and health needs are met and environmental constraints on growth are low. If final intrauterine growth patterns are found to be similar across sites in a manner analogous to the observations of the MGRS, revisiting biological limits on fetal growth putatively imposed by maternal constraints will be of interest. 11
The INTERGROWTH-21st Project newborn birth weight, length, and head circumference data also appear to be similar across the eight sites. Thus, expected gestational age- and sex-specific newborn size standards should provide nurseries with tools to assess the appropriateness of birth anthropometric characteristics of children born at various gestational ages.
In brief, I fully expect that the INTERGROWTH-21st Project's results will be consistent across its eight sites as was observed by the MGRS across its six sites (Fig. 1). 12 Figure 1 summarizes a key message of the MGRS likely to be strengthened by the INTERGROWTH-21st Project. The MGRS supports the view that human growth potential is universal for healthy populations at least through 5 years of age when health, environmental, and care needs are met. The INTERGROWTH-21st Project results likely will expand that to include growth during gestation.
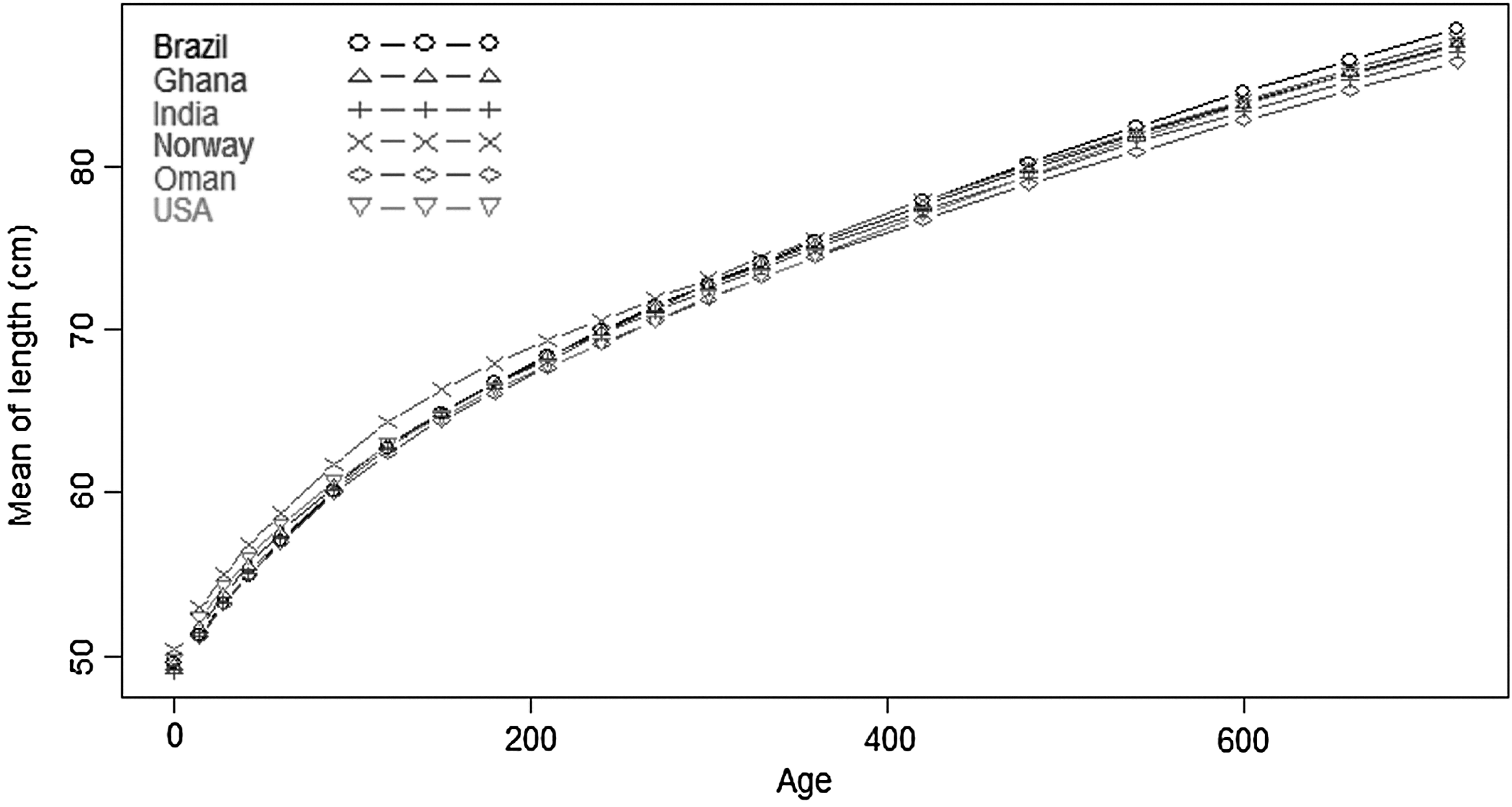
Mean length (cm) from birth through 2 year for each of the six Multicenter Growth Reference Study sites. Reproduced with permission from the WHO Multicentre Growth Reference Study Group. 12
This view raises inevitable questions relevant to the use of standards developed “prescriptively.” For example, “How is the similarity in growth possible given the enrolled populations' distinct genetic backgrounds?” It is true that tall parents tend to have tall children and that short parents tend to have short children, but such expectations reflect interindividual rather than interpopulation variation. Furthermore, because growth is a complex, quantitative genetic trait, it is not surprising that genome-wide association studies have identified many genes, approximately 200, associated with the genetic control of stature. 13 Those 200 genes explain approximately 10% of observed variability, much less than the 40–80% expected from earlier studies completed before the availability of genomic approaches. The small proportion of variation in stature explained by genes identified to date may result from a failure to detect a substantial number of genes with weaker effects that nonetheless have a significant cumulative impact and/or from the failure to account for other mechanisms (e.g., epistasis). Additionally, the relatively low proportion of variability explained by that large number of genes likely reflects the influences on stature by nutrition and other care and environmental variables in ways that remain understood incompletely. In brief, these considerations lead to the expectation that most variation in growth exists among individuals rather than among populations, an expectation borne out by the MGRS and expected to be bolstered by the INTERGROWTH-21st Project.
The assertion of similar growth potentials across populations also elicits questions as to whether or not standards based on prescriptive designs can be used appropriately in undernourished populations. After all, doesn't current thinking support a multigenerational time frame for the normalization of the stature of children of growth-stunted parents? 14 This question was examined recently by comparing projected adult heights of children enrolled in the MGRS. 15 Projected adult heights were estimated by doubling the children's length at 2 years of age (adjusting length measurements for estimations of stature). That study accepted the thesis that doubling a child's stature at 2 years of age predicts adult height reasonably well at a population level and that those predictions compare favorably with mid-parental heights, at least among well-nourished populations. 16
In examining this question, my colleagues and I predicted that no significant differences would be observed between mid-parental heights and the MGRS children's projected adult heights in Norway and the United States, but that substantial differences would be observed in the four sites more likely to have included parents who experienced growth constraints during their childhoods. Figure 2 summarizes the results of that comparison. As predicted, no differences were observed between mid-parental heights and the children's predicted adult height for the U.S. and Norwegian sites; however, differences of approximately 6–8 cm were observed in the children's favor in the remaining four sites.
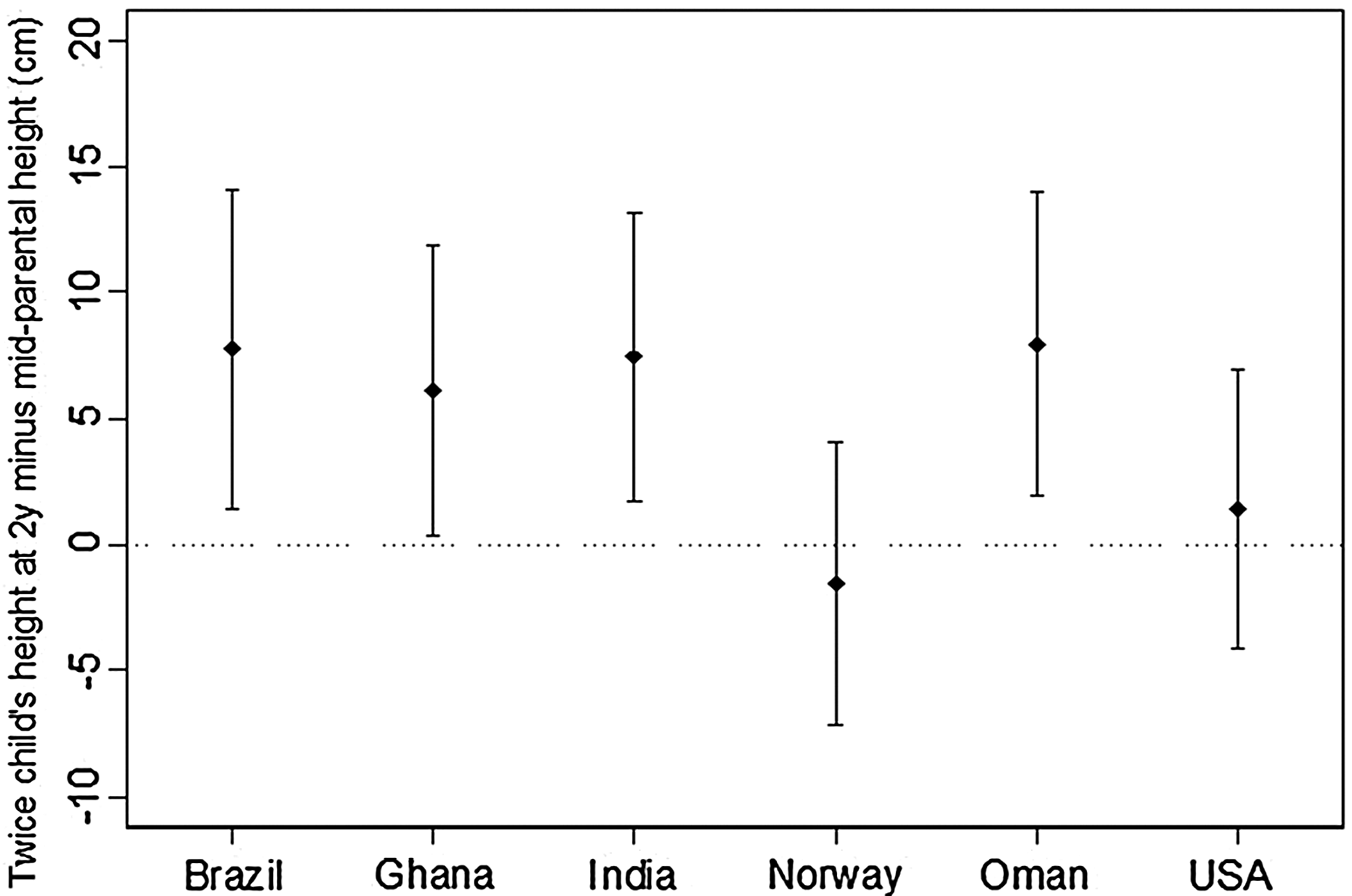
Means (points) and standard deviations (bars) of the difference between two times the height of the child at 2 years and the mid-parental height by site. Reproduced with permission from Garza et al. 15
These analyses support the expectation that, from a biological perspective, significant progress is achievable within one generation in redressing nongenetic, constrained growth. The key caveat is that health, environmental, and care needs must be met from gestation through childhood. Furthermore, gaps between expectations based on the new standards and what is achieved in most settings will likely and primarily reflect the consequences of disease, adverse environments, and/or inadequate nutrition and care rather than genetics or parental experiences. Thus, comparisons of “growth performance” against the new standards should inform clinical management and policy choices. In sum, these efforts support the view that a disproportionate number of individuals with shorter than expected stature in populations is not necessarily the result of limits imposed by parental childhood experiences or genetics, but more likely is the result of political and economic constraints.
Note
Two important articles17,18 based on the INTERGROWTH-21st Project have either been published or been accepted for publication since the Sixth Annual Summit on Breastfeeding, held on June 2–3, 2014. Those articles affirm preliminary analyses discussed in the talk on which this manuscript was based.
Footnotes
Acknowledgments
I wish to thank Professor Stephen H. Kennedy of the Neufield Department of Obstetrics and Gynecology and Oxford Maternal and Perinatal Health Institute, Green Templeton College, University of Oxford, for his generous and careful review of the manuscript for the accuracy of preliminary findings shared with the INTERGROWTH-21st Project Scientific Advisory Committee. Any remaining errors are solely the author's responsibility.
Disclosure Statement
No competing financial interests exist.