
Abstract
Abstract
Background:
Quantification of the association between breastfeeding and breast cancer risk is still conflicting. Therefore, we conducted a meta-analysis to summarize the evidence from epidemiological studies of breastfeeding with the risk of breast cancer.
Materials and Methods:
Pertinent studies were identified by a search of PubMed between January 1, 2008 and July 31, 2014. The random-effect model was used. Sensitivity analysis, subgroups analysis, and publication bias were conducted.
Results:
Twenty-four articles with 27 studies involving 13,907 breast cancer cases were included in this meta-analysis. Pooled results suggested that breastfeeding was inversely associated with the risk of breast cancer. The summary relative risk (RR) of breast cancer for the ever compared with never categories of breastfeeding was 0.613 (95% confidence interval [CI], 0.442–0.850). An inverse association was also found for the longest compared with the shortest categories of breastfeeding with the risk of breast cancer (RR=0.471; 95% CI, 0.368–0.602). No evidence of publication bias was found.
Conclusions:
Findings from this meta-analysis suggest that breastfeeding, particularly a longer duration of breastfeeding, was inversely associated with risk of breast cancer.
Introduction
B
Breastfeeding is hypothesized to reduce the risk of breast cancer primarily through two mechanisms: facilitating differentiation of mammary cells and reducing the lifetime number of ovulatory cycles.2–4 Bernier et al. 5 performed a meta-analysis including 40 studies in 2000 and showed that breastfeeding can reduce the breast cancer risk. A systematic review 6 was conducted including 31 studies published between 1999 and 2007 to assess the association between breastfeeding and breast cancer risk. However, epidemiological evidence on this issue remains controversial after 2008. Some studies reported that breastfeeding did not modify breast cancer risk,7–14 whereas other studies suggested either a decreased risk in women who had ever breastfed15–17 or a decreased risk in women who had the longest breastfeeding duration.18–30 The aim of the present study was to carry out a meta-analysis of the relationship between breastfeeding and breast cancer, based on the epidemiological literature published in peer-reviewed journals between 2008 and 2014.
Materials and Methods
Search strategy
We performed a comprehensive literature search including published studies from database use of PubMed during the 6-year period between January 1, 2008, and July 31, 2014. The search was limited to published studies in English and studies of humans by using the following search key words and Medical Subject Headings terms: (breastfeeding OR breast feed OR lactation OR infant nutrition OR breast milk OR milk human) AND (breast) AND (cancer OR neoplasm OR carcinoma OR tumor). We also reviewed references of all included studies for additional publications.
Study selection
To be included, studies had to use a case-control, cohort, or cross-sectional study design and investigate the association between ever breastfeeding or the total duration of breastfeeding and incidence of breast cancer. The publication had to present the hazard ratio, odds ratio (OR), or relative risk (RR) with 95% confidence intervals (CIs) or data necessary to calculate these. When multiple publications from the same study were available, we used the publication with the largest number of cases and most-applicable information.
Data abstraction
For each eligible study, two investigators independently performed the eligibility evaluation and data abstraction. Disagreements were discussed and resolved by consensus. Data abstracted from each study were as follows: author list, year of publication, study region and design, study sample size (number of cases and controls or cohort size), duration of follow-up for cohort studies, exposure and outcome assessment including ever breastfeeding and the total or average breastfeeding duration categories, study-specific adjusted estimates with their 95% CIs for ever compared with never breastfeeding and longest compared with shortest of the total or average duration category of breastfeeding, and factors matched by or adjusted for in the design or data analysis. If multiple estimates of the association were available, we abstracted the estimate that adjusted for the most covariates. If no adjusted estimates were presented, we included the crude estimate. If no estimate was presented in a given study, we calculated it and its 95% CI according to the raw data presented in the article.
Statistical analysis
The pooled measure was calculated as the inverse variance-weighted mean of the natural logarithm of multivariate adjusted RR with 95% CI for breastfeeding and breast cancer risk. The random-effects model was used to combine study-specific RR (95% CI), which considers both within-study and between-study variation. 31 The Q test and I2 of Higgins and Thompson 32 were used to assess heterogeneity among included studies. I2 describes the proportion of total variation attributable to between-study heterogeneity as opposed to random error or chance, and I2 values of 0%, 25%, 50%, and 75% represent no, low, moderate, and high heterogeneity, respectively. 33 Meta-regression with restricted maximum likelihood estimation was performed to assess the potentially important covariate exerting substantial impact on between-study heterogeneity. 34 Publication bias was estimated using Egger's regression asymmetry test. 35 A study of influence analysis 36 was conducted to describe how robust the pooled estimator is to removal of individual studies. An individual study is suspected of excessive influence if the point estimate of its omitted analysis lies outside the 95% CI of the combined analysis. All the statistical analyses were performed with STATA version 10.0 software (StataCorp, College Station, TX). A two-tailed p value of <0.05 was accepted as statistically significant.
Results
Study characteristics
The search strategy identified 1,479 articles from PubMed. Twenty-four articles7–30 with 27 studies were used in this meta-analysis. The detailed steps of our literature search are shown in Figure 1. The included articles, which represented 13,907 cases, were published between 2008 and 2014 and consisted of three cohort studies, 23 case-control studies, and one cross-sectional study. All of the studies only included parous women in analyses. The detailed characteristics of the 24 articles are shown in Table 1.
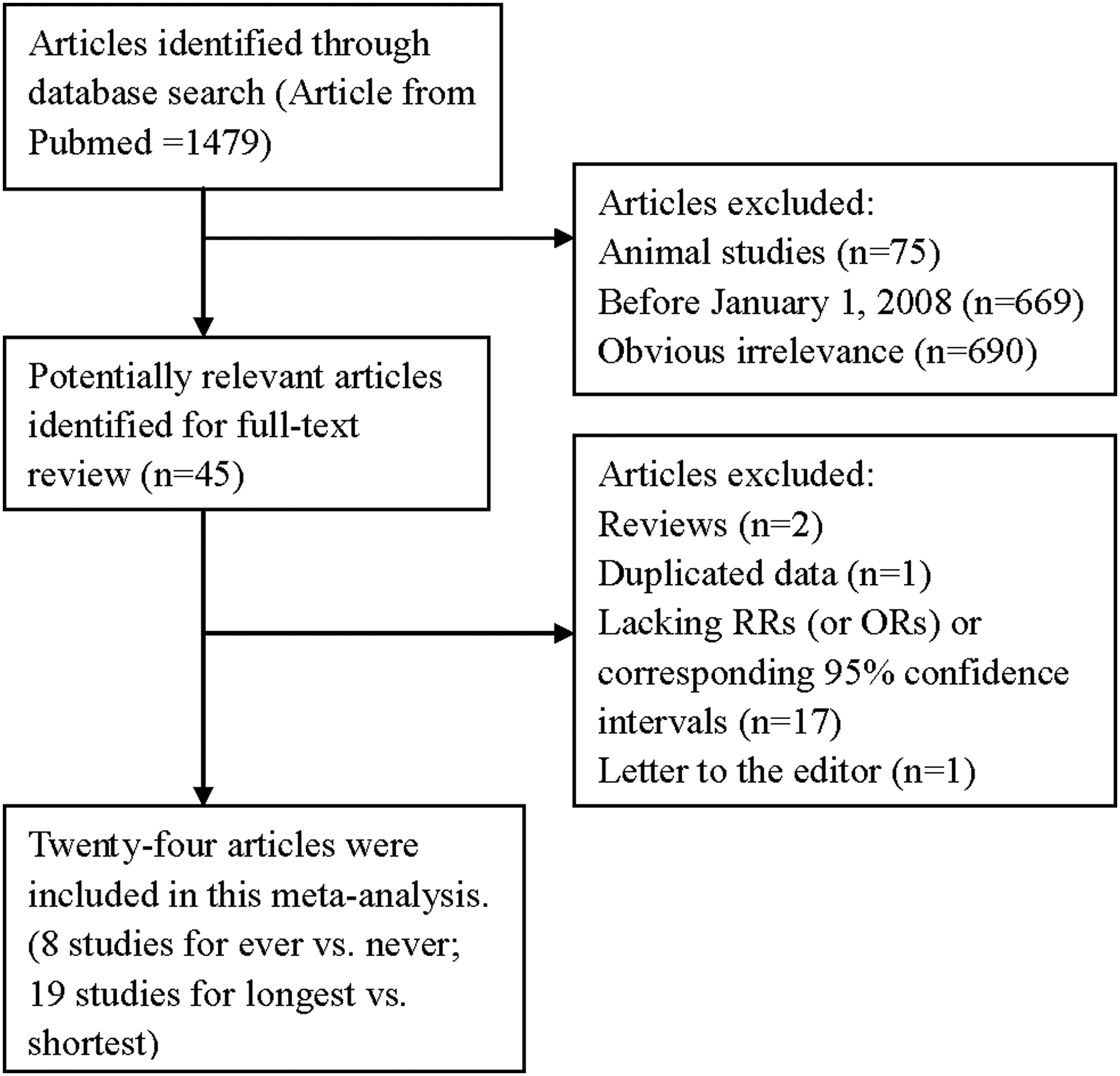
The flow diagram of screened, excluded, and analyzed publications. OR, odds ratio; RR, relative risk.
BMI, body mass index; ER, estrogen receptor; HCC, hospital-based case-control study; HRT, hormone replacement therapy; NA, not available; PCC, population-based case-control study; PR, progesterone receptor.
Breastfeeding and breast cancer
Twenty-four articles with 27 studies were included in this meta-analysis. Inverse association of breastfeeding with the risk of breast cancer was reported in 18 studies, whereas no significant association was reported in nine studies. Pooled results suggested that breastfeeding could reduce the risk of breast cancer: summary RR=0.510; 95% CI, 0.411–0.632; I2=87.5% (Fig. 2).
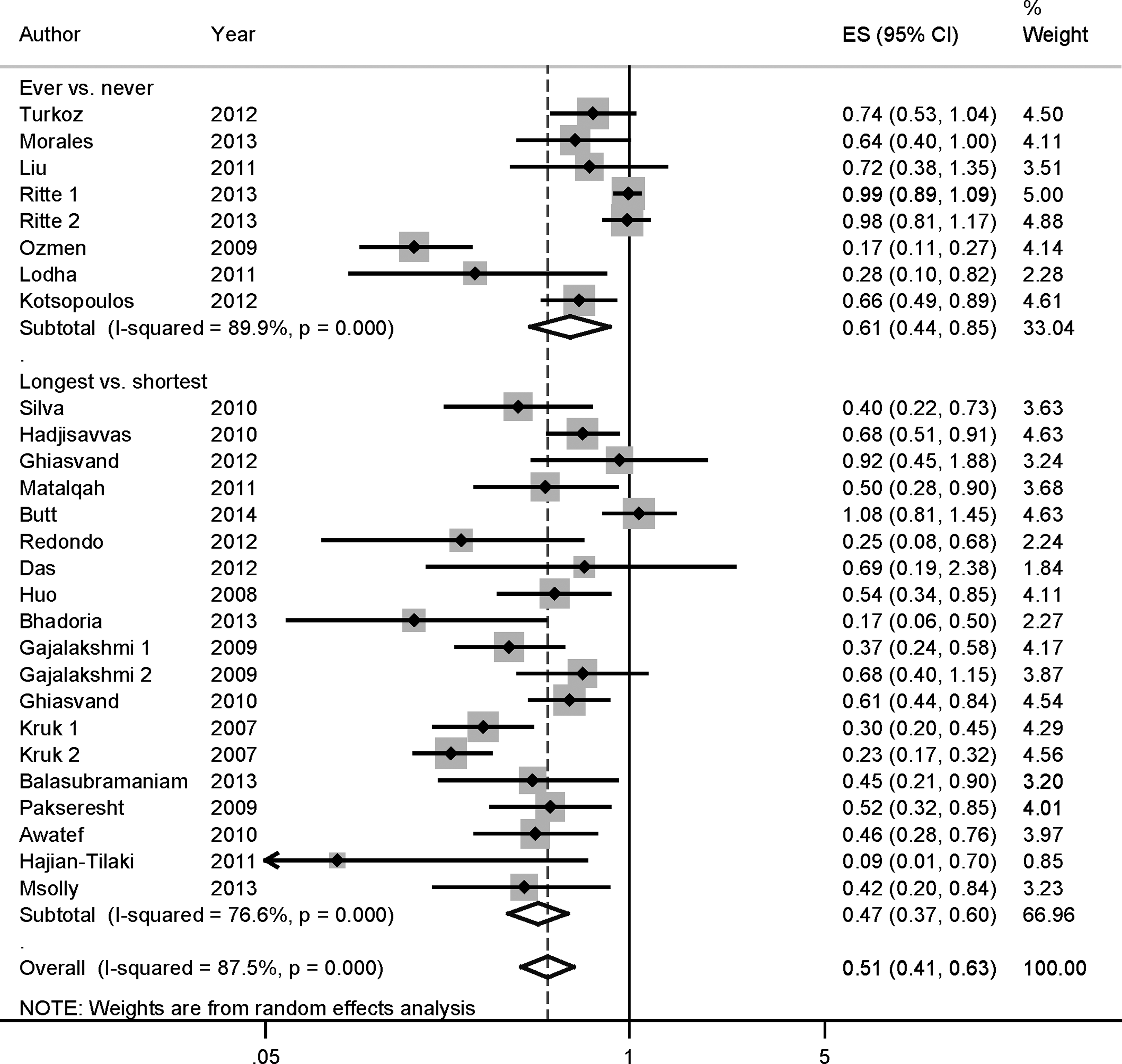
The forest plot between breastfeeding and breast cancer risk.7–30 The white diamonds denote the pooled relative risk. Black squares indicate the relative risk in each study, with square sizes inversely proportional to the standard error of the relative risk. Horizontal lines represent 95% confidence interval. ES, effect size.
Ever-breastfeeding and risk of breast cancer
Eight studies7–10,15–17 comprising 9,031 breast cancer cases investigated the association between ever-breastfeeding and breast cancer risk. The summary RR of breast cancer for the ever compared with never categories of breastfeeding was 0.613 (95% CI, 0.442–0.850) with high heterogeneity (I2=89.9%, p for heterogeneity=0.000) (Fig. 2).
Longest compared with shortest total durations of breastfeeding
Nineteen11–14,18–30 of the 27 studies assessed the association between duration of breastfeeding and risk of breast cancer. Fifteen of these studies found a significant protective association of some amount of extended duration of breastfeeding on breast cancer. The summary RR of breast cancer for the longest compared with shortest categories of breastfeeding was 0.471 (95% CI, 0.368–0.602) with high heterogeneity (I2=76.6%; pheterogeneity=0.000) (Fig. 2).
Meta-regression and subgroups analysis
As seen in Figure 2, evidence of heterogeneity (I2=87.5%, pheterogeneity=0.000) was found in the pooled results. In order to explore the moderate to high between-study heterogeneity found in the analysis, univariate meta-regression with the covariates of publication year, location where the study was conducted, study design (case-control or cohort), number of cases, and source of controls was performed. No significant findings were found in the above-mentioned analysis.
In stratified analysis by study design, the association was found in the case-control studies (summary RR=0.444; 95% CI, 0.362–0.546) but not in the cohort studies. In subgroup analyses for geographic locations, breastfeeding was significantly associated with the risk of breast cancer in Asia (summary RR=0.477; 95% CI, 0.359–0.635), Europe (summary RR=0.539; 95% CI, 0.357–0.814), and other countries (summary RR=0.580; 95% CI, 0.478–0.704). Subgroup analysis by sources of control suggested that significant associations were found both in population-based case-control studies (summary RR=0.453; 95% CI, 0.306–0.673) and hospital-based case-control studies (summary RR=0.440; 95% CI, 0.345–0.562). The detailed results are summarized in Table 2.
CI, confidence interval; RR, relative risk.
Influence analysis and publication bias
Influence analysis showed that no individual study had excessive influence on the association of breastfeeding and breast cancer risk. Egger's test (p=0.108) showed no evidence of significant publication bias between breastfeeding and breast cancer risk.
Discussion
The findings from this meta-analysis of epidemiologic studies indicated that ever breastfeeding had a reduced risk of breast cancer compared with never breastfeeding. The inverse association was also found for the longest compared with shortest categories of breastfeeding.
Several mechanisms have been proposed to explain the observed association as reviewed by other studies,37,38 and these include the following: (1) a reduced exposure to the cyclic hormones of reproductive life due to ovulatory suppression occurring with prolonged breastfeeding; (2) a protective effect from direct physical changes in the breast that accompany milk production; (3) a reduction in the concentrations of toxic organochlorines in the breast with increasing cumulative duration of breastfeeding; and (4) an expression of transforming growth factor-β, a hormonally regulated negative growth factor in human breast cancer cells, during breastfeeding. A protective effect associated with a longer duration of breastfeeding has been quite consistently reported in countries where the prevalence of prolonged breastfeeding is high39–42 ; these observations are generally consistent with our results.
Between-study heterogeneity is common in meta-analysis, 43 and exploring the potential sources of between-study heterogeneity is the essential component of meta-analysis. For breastfeeding and breast cancer risk, evidence of heterogeneity was found in the pooled results. The between-study heterogeneity might arise from publication year, study region, study design, and sources of controls. Thus, we used meta-regression to explore the causes of heterogeneity for covariates. However, no covariate having a significant impact on between-study heterogeneity for the above-mentioned covariates. Considering the pooled meta-analysis was fraught with the problem of heterogeneity, subgroup analyses by the type of study design, sources of controls, and geographic locations were performed to explore the source of heterogeneity. However, the between-study heterogeneity persisted in some subgroups, suggesting the presence of other unknown confounding factors. Breast cancer is a complex etiology and pathophysiology disease generated by the combined effects of genes and environment factors. Thus, other genetic and environment variables, as well as their possible interaction, may well be potential contributors to the heterogeneity observed.
The strengths of this meta-analysis included the large sample size of 13,907 cases and large number of participants. This sample size should have provided sufficient statistical power to detect the putative association between ever breastfeeding and the duration of breastfeeding with risk of breast cancer. In addition, our study considered several subgroups to evaluate heterogeneity.
Our study also has several limitations. First, as a meta-analysis of observational studies, it was prone to biases (e.g., recall and selection bias) inherent in the original studies. Cohort studies are less susceptible to bias than case-control studies because, in the prospective design, information on exposures is collected before the diagnosis of the disease. Although the results of the meta-regression showed no evidence of significant heterogeneity between subgroups, summary association estimates was different in subgroup analyses by study design. It is possible that a small number of cohort studies was included, and the relations reported by case-control studies may have been overstated as a result of recall or interviewer bias. In addition, some cohort studies provided detailed information of adjustment for confounders, whereas some early case-control studies adjusted for fewer factors. Thus, more large studies, especially prospective studies, are needed in the future.
A second limitation was that individual studies may have failed to control for potential confounders, which may have introduce bias in an unpredictable direction. Ever breastfeeding and a longer duration of breastfeeding are often associated with other hormone-dependent or reproductive factors, including lower levels of body mass index, 44 a lower prevalence of oral contraceptive use, 45 a higher parity number, and a lower prevalence of smoking. 46 Many, but not all, of the studies adjusted for potential confounding factors.
Third, significant heterogeneity and a possible publication bias must be considered. There was significant heterogeneity in the pooled analysis of ever breastfeeding and total breastfeeding duration. Despite the numerous subgroup and sensitivity analyses that were carried out, heterogeneity still existed in our study. To our knowledge, the category of duration of breastfeeding, especially the longest duration, differed between studies and may have contributed to the heterogeneity in results. However, few of the included studies reported how they categorized the duration of breastfeeding, and thus we hardly considered this point in the subgroup analysis and ruled out the heterogeneity thoroughly. Publication bias can be a problem in meta-analyses of published studies; however, we showed no statistical evidence of a publication bias in the meta-analysis.
In conclusion, findings from this meta-analysis suggest that breastfeeding, particularly a longer duration of breastfeeding, was inversely associated with risk of breast cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.