
Abstract
Abstract
Background:
Women who are overweight or obese are at risk for maternal and neonatal medical complications, including macrosomia (birth weight ≥4,000 g), that may contribute to breastfeeding initiation failure. This study examined factors associated with breastfeeding initiation among obese women without diabetes who delivered macrosomic infants.
Study Design and Methods:
A retrospective chart review was conducted from 2008 to 2011. Based on prepregnancy body mass index (in kg/m2), women were classified as normal (18–24.9), overweight (25–29.9), obese (30–34.9), very obese (35–39.9), and extremely obese (≥40). Intention to breastfeed was ascertained prenatally, and breastfeeding initiation was defined if at discharge ≥50% of the infant feedings were breastmilk.
Results:
Twenty-nine percent of the population was overweight, 23% obese, 14% very obese, and 12% extremely obese. Intention to breastfeed was similar among normal-weight, overweight, obese, and very obese women but was significantly lower for those who were extremely obese (p<0.05). Breastfeeding initiation was 75% for normal-weight, 72% for overweight, 71% for obese, 66% for very obese, and 53% for extremely obese women (p<0.05). Among women who intended to breastfeed, breastfeeding initiation was uniformly high: 94% for normal-weight, 93% for overweight, 95% for obese, 92% for very obese, and 87% for extremely obese women.
Conclusions:
Intention to breastfeed as well as breastfeeding initiation was significantly lower for extremely obese women. Lack of intention to breastfeed declared during the antepartum period by extremely obese women highlights a need as well as an opportunity for intervention.
Background
D
This study examined factors associated with intention to breastfeed and breastfeeding initiation among overweight, obese, very obese, and extremely obese nondiabetic mothers of macrosomic infants.
Subjects and Methods
This retrospective chart review was approved by the Institutional Review Board of Wexner Medical Center at The Ohio State University. Hard copies and electronic medical records were reviewed. The study population included women without gestational diabetes (GDM) or pregestational diabetes (PGDM) 11 and their macrosomic infants born between 2008 and 2011 at The Ohio State University Wexner Medical Center. Pregnancies delivered at ≥37 weeks of gestation and not affected by major or fatal malformations were included. Obesity was defined as a BMI of 18.5–24.9 kg/m2 (normal), 25–29.9 kg/m2 (overweight), 30–34.9 kg/m2 (obese), 35–39.9 kg/m2 (very obese), and ≥40 kg/m2 (extremely obese). 12 Upon arrival of women to the Labor and Delivery suite, their feeding preference for their infants (breastfeeding or formula feeding) was ascertained.
Cesarean delivery was offered to nondiabetic women with an estimated fetal weight of ≥4,500 g. 11 Shoulder dystocia was diagnosed if, following delivery of the fetal head, additional obstetrical maneuvers other than gentle downward traction were required. 11 Birth trauma was defined by the occurrence of limb fractures or brachial plexus injury during delivery.
Depending on the condition of the mother and her infant, maternal–infant interactions (holding, skin-to-skin contact, breastfeeding, and postpartum visitation) were encouraged. Birth weight was determined using an electronic scale calibrated before each measurement. Macrosomia was defined as birth weight ≥4,000 g irrespective of gestational age. Crown–heel length and head circumference were measured using standard pediatric techniques. Weight/length ratio was calculated for all infants, with asymmetry defined by a weight/length ratio above the 90th percentile for gestational age and gender. 13
Per our institutional guidelines, symptomatic macrosomic infants are transferred directly from the delivery room to the neonatal intensive care unit (NICU). 9 Indications for NICU admission include respiratory distress (respiratory distress syndrome and transient tachypnea of the newborn), prematurity (severe hypotonia and poor sucking behavior), perinatal asphyxia, birth trauma, and hypoglycemia requiring intravenous dextrose treatment. Asymptomatic macrosomic infants born to nondiabetic mothers are transferred to the well baby nursery, where they are fed early and monitored for hypoglycemia. 9
Screening for hypoglycemia (blood glucose level <40 mg/dL) was done via serial point-of-care testing (Accu-Chek®; Roche Diagnostics, Indianapolis, IN) starting by the first hour of life and prior to the first feeding. 14 Infants in the well baby nursery with hypoglycemia were breastfeeding or given formula. Those with repeated low blood glucose values were treated with intravenous dextrose (4–6 mg/kg/minute). All infants admitted to the NICU were either fed or started on intravenous dextrose. Breastfeeding was defined as initiated if, at the time of discharge, the infant was exclusively breastfeeding or was receiving ≥50% of the feedings directly from the breast or by expressed breastmilk. Due to the study design, no follow-up information was available on infant feeding practices beyond hospital discharge.
Statistical analysis
Comparisons between groups and subgroups of patients were made with Student's t test for continuous variables and chi-squared or Fisher's exact test for categorical variables. Univariate and multivariate logistic regression analyses were used to ascertain the strength of association of maternal variables (race, education, primiparity, BMI, smoking, mode of delivery, breastfeeding intention) and neonatal variables (gestational age, birth weight, gender, admission to the NICU) with breastfeeding initiation. Significance was established at a p value of ≤0.05.
Results
Our study population consisted of 736 nondiabetic women who delivered macrosomic infants. Demographic and clinical maternal information is presented in Table 1. Twenty-two percent of the women had normal prepregnancy weight, whereas 29% were overweight, 23% were obese, 14% were very obese, and 12% were extremely obese. Mean age at delivery (29 years), age ≤30 years (60%) and ethnic distribution (approximately 66% white, 15% black, 10% Hispanic, and 9% African, Asian, or other) were similar among normal-weight, overweight, and obese women. Very obese women were more often white, whereas women who were extremely obese were more often black. There were significant differences in level of education, as 63% of women of normal weight had completed college or postgraduate studies, whereas only 28% of the extremely obese group did so.
Data are number of women (%) or mean±standard deviation values, as indicated.
Significant p values were calculated by achi-squared or bKruskal–Wallis test.
BMI, body mass index; NS, not significant.
Mode of delivery produced remarkable differences among the groups: vaginal deliveries declined steadily from 80% among women of normal BMI to 43% among those who were extremely obese. Conversely, cesarean delivery increased from 20% to 57% from normal-weight to extremely obese women. Repeat cesarean deliveries occurred twice as often among overweight, obese, very obese, and extremely obese than among normal-weight women. In contrast, primary cesarean deliveries were more common among women of normal BMI. Indications for primary cesarean deliveries were similar across the groups and included failure of labor to progress, breech presentation, suspected macrosomia, and fetal distress. Length of hospital stay was reduced (2.5±2 days) for women in the normal-weight group compared with women in the overweight, obese, and very obese groups. The longest hospitalization (2.9±1 days) was documented for women in the extremely obese group.
Neonatal outcomes
Thirteen of the 736 infants (1.6%) were born at 37 weeks gestational age, and three infants (0.4%) were born at 42 weeks gestational age, whereas the remaining 720 (98%) were born at 38–41 weeks gestational age (Table 2). Four hundred ninety of the 736 (67%) infants were male. Weight/length ratio (7.8±0.3) values were similar among the different categories of maternal weight, but the prevalence of asymmetric growth was lower among infants of normal-weight women (78%) and higher among those of very obese (93%) and extremely obese women (84%). However, there was no correlation between asymmetric growth and hypoglycemia in any of the groups of women.
Data are number of infants (%) or mean±standard deviation values, as indicated.
Significant p values were calculated by aKruskal–Wallis or bchi-squared test.
BMI, body mass index; GA, gestational age; NICU, neonatal intensive care unit; NS, not significant; RDS/TTNB, respiratory distress syndrome/transient tachypnea of the newborn.
One-minute Apgar scores of ≤5 occurred for 29 of 736 (4%) infants, and persistent low scores at 5 minutes were observed in only two infants. Low and normal Apgar scores were distributed evenly in all weight groups. Six hundred eighty of 736 infants (92%) were transferred from the delivery room to the well baby nursery, whereas 56 (8%) were transferred directly to the NICU. The most common admission diagnosis was respiratory distress (43%).
Shoulder dystocia affected 70 out of 456 (15%) of infants born vaginally. Six of these infants experienced limb fractures, and four suffered brachial plexus injury. Only four of the 10 infants (25%) with birth trauma required admission to the NICU. All 10 of these infants recovered without sequelae.
One hundred eleven (15%) of the 736 infants developed hypoglycemia; 85% of them were corrected with oral feedings, whereas the remaining 15% required temporary intravenous dextrose treatment. The number of infants who required intravenous treatment was similar across the different groups of women. Seventy percent of the 111 hypoglycemia episodes consisted of single low glucose values. Except for gestational age and length of hospitalization, all of the above-described neonatal outcomes were distributed evenly across the maternal weight groups. Length of hospital stay was longer among infants born to extremely obese women compared with those in the normal-weight and overweight groups. Ninety-eight percent of infants across the maternal weight categories were discharged home simultaneously with their mothers.
Breastfeeding intention
Intention to breastfeed was higher among normal-weight (80%), overweight (79%), obese (75%), and very obese (73%) women than among extremely obese (61%) women (Fig. 1). Comparisons between very obese and extremely obese women who intended to breastfeed and those who intended to feed formula showed that the former were older (29±5 years versus 26±6 years; p<0.001) and were more likely to be college graduates (52% versus 16%; p<0.001). Seventy-two percent of white very obese and extremely obese women intended to breastfeed in contrast to only 51% of their black counterparts (p=0.02).
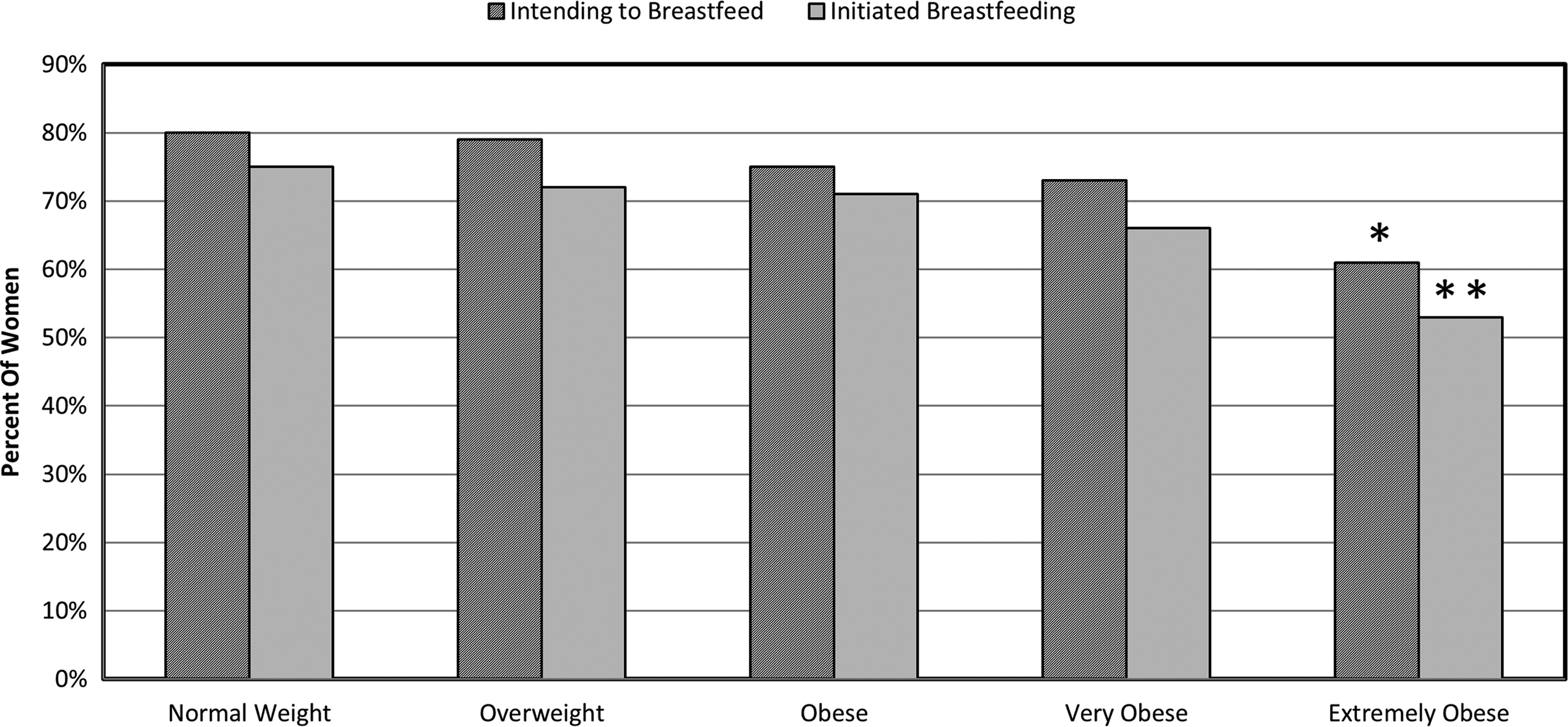
Percentage of women in each prepregnancy weight category who intended to breastfeed and those who within each group initiated breastfeeding. By chi-squared test, *p<0.01, **p=0.008 compared with normal weight.
Breastfeeding initiation
At the time of hospital discharge, none of the 182 women who intended to feed formula changed their mind. Of the 554 women who intended to breastfeed, 511 (92%) initiated breastfeeding. Stratification of data showed that breastfeeding initiation was inversely related to prepregnancy BMI (Fig. 1). Breastfeeding initiation was similar for normal-weight (75%), overweight (72%), obese (71%), and very obese (66%) women but was significantly lower for extremely obese (53%) women. It is remarkable that among women who intended to breastfeed, breastfeeding initiation was uniformly high: 94% for normal-weight, 93% for overweight, 95% for obese, 92% for very obese, and 87% for extremely obese women. No significant relationship between breastfeeding initiation and parity or cesarean delivery was noted. Older and more educated women were more likely to initiate breastfeeding, whereas smokers and very and extremely obese women were less likely. Odds of breastfeeding initiation were higher for nonsmokers (odds ratio=2.28; 95% confidence interval, 1.15–4.52; p<0.01), for white compared with black women (odds ratio=2.13; 95% confidence interval, 1.31–3.44; p=0.002), and for college graduates compared with those with ≤11th grade education (odds ratio=12.2; 95% confidence interval, 6.73–22.46; p<0.001).
The logistic regression models were analyzed for each of the five prepregnancy BMI groups. Statistically nonsignificant variables (mothers' age, primiparity, and mode of delivery) were excluded from the models (Table 3). Across all weight groups, higher level of education was associated with a greater likelihood of initiating breastfeeding. Important predictors of initiation among overweight women (besides their level of education) were being white, a nonsmoker, and having an infant admitted to the regular nursery. In obese women, relevant predictors of breastfeeding initiation were Hispanic race and higher levels of education.
Significant difference.
CI, confidence interval; NICU, neonatal intensive care unit; NS, not significant; OR, odds ratio; PG, postgraduate.
Discussion
In terms of intention to breastfeed and breastfeeding initiation, overweight, obese, and very obese women who delivered macrosomic infants had similar rates compared with normal-weight women. In contrast, extremely obese women had a lower intention to breastfeed with a consequent decrease in breastfeeding initiation. Among traditional factors known to affect breastfeeding intention, extremely obese women were younger and more often African American and less educated than their overweight, obese, and very obese counterparts.
Obesity and diabetes, common complicating factors in pregnancies, are causally related to fetal and neonatal macrosomia.11,15–17 The strict definition of macrosomia based on birth weight (≥4,000 g, ≥4,500 g) alone is variable, but whatever definition is used, the incidence of macrosomia and its potential morbidities are well known.4,5,11 In the United States approximately 500,000 macrosomic infants are born every year, with 90% of their mothers being nondiabetic.4,13,18 Maternal characteristics associated with macrosomic infants born to women without diabetes include obesity, age, excessive weight gain during pregnancy, multiparity, and advanced gestation, as well as genetic predisposition.19–21
In our large cohort of women without diabetes who delivered macrosomic infants, over one-fourth were overweight, and approximately half were either obese, very obese, or extremely obese. Regardless of the mothers' prepregnancy BMI, macrosomia increases the risk of complications during labor and delivery.4,15,17,18 The odds of both repeat and primary cesarean delivery increases in direct relation to a woman's prepregnancy BMI. Although the incidence of vaginal deliveries decreases, complications such as shoulder dystocia, perinatal asphyxia, and birth injury exist.19–23 These and other neonatal complications common among macrosomic infants (respiratory distress, hypoglycemia, and admission to NICU) were also present in our study population. The incidence of maternal and neonatal complications among macrosomic infants born to nondiabetic women reported here is similar to that reported in the literature.19–23 This is relevant to our study because all maternal and neonatal morbidities described above have been known to influence breastfeeding initiation.8,9,23,24
The influences of obesity on breastfeeding initiation and duration have been well recognized.1,2,24 Most studies, however, have defined as obese those women with a prepregnancy BMI of >30 kg/m2 and often include women with diabetes. Considering that maternal and neonatal morbidities increase in direct relation to the prepregnancy BMI and to the birth weight of the infant,1,4,17 we elected to study breastfeeding intention and breastfeeding initiation among obese, very obese, and extremely obese women who delivered macrosomic infants separately.
Recently we reported on breastfeeding intention of obese and very obese women with five distinct comorbidities (392 with PGDM, 8 303 with GDM, 9 170 women with GDM and PGDM who delivered macrosomic infants, 23 and 281 with preeclampsia 25 ). The prevalence of obese women (ranging from 20% to 30%) was similar across these groups. On the other hand, very obese (defined by a BMI of >35 kg/m2) women constituted 30% of the preeclampsia group, 26% of the GDM group, 51% of the PGDM group, and 55% of all diabetics who delivered macrosomic infants. Breastfeeding intention among very obese women in those five groups ranged from 71% to 79% and was similar to that of the very obese women reported here. Our data also revealed that except for extremely obese women, those who intended to breastfeed were somewhat older, mostly primiparous, highly educated, and white, whereas those who did not intend to breastfeed were often African American and smokers and had a lower level of education.6,26,27
Using Pregnancy Risk Assessment Monitoring System data from South Carolina, Liu et al. 1 determined that women who were obese (BMI 30–34.9 kg/m2) and very obese (BMI ≥35 kg/m2) were less likely to initiate and maintain breastfeeding than their normal-weight counterparts. Similarly, Krause et al. 2 concluded that very obese women also had difficulties with breastfeeding and may require additional encouragement to initiate and to continue breastfeeding. In contrast, Gaudet et al. 5 studied neonatal outcomes and breastfeeding among 249 extremely obese women and reported a breastfeeding initiation rate of 85% compared with 92% for women of normal weight; they concluded that extreme obesity did not appear to influence intent or breastfeeding initiation. The discrepancy of their results with current reports1,2,24 as well as with the data presented here may be explained by the definition of breastfeeding as any attempt to nourish the infant with breastmilk during the hospital stay.
Kitsantas and Pawloski 24 studied obese women (BMI >29 kg/m2) and reported that only overweight/obese women with medical or labor/delivery complications (i.e., diabetes, fetal macrosomia, etc.) were less likely to initiate breastfeeding compared with those overweight and obese women without those complications. These authors concluded that a health history and pregnancy complications of obese women would single out those in greater need of support for successful breastfeeding initiation. In light of the above, we agree that the extremely obese women in our study had more medical complications (i.e., cesarean deliveries, longer hospitalizations for mothers and infants).
Donath et al. 26 reported on breastfeeding and smoking and concluded that the lack of intention, perhaps due to preconceived notions and misinformation, was the main factor in low breastfeeding initiation and duration. Along these lines, in a survey of women attending an urban pediatric clinic, Bogen et al. 27 reported that 80% of them believe that women who smoke should not breastfeed. Additional factors related to the intention of exclusively breastfeeding include maternal knowledge about infants' health benefits and comfort with breastfeeding in social settings.10,26–30 Some investigators have reported difficulties with lactation by women who are obese, as well as those who have large breasts, or both.29,31–33 It is important for healthcare providers to be aware that in the past, significant numbers of lactation consultants have been unaware of low breastfeeding initiation and early cessation among obese, very obese, and extremely obese women.29,34
Limitations of our study are those typical of retrospective investigations as well as the absence of postdischarge feeding information. The strength, however, is that we describe a population of women at risk for breastfeeding initiation failure compounded not only by obesity but also by neonatal macrosomia. Our large sample of women not only met the inclusion criteria for this specific study, but also allowed us to categorize women by degree of obesity. Furthermore, we recognize that most obese and very obese women are able to initiate breastfeeding at the same rate as normal-weight and overweight counterparts. Conversely, extremely obese women remain a specific group that will require special intervention.
Conclusions
We have examined breastfeeding intention and breastfeeding initiation in a large cohort of women grouped by prepregnancy BMI. Overweight, obese, and very obese women have rates of breastfeeding intention similar to those of normal-weight women. However, extremely obese women have a lower rate of intention to breastfeed. Unlike the other groups, they seem to be younger, less educated, and more often black. These characteristics identify a group at risk for both lack of intention to breastfeed and breastfeeding initiation failure and define an opportunity for targeted intervention. It is remarkable that successful breastfeeding initiation of all women regardless of prepregnancy BMI who intended to breastfeed further enhances the importance of assessing breastfeeding intention during the antepartum period.
Footnotes
Disclosure Statement
No competing financial interests exist.