
Abstract
Abstract
Objective:
Mother's own milk (MOM) remains the key strategy to prevent necrotizing enterocolitis (NEC) in preterm infants. We developed and implemented quality improvement (QI) initiatives to improve rate of using MOM in preterm infants of <32 weeks of gestation. The objective was to evaluate the impact of this QI project on NEC incidence in this population.
Study Design:
In November 2009, we established a QI multidisciplinary team that reviewed literature and practices of other institutions to promote exclusive use of MOM in preterm infants of <32 weeks of gestation. The team developed practice changes that were implemented in February 2010. We tracked use of MOM and occurrence of NEC stage ≥2 from January 2009 until March 2012 when donor human milk was introduced. The subjects were divided into three groups: baseline (year 2009; n=189), intervention phase (year 2010; n=202), and sustain phase (January 2011–March 2012; n=254). Clinical outcomes of the baseline and sustain phases were compared.
Results:
Exclusive use of MOM improved significantly from 60.8% to 73.6% at time of first feed (p=0.004) without any delay in feed introduction (median [interquartile range], 40 [26, 75.5] hours versus 43.5 [24, 69] hours; p=0.96). There was a nonsignificant increase in exclusive use of MOM at time of full feed (from 79.5% to 85.2%; p=0.11); however; use of any MOM increased significantly from 80.4% to 91.3% (p<0.001) at discharge. Time to reach full feed and length of stay remained similar between the baseline and sustain periods. On regression analysis, risk of NEC decreased significantly in the sustain period (odds ratio=0.32; 95% confidence interval, 0.11–0.93).
Conclusions:
QI initiatives were effective in increasing use of exclusive MOM at time of first feed and of any MOM at time of discharge and in reducing NEC incidence in our neonatal intensive care unit.
Introduction
N
It has been the practice to introduce early trophic feeds to enhance feeding tolerance in small preterm infants. There is an implicit expectation that shorter time to achieve full enteral feeds could be protective from hospital-acquired infections, due to shorter duration of indwelling central venous catheters used to deliver parenteral nutrition.12,13 A report found that only 61% of very low birth weight infants were discharged from the hospital on any breastmilk. 14 Unfortunately, mother's milk is often unavailable to preterm infants in the first few days of life, whereas minimal enteral nutrition is optimally commenced shortly after birth. Lack of availability of the mother's breastmilk represents the most common reason for not providing breastmilk to preterm infants. 15
The latest report from Health Canada identified that 87.3% of mothers breastfed or tried to breastfeed their last child. 16 However, duration rates fell shortly after birth. The most significant drop in breastfeeding rates usually occurs in the first 2–4 weeks after birth. 17 In order to improve the likelihood that the mother will continue breastfeeding, she needs substantial breastfeeding support during the postpartum period. 18 Healthcare providers play an essential role in a woman's initial decision to breastfeed. 19 However, many practitioners providing health care for postpartum mothers have little or no formal education in breastfeeding initiation. 20 This lack of specific education about techniques and methods to improve initiation of breastfeeding may result in providing insufficient instruction or conflicting advice on breastfeeding techniques, particularly for mothers who are additionally stressed by having a preterm infant.
A quality improvement (QI) project was started in our NICU for mothers delivering preterm infants in order to promote breastfeeding and increase the percentage of preterm infants discharged from the hospital on mother's own breastmilk. This QI project preceded the opening of the local Mother's Milk Bank. The goal of this study is to assess efficacy of the used QI initiatives on improving rate of MOM feeding in preterm infants born at <32 weeks of gestation and to determine the effect of these initiatives on incidence of NEC and other neonatal outcomes.
Materials and Methods
Design and ethical issues
This was a retrospective, observational study of preterm infants born at <32 weeks of gestation before and after the QI efforts with the following goals: (1) to improve the rate of maternal breastmilk feeding among the preterm infants born at <32 weeks of gestation, (2) to increase the use of colostrum for trophic feeds, and (3) to shorten the time to introduction of trophic feeds. The study was approved by Alberta Children's Hospital Ethical Board. No experimental practices were involved. The study population included all preterm infants born at <32 weeks of gestation and admitted to our tertiary NICU at Foothills Medical Centre between December 1, 2009 and March 31, 2012.
Description of the QI intervention
Using the Plan-Do-Study-Act methodology for QI, practice changes were developed and implemented sequentially. A multidisciplinary team, composed of a neonatologist, a nurse, and a lactation consultant (LC), reviewed the literature to identify the best methods to improve maternal lactogenesis in the early postpartum period. Educational materials were developed to teach LCs about the physiologic benefits of colostrum, strategies for hand expression of the breast to obtain early colostrum, and how to use the breast pump effectively. These materials were then modified for maternal education to be distributed and taught by the LCs, accompanied by a breastmilk collection package. The package contained syringes for collection of initial small volumes of colostrum and collection and storage containers for larger volumes of colostrum. In addition to written education material, an educational DVD (Breastfeeding Solutions, Apto, CA) 21 was also provided. The specific best practices utilized and shared with the nursing staff in the training included (a) early pumping and expression, (b) importance of hand expression with “hands on pumping,” (c) pumping routine, every 3 hours during the day and at least once during the night, (d) emphasis on the value of colostrum (i.e., “every drop counts”), and (e) education about important protective effects of breastmilk for preterm infants.
To facilitate early collection of colostrum, contact with the LC was targeted for within the first 6–12 hours postpartum. If the mother delivered unexpectedly, the LC would receive the consultation request and contact the mother as soon as possible postpartum. Furthermore, a LC or postpartum nurse observed hand expression and breast pumping at the beginning as part of the teaching, and amounts of expressed milk were checked on a regular basis after that. However, there were some mothers who had delayed first contact with the LC in the intervention period.
The first 6 months of intervention involved mothers of preterm infants born at <29 weeks of gestation. Given the limited availability of LCs and the plan to include all preterm infants born at <32 weeks in the project, in subsequent cycles, nurses were educated to be able to provide early bedside consultation. The NICU nurses were the first group of nurses approached to participate. Subsequent cycles led to involvement of antepartum nurses, as well as labor and delivery nurses, to provide education and information in advance of formal LC consultation. Lastly, LC consultations were offered to antepartum inpatient women at risk of preterm labor. Interventions of the QI project by date are summarized in Table 1. There were no other changes in clinical practice related to delivery, mother care, and neonatal care in the NICU during the washout period.
LC, lactation consultant; MOM, mother's own milk; NICU, neonatal intensive care unit; QI, quality improvement.
Study subjects and data collection
All mothers of infants <32 weeks of gestation who delivered at Foothills Medical Centre were eligible for the study. The following subjects were excluded: (1) infants of mothers with positive human immunodeficiency virus status or other contraindication for breastfeeding such as galactosemia, (2) infants born out of the Foothills Medical Centre, and (3) infants with major congenital or chromosomal abnormalities.
Data on the feeding type, date of starting, and duration to reach full feed were collected prospectively and linked later to other neonatal outcome data using the patient health record number.
Gestational age was defined as the best obstetric estimate that is based on early prenatal ultrasound, consistent obstetric examination, and obstetric history, unless the postnatal pediatric estimate of gestation differed from the obstetric estimate by more than 2 weeks. NEC was defined according to modified Bell criteria (stage II or higher). Bronchopulmonary dysplasia (BPD) was defined as the use of supplemental oxygen or mechanical ventilation at 36 weeks postmenstrual age. Patent ductus arteriosus was defined as clinical or echocardiographic diagnosis plus treatment with indomethacin, surgical ligation, or both. Intraventricular hemorrhage was diagnosed based on ultrasound and classified according to the grading by Papile; grade 3 and 4 hemorrhages were considered as severe intraventricular hemorrhage. Sepsis included any positive blood or cerebrospinal fluid culture after birth. Feed start was defined by three successful consecutive feeds, and full feed was defined by reaching 120 mL/kg/day.
Data analysis
The null hypothesis was that rates of breastmilk feeding in preterm infants born at <32 weeks of gestation would be similar over time despite our exclusive MOM project. Time periods were categorized as baseline period (12 months before intervention), washout period (12 months during intervention), and sustain period (15 months between end of washout period and until donor human milk was introduced). The washout period was not used in the comparison due to the following: (1) the first two cycles (6 months) involved NICU nurses only, and the intervention was limited to preterm infants born at <29 weeks of gestation, and (2) the intervention in the subsequent two cycles (6 months) involved labor and delivery nurses in addition to the NICU nurses and included all preterm infants born less than 32 weeks. However, the trends of the changes in the rate of breastfeeding and NEC outcomes during the entire study period, including the washout period, are illustrated in the figures.
Descriptive statistics including means, medians, standard deviations, and interquartile ranges were used to describe the study population. The categorical variables were compared between the previous described periods using the chi-squared test or Fisher's exact test. Continuous variables were analyzed using Student's t test or the Mann–Whitney U test when appropriate.
In order to account for differences in patients' characteristics and for potential confounding factors, multivariable logistic regression was used for dichotomous outcomes, and robust linear regression was used for continuous outcomes, which were positively skewed and had some outliers. Risk adjustment covariates were those found to be relevant to the outcomes of interest either in the current bivariate comparison of the baseline characteristics with p value of <0.1 or from previous studies. Modeling using times to start (in hours) and reach full feed (in days), length of stay (in days), and their natural logs produced the same conclusion. We presented our results using hours and days as they are easier to interpret than the transformed data.
Similar analysis was used to further explore the relationship between each type of feed including exclusive MOM, formula, and mixed feed and the former outcomes of interest. A p value of <0.05 was considered statistically significant, and 95% confidence interval (CI) was documented when appropriate. All statistical analyses were performed using Stata version 12.1 software (StataCorp, College Station, TX).
Results
In total, 217 and 281 infants born at <32 weeks of gestation at Foothills Medical Centre were identified in the baseline and sustain period, respectively. Eight and 13 subjects were excluded due to congenital anomalies, in addition to 9 and 14 subjects who died in the baseline and sustain period, respectively. Two subjects received donor milk in the sustain period and were excluded from the analysis. Data were available for 189 and 254 in the baseline and sustain periods, respectively.
Table 2 describes the maternal and neonatal characteristics of subjects included in the study. All characteristics were similar between baseline and sustain periods; however, there was a trend toward more deliveries by cesarean section in the sustain period. Table 3 summarizes the neonatal outcomes. On bivariate analysis, infants born in the sustain period had a marginal decrease in NEC and a shorter duration of mechanical ventilatory support. Feeding characteristics are presented in Table 4. There were no significant difference in age of starting feed and duration to reach full feed. Use of exclusive MOM at “feed start” increased significantly in the sustain period, but no difference was observed at duration to reach full feed. In contrast, use of any MOM at discharge improved significantly in the sustain period (Fig. 1). As expected, use of exclusive MOM increased between feed start and time of reaching full feed in both baseline (p<0.001) and sustain (p=0.002) periods. However, use of mixed feed (maternal human milk and formula) declined significantly between time of starting feed and time of reaching full feed in the sustain period (from 15.6% to 8.6%; p=0.03), whereas no significant change was noticed in the baseline period (from 9.0% to 13.6%; p=0.18).
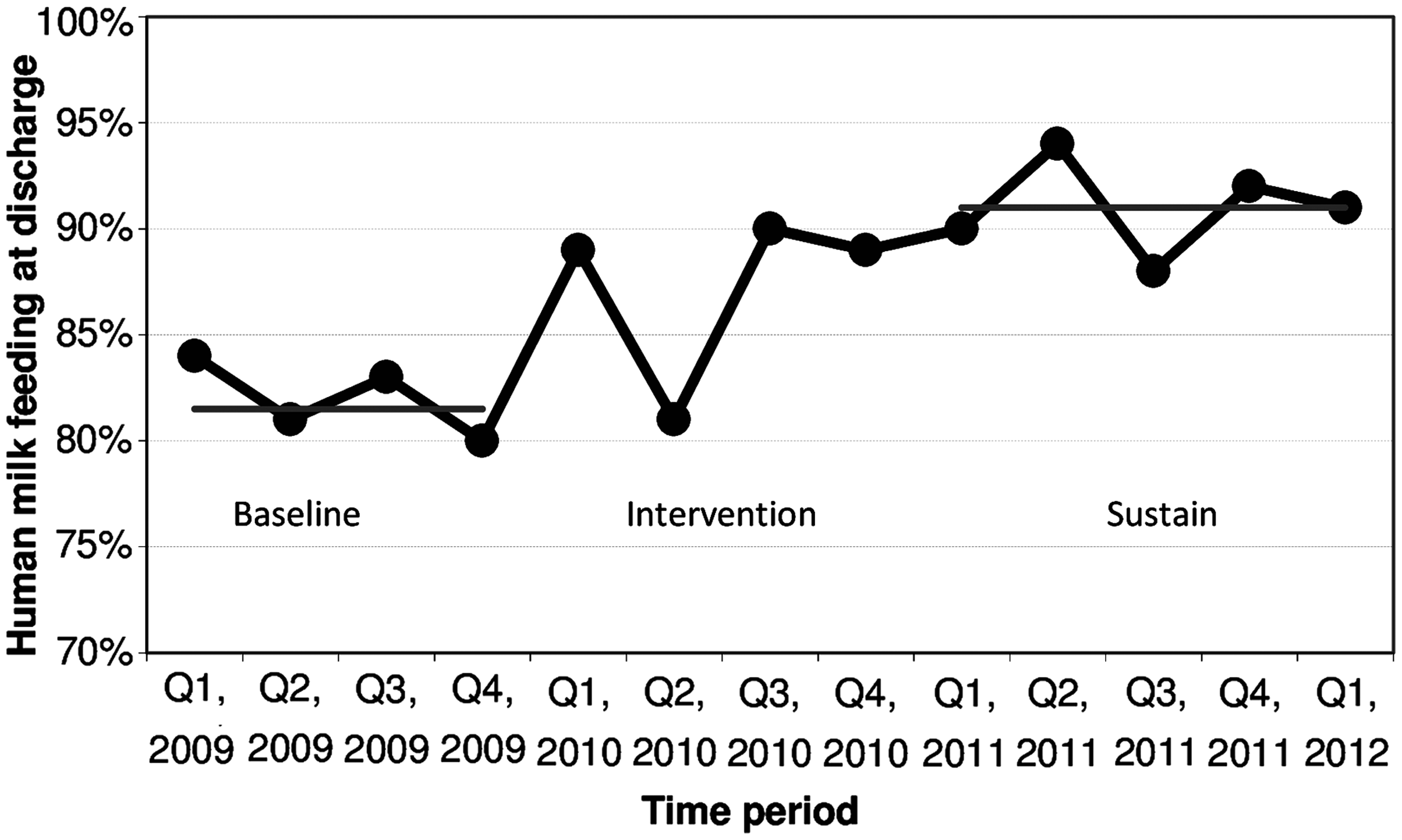
Rate of mother's own milk feeding at discharge by period. Q, quarter.
Continuous data are presented as mean±SD for normally distributed and median (interquartile range) for skewed data.
SNAP II, severity of sickness scale.
Data are number (%) unless indicated otherwise.
Continuous data are presented as median (interquartile range) due to skewed distribution.
BPD, bronchopulmonary dysplasia; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; PDA, patent ductus arteriosus; ROP, retinopathy of prematurity.
Continuous data are presented as median (interquartile range) due to skewed distribution.
Time to reach 40 mL/kg/day was used as a surrogate for feed tolerance.
Full feed was defined by 120 mL/kg/day.
On robust linear analysis, our QI project did not change the time to reach full feed (coefficient=−0.7 day; 95% CI, −1.9 to 0.4) after correcting for gestational age, being small for gestational age, severity of sickness at birth, and patent ductus arteriosus required treatment. There was no effect on length of stay (coefficient=1.7 day; 95% CI, −4.2 to 2.8) with additional adjustment for NEC, late-onset sepsis, and BPD. Figure 2 shows the decline in NEC incidence over time. Although there was a marginal reduction in rate of NEC on the bivariate analysis (Table 3), the NEC rate decreased significantly (odds ratio [OR]=0.32; 95% CI, 0.11–0.93) when the logistic regression model was used to correct for previous risk adjustment variables (i.e., gestational age, small for gestational age, severity of sickness at birth, and patent ductus arteriosus required treatment). In contrast, there was no effect on BPD rate (OR=0.59; 95% CI, 0.31–1.11) with similar adjustment.
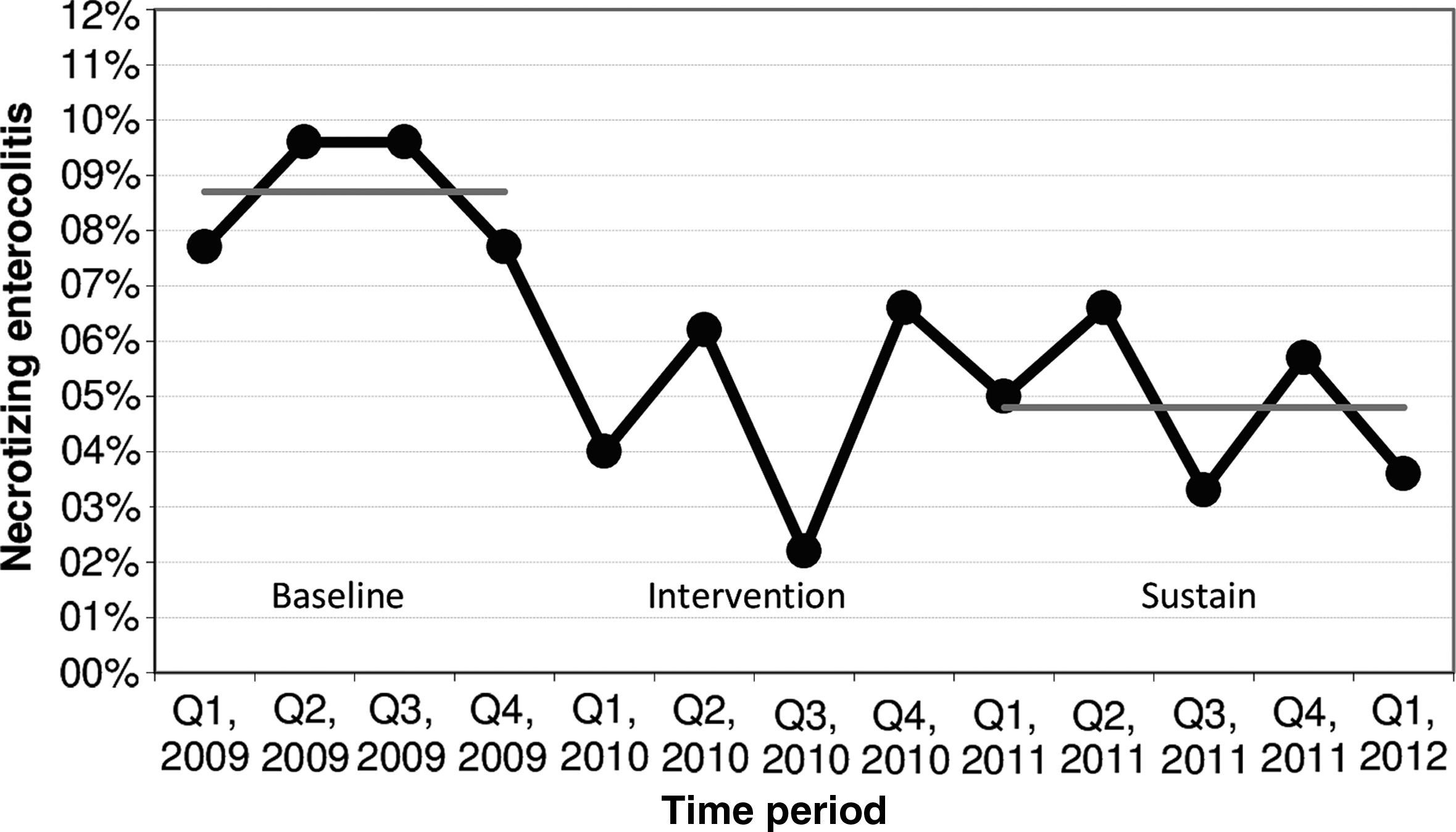
Incidence of necrotizing enterocolitis by period. Q, quarter.
In order to study effect of type-specific feeding on clinical outcomes, all data were pooled, and use of formula and mixed feed was compared with the use of exclusive maternal human milk as the reference.
MOM, formula, and mixed feed were used at time of first feed in 68.8%, 18.4%, and 12.8%, respectively, and at time of reaching full feed in 83.4%, 5.9%, and 10.8%, respectively.
Use of formula alone or mixed with human milk at first feeds resulted in a significant decrease in the time to start feed (coefficient=−9.3 hours; 95% CI, −16.1 to −2.5) and the time to reach full feed (coefficient=−2.0 days; 95% CI, −3.3 to −1.7). Risk for NEC increased significantly in infants who exclusively used formula at full feed (OR=5.28; 95% CI, 1.21–22.9), whereas there were no cases of NEC in the mixed feed group. Risk for BPD was less in infants who received mixed feed at the time of full feed (OR=0.16; 95% CI, 0.03–0.71). However, only 26 subjects were in this group.
Discussion
The present QI project aimed to promote maternal breastmilk feeding in preterm infants born at <32 weeks of gestation. Exclusive maternal breastmilk feeding improved significantly from 60.8% to 73.6% at time of first feed without any delay in feed introduction. Despite the limited improvement at time of full feed, more infants were discharged home on breastmilk. This increase in maternal breastfeeding resulted in a significant decrease in the risk of NEC.
Merewood et al. 22 have shown similar improvement in the initiation of human milk feeding in infants admitted to their NICU after implementing the Baby-Friendly Hospital Initiative. However, the study included term and preterm infants and defined successful initiation if the infant received at least one human milk feeding in the first week of life. The rate of successful initiation improved from 34.6% to 74.4%. Our QI project showed ability to increase exclusive human milk initiation even with a higher baseline rate.
Although it was not statistically significant, the QI project appeared to marginally increase the use of exclusive maternal milk at time of full feed. Lowenstein et al. 23 have documented significant increase in human milk use at Day 14 of life from 64.95% to 73.66%. The median age of life to reach full feed in the current QI project was 13 days, which approximately matches the day identified by Lowenstein et al. 23 ; however, our use of human milk was significantly higher at baseline (79.5%) and in the sustain period (85.2%). Furthermore, our project described the use of exclusive maternal breastmilk at time of full feed (except for adding human milk fortifier), whereas Lowenstein et al. 23 reported any use of human milk.
Use of any maternal human milk at discharge was also increased in our project from 80.4% to 91.3%. Lee et al. 15 showed a 9.4% increase in the use of any human milk at discharge; however, the rate of any human milk use at discharge was only 64%, which is much lower than our rate in the baseline period. In contrast, Lowenstein et al. 23 reported no change in the use of any human milk at time of discharge in spite of the relatively good percentage of use at Day 14 (82.4%) and Day 28 (80.0%). Their rates of use at discharge were 37.93%, and 38.58% in the prestudy interval and during the project, respectively. A recent multicenter large Italian study with 31% of participants weighing <1,500 g has shown that the proportion of infants not fed with human milk varied from 6% to 82% across different centers. 24 This indicates the wide difference in practice and emphasizes the role of continuous lactation support for mothers of preterm infants during their long stay in the NICU.
Use of exclusive human milk remains the major protective factor against NEC in preterm infants. 25 In our study, NEC rates were decreased from 8.9% at baseline to 4.8% in the sustained period. This finding is consistent with the results of the QI initiative by Lee et al., 15 who reported a decrease in NEC rate from 7.0% to 2.4%. During the period of this QI initiative, our NICU did not have access to donor human milk, so the time to start feeds was not significantly shortened, as the “culture of the unit” changed such that the healthcare team became adverse to beginning feeds with formula. Similarly, the time to reach full feeds was not shortened. However, more infants were receiving exclusive mother's milk at the start of feeds, defined as three or more consecutive feeds, and significantly more infants were discharged home feeding on mother's milk. The increased use of mother's milk is associated with a decrease in NEC, when adjusting for other risk factors. The premature gut is colonized rapidly after birth, and under an ideal environment, a normal intestinal immune defense system develops. Aberrant bacterial colonization of the immature intestine is a significant risk factor identified with NEC. 26 This can largely be explained by the fact that early use of MOM promotes intestinal colonization of a balanced, nonpathogenic microbiota that helps prevent the abnormal bacterial growth that is commonly seen in formula-fed infants.27,28
When our data were pooled, risk of BPD decreased in the mixed feed group only. Although prematurity and ventilation remain the main risk factors for BPD, pulmonary inflammation remains the common pathway for lung injury. 29 In contrast, improving nutritional status has shown a protective effect against BPD and is considered a fundamental key to outgrow BPD. 30 Use of human milk confers precise immunologic and anti-inflammatory advantages to preterm infants. However, human milk does not meet the energy and protein needs of preterm infants. Therefore, we hypothesize that the decreased rate of BPD in the mixed feed group may be due to a combined effect of anti-inflammatory/immunological effects of MOM and achieving more optimal energy and protein needs using formula. Nonetheless, further research work is required to investigate the best way of human milk fortification. Interventions of our QI project exhibited the capacity to promote MOM use despite the relatively high baseline rate to begin with. The interventions applied in our QI strategy were simple, locally developed written and visual educational materials, augmented with a commercially available DVD, delivered one-on-one to the mother by nursing and LC staff. Using these interventions in NICUs with lower rate of MOM use should be feasible, with the potential to enhance use of mother's milk feeds and reduce the rate of NEC.
Although our results provide details on an effective QI project to promote exclusive use of maternal breastmilk in a regional NICU, several limitations need to be considered. These include the pre–post design of the study, use of historical control, lack of MOM dose measurement, and lack of data on number of women provided the education in each period. Furthermore, the study described the era preceding introduction of donor human milk. Therefore, we cannot conclude whether the efficacy of this QI project will continue with the use of donor human milk; however, data collection is ongoing, and we plan to report our outcomes in the future.
Conclusions
The current QI project demonstrates a successful strategy to improve rate of maternal human milk use in a Level III NICU with a limited number of LCs. Moreover, it provides a low-cost model to decrease NEC rates in NICUs when donor milk is not available. We also identify the need for an ongoing data collection, quantifying human milk dose in the first few weeks, and determining the cost–benefit of our approach in the future studies.
Footnotes
Acknowledgments
We would like to thank Drs. Andrei Harabor and Carlos Fajardo, Section of Neonatology, Department of Pediatrics, University of Calgary, for separately reviewing abdominal X-ray images and defining stages of NEC.
Disclosure Statement
No competing financial interests exist.