
Abstract
Abstract
Background:
Prepregnancy overweight/obesity can adversely affect breastfeeding initiation, but studies examining this association among different racial/ethnic groups of U.S. women are limited. This study used a large, nationally representative sample to assess racial/ethnic differences in breastfeeding noninitiation among U.S. women of different body mass index (BMI) classifications.
Materials and Methods:
This study analyzed data from the Pregnancy Risk Assessment Monitoring System, including 95,141 women who delivered a live, singleton baby from 2009 to 2011 and provided BMI and breastfeeding information. Prepregnancy BMI was categorized as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2). Breastfeeding initiation was reported as having ever breastfed after delivery (yes or no). Adjusted models, which included only potential confounders resulting in a 10% or greater change in estimate, generated adjusted odds ratios (AOR) and 95% confidence intervals (CI) for breastfeeding noninitiation. Analysis was stratified by race/ethnicity.
Results:
Compared with normal weight non-Hispanic white women, the odds of breastfeeding noninitiation were 17% and 25% higher among overweight (AOR=1.17, 95% CI=1.07–1.29) and obese (AOR=1.25, 95% CI=1.14–1.36) non-Hispanic white women, respectively. Among non-Hispanic black women, the odds of breastfeeding noninitiation were 29% higher only in obese women compared with normal weight non-Hispanic black women. No association was observed among Hispanic women or women of other races.
Conclusions:
Prepregnancy BMI is a significant predictor for breastfeeding noninitiation for non-Hispanic white and non-Hispanic black women. Further exploration of the differences underlying the association between prepregnancy BMI and breastfeeding behaviors among racial subpopulations of women in the United States is warranted.
Introduction
T
Despite this recommendation, one in five infants (20.1%) born in the United States has never been breastfed. 6 Maternal characteristics associated with lower rates of breastfeeding include younger age, low income, black race, and low educational attainment.7,8 For example, an analysis by the Centers for Disease Control and Prevention (CDC) found that in 2011, 81.1% of non-Hispanic white women initiated breastfeeding, whereas 61.6% of non-Hispanic black women initiated breastfeeding in the United States. 6 Recognizing breastfeeding noninitiation as a major public health issue, the U.S. Department of Health and Human Services set a national objective to increase the proportion of infants who are ever breastfed to 81.9% as part of its Healthy People 2020 initiative. 9
In addition to breastfeeding rates failing to meet national standards, more than half (54%) of women in the United States begin pregnancy overweight or obese. 10 Research has shown that overweight/obesity is linked not only to increased risk for medical complications such as preeclampsia and infant death, but also to poor maternal health behaviors such as breastfeeding discontinuation.11,12 Moreover, certain groups of women, such as non-Hispanic blacks, are at greater risk for overweight/obesity. 13 In 2012, 80% of non-Hispanic black women 20 years of age or older were overweight/obese compared with 60.3% of non-Hispanic white women. 14
To date, several studies, including systematic reviews, point to an inverse relationship between elevated prepregnancy body mass index (BMI) and breastfeeding outcomes, such that breastfeeding initiation decreases as prepregnancy BMI increases.11,15,16 However, few studies have assessed whether this trend holds true across different racial/ethnic groups of women in the United States. Most studies have targeted specific subpopulations of women of certain racial/ethnic groups or BMI classifications.17–20 One study by Liu et al. 18 reported that very obese (BMI≥35 kg/m2) non-Hispanic white women in South Carolina were less likely to breastfeed than normal weight women (adjusted odds ratio [AOR]=0.63, 95% confidence interval [CI]=0.42–0.94), but no association was found among black women. Indeed, there is a paucity of evidence examining racial differences beyond black and white, using a large, nationally representative sample of U.S. women.
To address this gap in the literature, this study uses data from the 2009–2011 national Pregnancy Risk Assessment Monitoring System (PRAMS) to examine the extent to which prepregnancy BMI is associated with postpartum breastfeeding noninitiation among different racial/ethnic groups of women in the United States.
Materials and Methods
This study analyzes data from PRAMS for 2009–2011 (n=112,358). This national surveillance examines mothers' attitudes, feelings, and behaviors before, during, and after their most recent pregnancy. 21 Using state birth certificate records as its sampling frame, PRAMS draws a random sample of women living in the United States with recent live births. Participating states typically oversample subpopulations such as minority women and high-risk births (e.g., low birth weight, preterm) and must achieve at least a 65% response rate to be included in the national PRAMS dataset. 21 The PRAMS questionnaire, administered by mail or phone, is typically completed 2–6 months after delivery. It consists of core items that are asked for all participants and additional questions that vary by state. The present study analyzes data from the core questionnaire, which is also linked to state birth certificate data. More information on the PRAMS methodology and questionnaire is available elsewhere. 21 Participants for this study include a representative sample of U.S. women who had a live, singleton birth. Women who delivered multiple births as well as those with missing information on the exposure (prepregnancy BMI) or outcome of interest (postpartum breastfeeding initiation) were excluded, resulting in a sample of 95,141 women (weighted n=4,919,333).
Maternal prepregnancy BMI was calculated based on participants' self-reported weight and height prior to pregnancy (in kg/m2). Participants were asked, “Just before you got pregnant with your new baby, how much did you weigh?” and “How tall are you without shoes?” Using classifications from the World Health Organization, prepregnancy BMI was categorized as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2). 22
For this analysis, postpartum breastfeeding initiation was operationally defined as having ever breastfed.23,24 Specifically, breastfeeding initiation was dichotomized as “yes” or “no” based on a survey item in the PRAMS core questionnaire that asked, “Did you ever breastfeed or pump milk to feed your new baby after delivery, even for a short period of time?” Women who responded “yes” were classified as “breastfeeding initiation,” whereas those who responded “no” were classified as “breastfeeding noninitiation.”
Maternal sociodemographic, behavioral, and health-related factors were examined as potential confounders. Sociodemographic factors included maternal age in years (≤19, 20–24, 25–29, 30–34, ≥35), race/ethnicity (non-Hispanic white, non-Hispanic black, non-Hispanic other, Hispanic), education in years (0–11, 12, 13–15, ≥16), marital status (married versus not married), household income level (<$20,000, $20,000–$34,999, $35,000–$49,999, ≥$50,000), and place of residence (urban versus rural).
Factors related to access to care and utilization of services included insurance used to pay for prenatal care (private or health maintenance organization, Medicaid, none, other, multiple), adequacy of prenatal care utilization (inadequate, intermediate, adequate, adequate plus), and participation in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) program during pregnancy (yes versus no).
Maternal health behaviors included smoking and drinking in the 3 months prior to pregnancy (yes versus no), use of a multivitamin, prenatal vitamin, or folic acid during the month before pregnancy (none, one to three times a week, four to six times a week, every day), and exercising 3 or more days of the week during the 12 months before pregnancy (yes versus no). Maternal health and psychosocial factors included gestational weight gain in pounds (<12, 12–15, 16–25, 26–30, ≥31), parity (primiparous versus multiparous), delivery type (vaginal versus cesarean section), experiencing intimate partner violence prior to pregnancy (yes versus no), stressful life events during the 12 months before delivery (0, 1–2, 3–5, ≥6), and pregnancy intention (intended versus not intended). Women who reported a diagnosis of chronic diabetes mellitus prior to pregnancy, gestational diabetes, high blood pressure, hypertension (including pregnancy-induced hypertension), preeclampsia, toxemia, or placental problems during pregnancy were categorized as having pregnancy complications (any versus none). Women who reported feeling down, depressed, sad, hopeless, or slowed down after childbirth were classified as having postpartum depressive symptoms (yes versus no).
Descriptive statistics including weighted frequencies and weighted percentages were generated to assess the distribution of maternal characteristics by prepregnancy maternal BMI and postpartum breastfeeding noninitiation. Logistic regression models were used to obtain odds ratios (ORs) and 95% CIs for breastfeeding noninitiation. Interaction was tested to examine if gestational weight gain was a significant effect modifier. To adjust for confounding, a forward selection process adding factors to the model one at a time was used. Variables were retained in parsimonious models if their addition resulted in a 10% or greater change in estimate for the association between prepregnancy maternal BMI (normal weight as referent group) and breastfeeding noninitiation. 25 All unadjusted and adjusted analyses were stratified by race/ethnicity. Analyses were conducted using SAS version 9.4 software (SAS Institute, Cary, NC) to account for the complex survey design of PRAMS. This study was approved by the Virginia Commonwealth University Institutional Review Board.
Results
The prevalence of breastfeeding initiation among the study population was 83.2%. Half of all women were normal weight prior to pregnancy (50.4%), whereas 24.1% were overweight, 21.2% were obese, and 4.3% were underweight. Almost two-thirds of the women were non-Hispanic white (60.6%), 17.9% Hispanic, 13.5% non-Hispanic black (13.5%), and 8.0% non-Hispanic other race(s). The majority were 20–29 years old (52.1%) and married (61.4%) and had more than high school education (58.3%). Over one-third (36.8%) earned $50,000 or more (Table 1).
All numbers are weighted.
BMI, body mass index; IPV, intimate partner violence; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
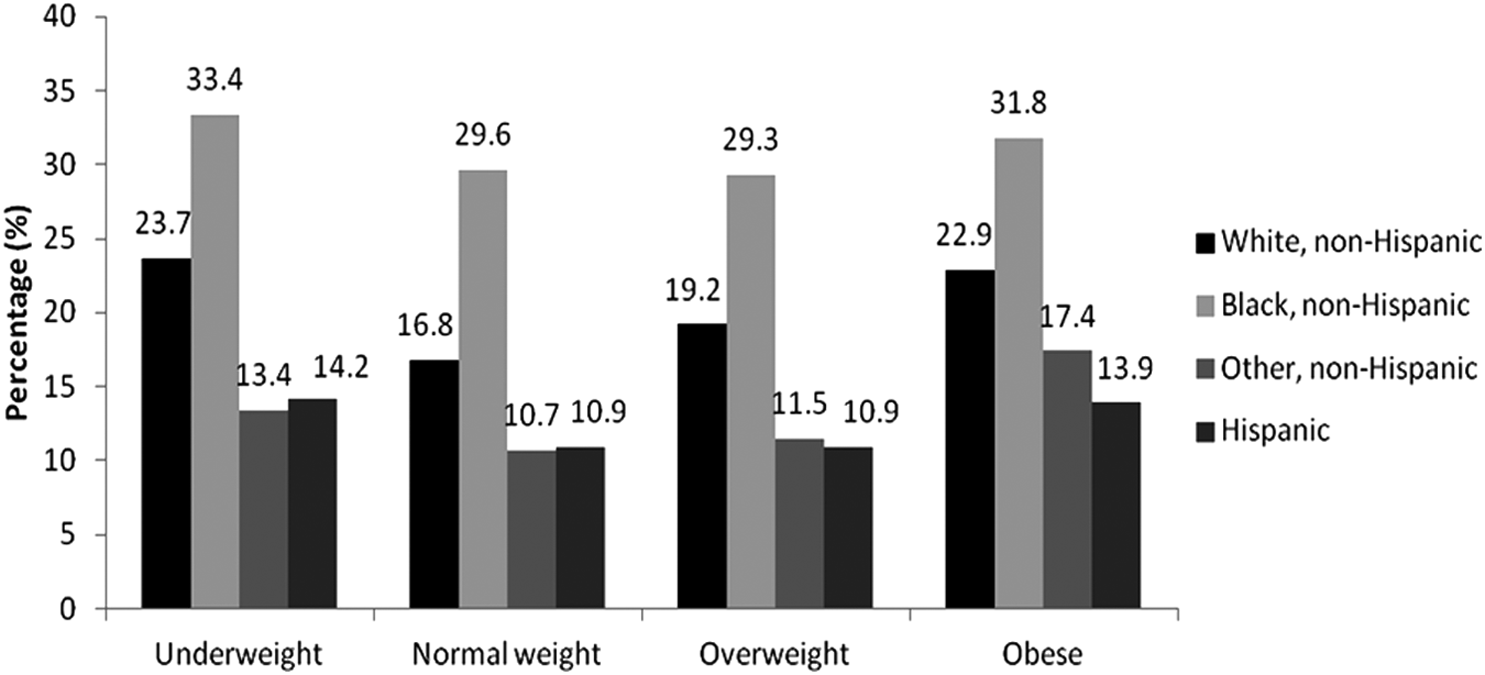
The prevalence of breastfeeding noninitiation was highest among women who were non-Hispanic black (30.3%), less than 20 years of age (30.1%), had less than high school education (29.5%), and earned less than $20,000 (27.7%) (Table 2). The unadjusted analysis shows a statistically significant association between breastfeeding noninitiation and age, education, race/ethnicity, marital status, income, place of residence, WIC receipt, smoking, multivitamin use, exercise, pregnancy complications, delivery type, parity, unintended pregnancy, stressful life events, and intimate partner violence. Figure 1 depicts racial differences in breastfeeding noninitiation by BMI categories. The data show that non-Hispanic black women had the highest breastfeeding noninitiation rate across all BMI groups.
Prevalence of breastfeeding noninitiation by maternal race/ethnicity and prepregnancy body mass index.
BMI, body mass index; CI, confidence interval; IPV, intimate partner violence; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Logistic regression analyses examining the association between prepregnancy BMI and breastfeeding noninitiation among all women (prior to stratification) are shown in Table 3. Compared with normal weight women, the odds of breastfeeding noninitiation were higher among women who were underweight (crude OR [COR]=1.42, 95% CI=1.24–1.62), overweight (COR=1.14, 95% CI=1.06–1.23), and obese (COR=1.46, 95% CI=1.35–1.57). The estimates for underweight and obese women were attenuated but remained statistically significant after adjusting for maternal education. Compared with normal weight women, the odds of breastfeeding noninitiation were highest among obese (AOR=1.27, 95% CI=1.18–1.37) followed by underweight (AOR=1.22, 95% CI=1.07–1.40) and overweight (AOR=1.14, 95% CI=1.18–1.37) women. There was no interaction between gestational weight gain and prepregnancy BMI on breastfeeding initiation (p>0.44).
AOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; COR, crude odds ratio.
Bolded estimates indicate statistically significant results.
Logistic regression analyses examining the association between prepregnancy BMI and breastfeeding noninitiation stratified by maternal race/ethnicity are shown in Table 4.
Adjusted model controlling for maternal education.
Adjusted model controlling for Special Supplemental Nutrition Program for Women, Infants, and Children participation.
Adjusted model controlling for urban/rural and maternal education.
Adjusted model controlling for urban/rural, maternal age, and adequacy of prenatal care utilization.
Adjusted model controlling for maternal age.
Adjusted model controlling for urban/rural and postpartum depressive symptoms.
Adjusted model controlling for urban/rural.
Adjusted model controlling for household income, adequacy of prenatal care utilization, and prepregnancy smoking.
Adjusted model controlling for urban/rural and intimate partner violence.
AOR, adjusted odds ratio; BMI, body mass index; CI, confidence interval; COR, crude odds ratio.
Bolded estimates indicate statistically significant results.
Non-Hispanic white
Although the unadjusted analysis showed higher odds of breastfeeding noninitiation among non-Hispanic white underweight women (COR=1.54%, 95% CI=1.30–1.82), the estimate lost its statistical significance after adjusting for maternal education (Table 4). Among overweight non-Hispanic white women, the odds of breastfeeding noninitiation were 17% higher compared with normal weight non-Hispanic white women (COR=1.17, 95% CI=1.07–1.29). None of the confounding factors examined changed the estimate.
In the unadjusted analysis, the odds of breastfeeding noninitiation among obese non-Hispanic white women were 47% higher compared with normal BMI non-Hispanic white women (OR=1.47, 95% CI=1.34–1.61). After controlling for receipt of WIC services, the odds of breastfeeding noninitiation were attenuated. The odds of breastfeeding noninitiation were 25% higher among obese women (AOR=1.25, 95% CI=1.14–1.37) compared with normal weight non-Hispanic white women.
Non-Hispanic black
The unadjusted analysis showed no statistically significant association between BMI and breastfeeding noninitiation (Table 4). However, after adjusting for maternal education and place of residence (urban/rural), the association became significant for obese non-Hispanic black women. Compared with their normal weight counterparts, obese non-Hispanic black women had a 29% higher odds of noninitiation (AOR=1.29, 95% CI=1.10–1.51).
Non-Hispanic other
The unadjusted analysis showed that obese non-Hispanic women of other race(s) had a 75% higher odds of breastfeeding noninitiation compared with their normal weight counterparts (OR=1.75, 95% CI=1.29–2.37) (Table 4). However, the association lost statistical significance when adjusted for household income, adequacy of prenatal care utilization, and prepregnancy smoking (AOR=0.98, 95% CI=0.71–1.36).
Hispanic
The unadjusted analysis showed higher odds of noninitiation among Hispanic obese women (OR=1.32, 95% CI=1.02–1.71) (Table 4). However, the association lost statistical significance when adjusted for place of residence (AOR=1.14, 95% CI=0.80–1.61).
Discussion
Findings from this study demonstrate the majority of women in the United States who gave birth to a live, singleton baby from 2009 to 2011 initiated breastfeeding. This exceeds the Healthy People 2020 national goal of 81.9% of infants who are ever breastfed. 9 This promising finding should be interpreted with caution, as it is higher than other recent estimates such as the CDC's National Immunization Survey, which reported 79.2% of infants born in 2011 were ever breastfed. 6 The discrepancy in results may be due to differences in study design and study population composition. Unlike the current study, the CDC analysis included women who gave birth to multiples, who may face more barriers to initiate breastfeeding. 26
Findings from the current study also demonstrate that breastfeeding disparities continue to exist, as the risk for breastfeeding noninitiation was considerably higher among women who were non-Hispanic black, less educated, younger, or a WIC or Medicaid recipient or who smoked. In particular, this study showed that compared with other racial/ethnic groups, non-Hispanic black women were least likely to initiate breastfeeding. Therefore, interventions to promote breastfeeding initiation, duration, and exclusivity should continue to target women who self-identify as non-Hispanic black in order to reduce the significant racial/ethnic gap in breastfeeding.
Non-Hispanic white women differed from other racial/ethnic groups in that they were the only group in which both prepregnancy overweight and obesity increased the odds of breastfeeding noninitiation. Two studies in the United States reported increased odds of breastfeeding noninitiation among very obese 18 and obese 27 non-Hispanic white women, but this study is among the first to indicate that prepregnancy overweight can also affect breastfeeding initiation.
Although this study found greater odds of breastfeeding noninitiation among obese non-Hispanic black women, not all previous studies have reported this to be true. In two studies, prepregnancy obesity was not associated with breastfeeding initiation among black women.18,28 Moreover, this study did not find overweight non-Hispanic black women to differ in breastfeeding initiation compared with normal weight women. This is not consistent with other studies that have reported overweight non-Hispanic black women to be more likely to initiate breastfeeding than normal weight women. 24 However, differences in study design may have contributed to these conflicting results. Although the current study used a large, nationally representative sample of women, previous studies have been limited to smaller groups living in specific settings in the United States18,27,28 and controlled for different potential confounding factors. Having afforded stronger study design, the current study's findings provide more robust evidence that prepregnancy obesity, but not prepregnancy overweight, is adversely associated with breastfeeding initiation among non-Hispanic black women in the United States. The racial difference in prepregnancy obesity but not overweight between non-Hispanic white women and non-Hispanic black women may contribute to conflicting findings in the literature.
Another novel finding from this study was that, overall, underweight women had a higher prevalence of breastfeeding noninitiation compared with normal weight women, which supports growing evidence in the literature.19,27,29 However, research findings on racial/ethnic differences have been inconsistent. In the current study, within racial/ethnic groups of women, no differences in breastfeeding initiation were found between underweight and normal weight women. In contrast, Thompson et al. 19 reported underweight non-Hispanic black and Hispanic women to be less likely to initiate breastfeeding compared with normal weight women, whereas Kachoria and Oza-Frank 27 reported underweight non-Hispanic white women were less likely to initiate breastfeeding than normal weight non-Hispanic white women. In Italy, researchers found that underweight women were less likely to initiate breastfeeding, but analyses did not include maternal race/ethnicity. 29 In light of these inconsistent findings and the fact that the association between prepregnancy underweight and breastfeeding initiation is relatively unknown, further research is needed.19,27,29
Current research posits that the link between elevated prepregnancy BMI and breastfeeding may be attributable to a woman's biological, physical, or psychosocial characteristics.11,30 For example, obese women who have greater amounts of adipose tissue may have larger breasts or flattened nipples, which can hinder infant latching. 31 Psychological barriers to breastfeeding noted in the literature include the fear of pain associated with breastfeeding,32,33 fear of social isolation,33,34 and low self-efficacy. 34 In addition, some studies have shown obese women have lower intentions to breastfeed, a significant predictor for initiation,29,35–37 whereas others have shown this to be untrue. 38
Considering that maternal race/ethnicity is a social construct, 39 racial/ethnic differences in breastfeeding behaviors observed among this population may be indicative of the influence of sociocultural factors. Cultural barriers and beliefs regarding breastfeeding among non-Hispanic black women have been previously reported in qualitative studies; these include the use of formula as a norm 34 and the taboo against breastfeeding in public.33,34 Cultural differences in perceptions of weight and attractiveness may also play a role in breastfeeding disparities. In a study among obese women, black women described more feelings of pride and positive body image than white women, who described more feelings of depression and shame. 40 This may suggest postpartum breastfeeding noninitiation, as it relates to body image, may be less salient for black women.
Contrary to previous research,17,28 this study did not find prepregnancy BMI to be a significant, independent predictor for breastfeeding initiation among non-Hispanic women of other race(s) or Hispanic women. There are several possible explanations for these findings. First, the inherent racial/ethnic heterogeneity of women categorized as “other” may mask important cultural, racial, or physiological differences that could affect breastfeeding outcomes among this diverse group of women. The fact that prepregnancy BMI had no effect on breastfeeding initiation for this group and Hispanics in the study population suggests that there may be other factors besides biological reasons that may affect breastfeeding initiation. In fact, among ethnic minorities and generation of immigrants, exclusivity and other infant feeding behaviors may be more of an issue than breastfeeding initiation. For example, in a recent analysis of exclusive breastfeeding among Asian and Native Hawaiian and other Pacific Islander subgroups, a study reported that compared with white women, individual subgroups, such as Filipino and Japanese women, had significantly lower prevalence ratios of exclusive breastfeeding at least 8 weeks after delivery. 41 Findings from the study emphasize the importance of disaggregating racial populations and the need to investigate breastfeeding behaviors within smaller racial/ethnic subgroups of childbearing women in the United States.
The lack of association between prepregnancy BMI and breastfeeding noninitiation among Hispanic women in the current study could also reflect the “Hispanic paradox,” a common epidemiological pattern in which Hispanic and Latino populations in the United States have better health behaviors and outcomes than white populations, despite being low income and less educated. 42 Findings from the current study support a common theory that Hispanic women who are less acculturated to U.S. cultural beliefs and practices may be more likely to breastfeed compared with Hispanic women who are more acculturated. 43 For example, Ahluwalia et al. 44 reported women who self-identified as Hispanic and responded to the PRAMS survey in English (considered “more acculturated”) had lower odds of breastfeeding initiation than those who responded in Spanish (“less acculturated”). Although BMI was not associated with breastfeeding initiation among Hispanic women in this study, other studies have shown obesity to adversely affect infant feeding practices within this population.17,28 Therefore, Hispanic women should not be excluded in efforts to support continued and exclusive breastfeeding.
To the authors' knowledge, this is one of the first studies to closely examine the association between prepregnancy BMI and postpartum breastfeeding noninitiation within various racial/ethnic strata among a large, nationally representative sample of U.S. women. Because the PRAMS dataset involves a statistically robust sample size and multistaged sampling, findings from the current study can be generalizable to women of childbearing age with recent live births in participating states. It is important that the current study makes a valuable contribution to the literature by demonstrating prepregnancy BMI is a significant predictor for breastfeeding noninitiation for certain racial groups of women but not others, even after controlling for important maternal characteristics known to affect breastfeeding initiation. Findings from this study highlight the need for further exploration of the underlying mechanisms of breastfeeding behaviors and outcomes among smaller racial/ethnic subpopulations of U.S. women and suggest that breastfeeding initiation is largely influenced by sociocultural factors.
Despite its strengths, this study was not without its limitations. First, both prepregnancy BMI and postpartum breastfeeding initiation were self-reported by new mothers and therefore were subject to recall bias. However, self-reported prepregnancy weight and height have been shown to be more complete and consistent with clinical records. 45 Second, this study did not quantify the length of time that a mother breastfeeds or distinguish exclusive breastfeeding from other infant feeding practices, which would provide a more in-depth understanding of postpartum breastfeeding behaviors among U.S. women. Nevertheless, breastfeeding initiation is a necessary precursor to breastfeeding duration, and any breastfeeding is associated with improved health outcomes. 5 Furthermore, because of its cross-sectional design, this analysis cannot ascertain a causal relationship between prepregnancy BMI and postpartum breastfeeding noninitiation. However, the operationalization of breastfeeding initiation as “Did you ever breastfeed or pump milk to feed your new baby after delivery, even for a short period of time?” suggests some degree of directionality from prepregnancy BMI. Lastly, women who had multiple births were excluded from this study, but this deliberate restriction is consistent with the literature15,17,19,27 and helps to control for possible confounding bias because women who give birth to multiples may face more challenges that in turn affect breastfeeding outcomes. 26
Conclusions
The results from the current study indicate that the effect of prepregnancy BMI on breastfeeding initiation may vary by maternal race/ethnicity, such that non-Hispanic white women who are overweight or obese prior to pregnancy and non-Hispanic black women who are obese are less likely to initiate breastfeeding. In contrast, prepregnancy BMI was not significantly associated with breastfeeding noninitiation among Hispanic women or non-Hispanic women of other race(s). Therefore, in working with pregnant non-Hispanic white and black women who present with obesity, healthcare providers should consider their unique challenges to breastfeeding initiation and the fact that they may benefit from additional technical or interpersonal support. Similarly, future breastfeeding interventions should continue to target all women to ensure breastfeeding initiation, continuation, and exclusivity. In light of inconsistent findings in the literature, more research is needed to explore the effect of maternal race/ethnicity on prepregnancy BMI and breastfeeding initiation in order to better understand the mechanisms behind racial/ethnic disparities in breastfeeding outcomes in the United States.
Footnotes
Acknowledgments
This study is partially supported by grants from the Agency for Healthcare Research and Quality (1R01HS021504-01A1) and the Health Resources and Services Administration (5H49MC00124). We would like to acknowledge the PRAMS Working Group: Alabama—Izza Afgan, MPH; Alaska—Kathy Perham-Hester, MS, MPH; Arkansas—Mary McGehee, PhD; Colorado—Alyson Shupe, PhD; Connecticut—Jennifer Morin, MPH; Delaware—George Yocher, MS; Florida—Avalon Adams-Thames, MPH, CHES; Georgia—Chinelo Ogbuanu, MD, MPH, PhD; Hawaii—Emily Roberson, MPH, PhD; Illinois—Theresa Sandidge, MA; Iowa—Sarah Mauch, MPH; Louisiana—Amy Zapata, MPH; Maine—Tom Patenaude, MPH; Maryland—Diana Cheng, MD; Massachusetts—Emily Lu, MPH; Michigan—Cristin Larder, MS; Minnesota—Judy Punyko, PhD, MPH; Mississippi—Brenda Hughes, MPPA; Missouri—Venkata Garikapaty, MSc, MS, PhD, MPH; Montana—JoAnn Dotson; Nebraska—Brenda Coufal; New Hampshire—David J. Laflamme, PhD, MPH; New Jersey—Lakota Kruse, MD; New Mexico—Eirian Coronado, MPH; New York—Anne Radigan-Garcia; New York City—Candace Mulready-Ward, MPH; North Carolina—Kathleen Jones-Vessey, MS; North Dakota—Sandra Anseth; Ohio—Connie Geidenberger, PhD; Oklahoma—Alicia Lincoln, MSW, MSPH; Oregon—Kenneth Rosenberg, MD, MPH; Pennsylvania—Tony Norwood; Rhode Island—Sam Viner-Brown, PhD; South Carolina—Mike Smith, MSPH; Texas—Rochelle Kingsley, MPH; Tennessee—David Law, PhD; Utah—Lynsey Gammon, MPH; Vermont—Peggy Brozicevic; Virginia—Marilyn Wenner; Washington—Linda Lohdefinck; West Virginia—Melissa Baker, MA; Wisconsin—Katherine Kvale, PhD; Wyoming—Amy Spieker, MPH; CDC PRAMS Team, Applied Sciences Branch, Division of Reproductive Health.
Disclosure Statement
No competing financial interests exist.