
Abstract
Abstract
Introduction:
The research was conducted to determine the correlation between breastfeeding success in the early postpartum period and the perception of self-efficacy in breastfeeding and breast problems in late postpartum.
Methods:
This analytic and cross-sectional research was carried out at Aydın Obstetrics and Gynecology and Children's Diseases Hospital. Three hundred twenty-seven primipara mothers who had delivered a single baby of healthy term at 37 or more gestational weeks with no previous experience with breastfeeding and who agreed to cooperate participated in the research.
Results:
The mothers' mean gestational week of delivery was 39.25 ± 1.10 weeks, and it was found that 56.0% had delivered by cesarean section and 57.0% had started to breastfeed immediately after the birth. The mothers' LATCH mean score was 6.55 ± 0.86; their postnatal breastfeeding self-efficacy mean score was found to be 59.10 ± 7.21. Mothers who had high success in breastfeeding at early postpartum were found to experience fewer problems with their breasts (Z = −2.65, p < 0.05), gave birth by vaginal delivery (Z = −2.88, p < 0.05), and had not received anesthesia during the delivery (Z = −2.52, p < 0.05). In the correlation analysis, it was seen that mothers with high success in breastfeeding also had high self-efficacy scores (r = 0.210, p = 0.003).
Conclusion:
The results of the research indicated that breastfeeding success in the early postpartum period reduced breast problems and increased the perception of breastfeeding self-efficacy in the late postpartum period.
Introduction
T
Research shows that the factors causing the failure to continue with breastfeeding include the following: the mother's perception that her milk is inadequate and that the baby will not be nourished properly; the baby's inability to suckle due to faulty breastfeeding technique; different problems with the breast and the nipple; the lack of enthusiasm of the mother about breastfeeding; the lack of information and low feelings of self-efficacy of the mother concerning breastfeeding; the baby being fed by someone other than the mother through the night; bottle feeding; mixed messages given to the mother; feeding by the clock; inadequacy in informing and supporting the mother; and the inability to find solutions to the challenges the mother may face shortly after the delivery.4–6
Midwives play a major role in starting off breastfeeding after delivery and having it successfully continue; as such, they need to be fully aware of the factors that have an impact on the success of breastfeeding and they must be able to evaluate the degree of success and be equipped with appropriate plans for intervention.7,8 One of the most important factors that influence the success of breastfeeding is whether the mother is willing to breastfeed or not, how much effort she will spend on this, and her perception of self-efficacy in breastfeeding, meaning her emotions and thoughts about the activity.9–14 The stronger the perception of self-efficacy, the stronger are the mother's efforts, persistence, and endurance. 9 Another factor that may hinder a mother from continuing to breastfeed her infant is any breast-related problem she may face. Of mothers who breastfeed, 80–90% experience nipple pain and it is known that 26% of these mothers go on to endure cracking and even quite severe pain in the nipples. 15 In this context, evaluating mothers' breastfeeding success in the early period right after delivery may enable midwives in not only preventing the development of breast problems but also in helping to increase mothers' perception of breastfeeding self-efficacy, thereby contributing to a longer breastfeeding experience.
Materials and Methods
Research purpose
The research was conducted as an analytic and cross-sectional study to determine the correlation between breastfeeding success in the early postpartum period and the perception of self-efficacy in breastfeeding and breast problems in the late postpartum.
Data collection
The study recruited primipara mothers, ages 18–35, who had delivered a single baby of healthy term at 37 or more gestational weeks, who had no previous experience with breastfeeding, and who agreed to participate in the research. To avoid an adverse effect on research results, mothers who did not nurse their babies, had chronic illnesses, or had psychological disorders (diabetes mellitus, hypertension, depression, and so on) were excluded from the research.
The data for the research were compiled in two stages. In the first stage, interviews were conducted with the mothers in the first 24–48 hours postpartum using the face-to-face interviewing technique. In this first interview, the researcher filled out the data collection form on the descriptive characteristics of the mothers as well as the LATCH breastfeeding assessment tool. The LATCH breastfeeding assessment tool used in evaluating the success of the mothers in breastfeeding was used in two different breastfeeding periods. The mothers' addresses and telephone numbers were recorded during the interviews. The interviews each took an average of 30 minutes. In the second stage of the research, breast-related problems were assessed on the 40th day postpartum and later with a home visit or telephone call by the filling out of a postnatal breastfeeding self-efficacy scale. The interviews each took an average of 15 minutes.
Data collection instruments
Mother's descriptive form
This form comprised 25 questions compiled by a scan of the literature. The questionnaire included questions on the sociodemographic characteristics of the mothers and their spouses, obstetric data, as well as questions related to breastfeeding.
The LATCH breastfeeding assessment tool
One of the measurement tools used to assess breastfeeding is LATCH. The LATCH breastfeeding assessment tool was created in 1986 and uses a scoring system that is similar to that of APGAR. This measurement tool was developed to provide an objective assessment of breastfeeding, determine the nature of breastfeeding problems, design training plans, and to create a common language among health professionals, which could be used in research. 13 The tool is based on five assessment criteria (Latch on breast, Audible swallowing, Type of nipple, Comfort breast/nipple, Hold), and the initials of each criterion in English make up the acronym.
Each item is assessed on the basis of 0–2 points. The total points that can be received on the scale is 10 (Fig. 1). 16 There is no cutoff point on the tool and as the LATCH score rises, breastfeeding success is understood to be high. Adams and Hewell studied the reliability of the LATCH Breastfeeding Assessment tool in the United States in 1997, and its interrater reliability rate was found to be 94.4%. Yenal and Okumuş tested the reliability of the scale in Turkey and its Cronbach alpha value was found to be 0.95. 17
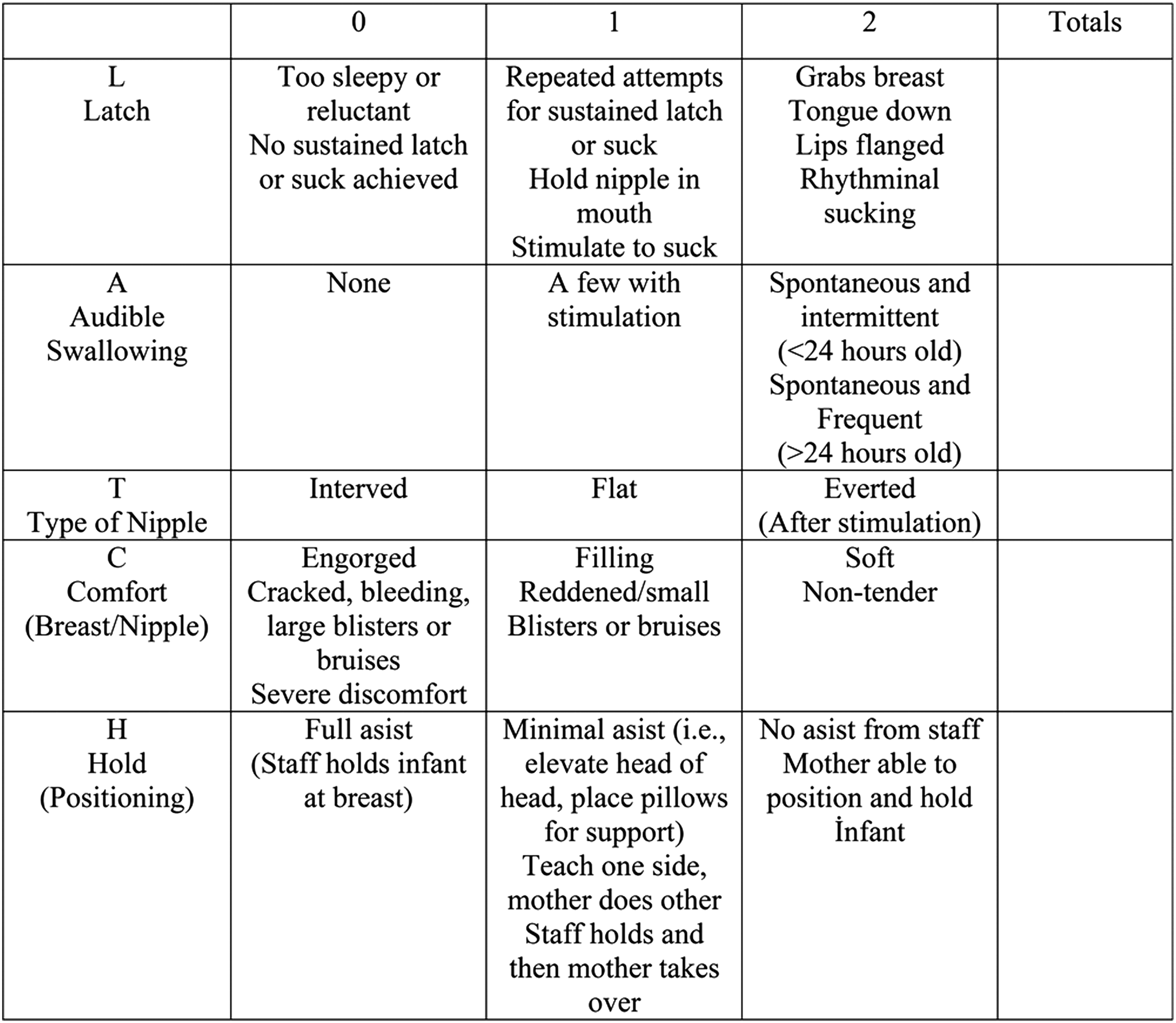
LATCH Breastfeeding Assessment.
Postnatal Breastfeeding Self-Efficacy Scale Short Form
Dennis and Faux developed the first Breastfeeding Self-Efficacy Scale as a 33-item questionnaire. Later, the scale was reviewed and turned into a short form of 14 items. The scale assesses how confident mothers feel about being able to breastfeed. All of the items in the scale are presented positively. The scale is a five-item Likert type of scale, assessing responses on a range of “I'm not at all sure” (one point) to “I'm always sure” (five points). The minimum score that may be received is 14; maximum is 70. There is no cutoff point on the scale. 18 The higher the score, the higher is the level of self-efficacy in the context of breastfeeding. Aluş-Tokat and Okumuş drew up the Turkish version of the scale. The Cronbach value for the scale was 0.86; it was found to be a reliable measurement tool. 19 The Cronbach alpha value for the scale in this study was found to be 0.89.
Postpartum breast problems form
This form was developed based on a scan of the literature and comprises 10 questions related to maternal postpartum breast problems (cracking of the nipples, engorged breasts, breast abscesses, mastitis, and so on).
Setting
The research was conducted over the period January to November 2012 with mothers in the Obstetrics Service of the Aydın Obstetrics and Gynecology and Children's Diseases Hospital of the Turkish Ministry of Health. The hospital actively supports the WHO 10 steps for breastfeeding support. With a bed capacity of 254, the hospital houses obstetrics, gynecology and children's services, delivery rooms, and neonatal and surgical intensive care units. The postpartum floor where the research took place has a capacity for 34. The hospital generally employs a total of 139 midwives, 64 nurses, and 14 obstetrics–gynecology specialists, and there are 14 specialized physicians, 10 midwives, and 1 nurse working on the postpartum floor. The standard stay at the hospital after delivery is at least 12 hours for normal spontaneous vaginal births and at least 48 hours for cesarean deliveries. The hospital has a prenatal preparatory class available, and breastfeeding training is provided in this program. In addition, at discharge after delivery, a written brochure is handed out to mothers on the breastfeeding training program and about breastfeeding.
Sample
Primipara mothers living in the city center of the province of Aydın with no prior breastfeeding experience delivering at the Aydın Obstetrics and Gynecology and Children's Diseases Hospital of the Turkish Ministry of Health constituted the study population. According to the hospital records, the number of births at the Aydın Obstetrics and Gynecology and Children's Diseases Hospital of the Turkish Ministry of Health was 4,419 in 2010. Of the mothers giving birth, 32% (n = 1,414) were primiparas. The NCSS-PASS 2008 (Statistics, Power Analysis & Sample Size Program) was used to employ power analysis in determining the size of the sample. Before the research, power analysis results demonstrated a Type I error of 0.05, and at a power of 80%, the sample size was calculated to be 327. In line with this, a convenience sampling of 327 mothers was taken into the study. The research was, however, ultimately completed with 200 mothers (Fig. 2). The mean scores obtained in the research on the LATCH breastfeeding assessment tool and the Postnatal Breastfeeding Self-efficacy Scale were taken as a base, and in the post hoc power analysis, the sampling of 200 was accepted with a Type I error of 0.05, indicating that the power of the study was 85%.
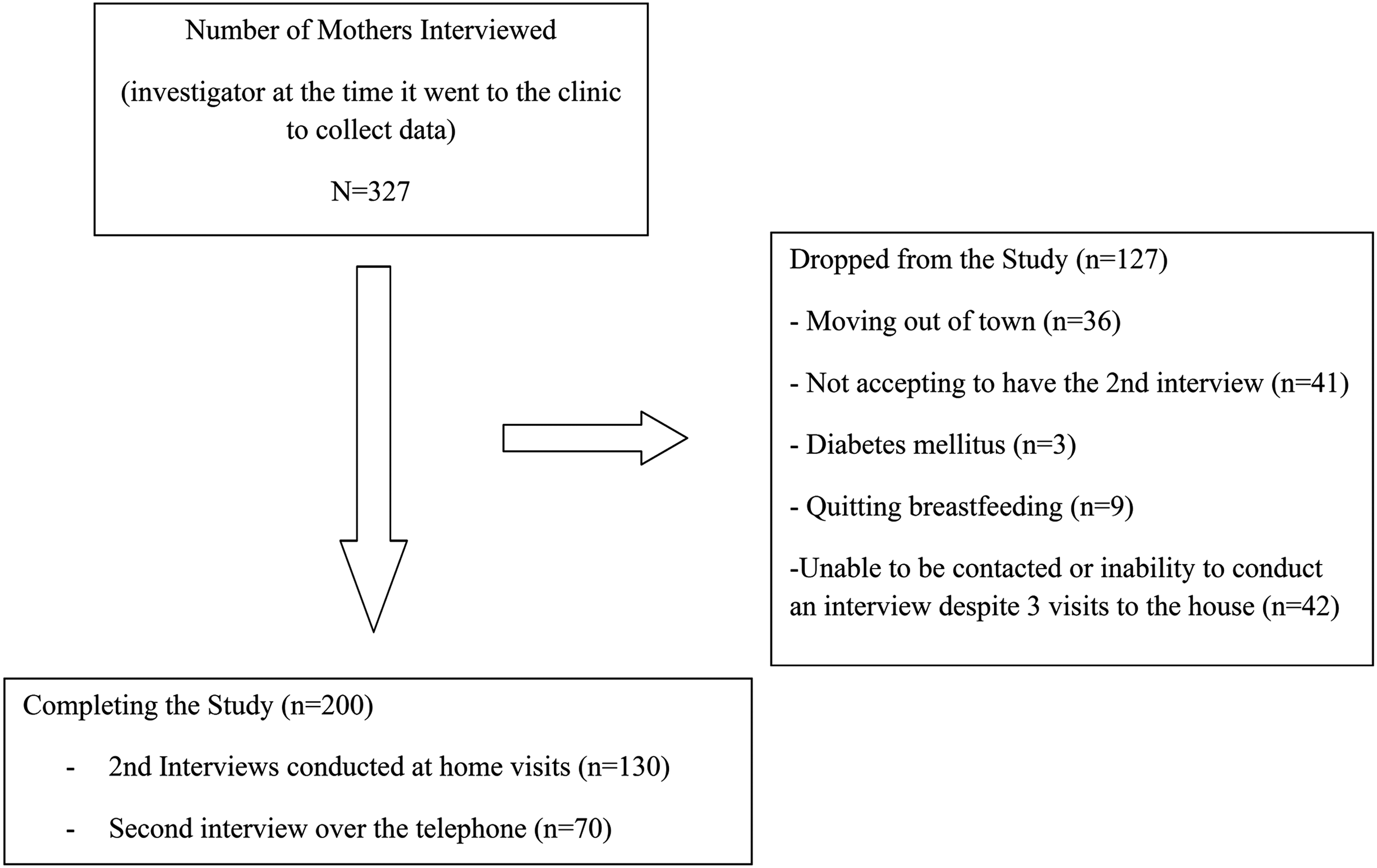
The Study Population and the Sample.
Data analysis
The data from the research were analyzed using the Statistical Package for the Social Sciences, Version 16.0 (SPSS). Numbers and percentage distributions were used for the descriptive statistics; mean scores were used in the LATCH Breastfeeding Assessment tool and the postnatal breastfeeding self-efficacy perception scale. Pearson's correlation coefficient was used to determine the correlation between the LATCH breastfeeding assessment scale scores and the breastfeeding self-efficacy scores. The correlation between the mothers' descriptive characteristics and breastfeeding, fertility, breast problem, and neonatal data and the mean scores on the LATCH assessment tool and the postnatal breastfeeding self-efficacy perception scale were explored with an analysis using the Kruskal–Wallis and Mann–Whitney U tests. Significance was determined as 0.05 in the statistical assessments.
Matters of ethics
Approval was obtained from the Adnan Menderes University Faculty of Medicine Noninterventional Clinical Research Ethics Board for the implementation of the research and the collection of data. The mothers included in the research were duly informed about the study and their written consent was elicited.
Research limitations
The research was carried out using the convenience sampling method. Because of this, the data obtained are representative only of the women participating in the study.
Results
The research was completed with 200 mothers. The mean age of the mothers in the study was 24.96 ± 5.05 (range: 18–35); 29.0% were high school graduates and 30.5% worked, and it was found that 64% of the employed mothers worked in the private sector (Table 1).
The data did not display normal distribution by Kolmogorov–Smirnov Test.
The Mann–Whitney U and Kruskal–Wallis H tests were used. Statistically significant values are shown in bold.
SD, standard deviation.
Of the mothers, it was observed that 91.0% had a planned pregnancy; average gestation at the birth was 39.25 ± 1.10 weeks (range: 37–42). It was seen that 56.0% had delivered by cesarean section, 57.0% had received anesthesia during the delivery, and, of these women, 84.2% were administered epidural anesthesia. It was found that 25.0% of the mothers had experienced problems in their last pregnancy; the leading problem with pregnancy was danger of miscarriage, at 38.0%, followed by a rate of 24.0% for nausea and vomiting. In the research, it was determined that the breastfeeding success was higher in the mothers who gave birth with vaginal delivery (Z = −2.88, p < 0.05) and had not received anesthesia during the delivery (Z = −2.52, p < 0.05) (Table 1).
Of the mothers participating in the study, 52.4% had delivered girls; average birth weight was 3,280.28 ± 395.50 g (range: 2,500–5,000) while average height was 49.51 ± 1.56 cm (range: 46–56) (Table 1).
The mothers' mean score on the LATCH Breastfeeding Assessment Tool at the first observation was 6.49 ± 1.29 and 6.60 ± 1.18 at the second observation. The average of the two total observation scores was 6.55 ± 0.86 (range: 3–9). The late postpartum breastfeeding self-efficacy scale mean score of the mothers was found to be 59.10 ± 7.21 (range: 14–70).
Of the mothers participating in the study, 68.0% (136 mothers) were noted to have developed breast problems in the postpartum period. These breast problems were seen to be cracking of the nipples in 125 mothers, engorged breasts in 24 mothers, breast abscesses in 12, mastitis in 4, and fungus infections in 3 mothers. It was found that in mothers who did not experience postpartum breast problems, LATCH Breastfeeding Assessment Tool total mean scores were higher (Z = −2.65, p < 0.05) (Table 2).
The data did not display normal distribution by Kolmogorov–Smirnov Test.
The Mann–Whitney U test was used. Statistically significant values are shown in bold.
Table 2 displays the distribution of total mean scores on the late postpartum breastfeeding self-efficacy scale according to the presence of postpartum period breast problems in the mothers. In the statistical analysis, it was seen that there was no significant difference in the total mean scores of the mothers on the late postpartum breastfeeding self-efficacy scale according to the presence or absence of postpartum breast problems (Z = −1.25, p > 0.05). In the research, it was determined that the breastfeeding self-efficacy was higher in the mothers who gave birth by cesarean delivery (Z = −2.06, p < 0.05).
Of the mothers participating in the study, 57.0% of the mothers started breastfeeding immediately after delivery. In terms of the duration of breastfeeding, it was seen that 53.0% continued to nurse for as long as the baby wanted the breast; in terms of breastfeeding frequency, 50.5% nursed their baby on demand/when the baby cried. It was noted that 23.0% of the newborns were given food outside of mother's milk. A look into the reasons as to why mothers offered their babies food outside of mother's milk showed that 89.1% of the mothers believed that mother's milk would not be adequate for the child. A group of 71% of the mothers stated that they would nourish their infants exclusively with mother's milk for the first 6 months. It was observed that 37.5% of the mothers had received education in breastfeeding in the antenatal period; of the mothers who received this education, 64.0% had obtained the knowledge from midwives/nurses. Of the mothers, 98.5% were found to be receiving support in caring for the baby.
Table 3 shows the correlation between the LATCH breastfeeding assessment tool mean scores at the first, second, and at both observations of the mothers in the early postpartum and the late postpartum breastfeeding self-efficacy scale total scores. A positive correlation was seen between the LATCH breastfeeding assessment tool total scores and the total scores on the breastfeeding self-efficacy scale.
p < 0.01.
Discussion
In the study conducted to determine the correlation between mothers' breastfeeding success in the early postpartum and their perception of self-efficacy and breast problems in late postpartum, it was found that 68.0% of the mothers experienced postpartum breast problems and that these problems were mostly cracking of the nipples, engorged breasts, mastitis, breast abscesses, and fungus infections. In studies conducted with postpartum mothers, Kepekçi et al. and Gürol and Akyüz et al. have reported that 49.0%, 77%, and 51.7% of mothers, respectively, experience cracking of the nipples.20–22 In a study by İnce et al., it was found that 10.2% of mothers had cracked nipples, 3.4% suffered from mastitis, and that primiparas experienced more breast problems compared to their counterparts. 23 Research shows that breast problems are frequently encountered in the postpartum period and that the most common breast problem is cracked nipples.
Inadequate nursing in the first weeks after breastfeeding is initiated or the baby's suckling in the wrong position may lead to injury to the nipple, cracked nipples, and pain while nursing, thus making it more difficult for the infant to nurse on mother's milk and continue to breastfeed. 24 When breastfeeding is successful, however, breast problems are avoided and breastfeeding can continue. It has been discovered that mothers who have had a higher degree of success in breastfeeding in the early postpartum period experience fewer breast problems in the postpartum. Accordingly, Gürol's study has reported that the higher the score of mothers on the LATCH Breastfeeding Assessment Tool, the lower the incidence of nipple pain and trauma. 21
The two observations of the mothers' scores on the LATCH breastfeeding assessment tool showed a mean of 6.55 ± 0.86, and in studies with mothers with and without breastfeeding experience, these scores on the same assessment tool have been reported to be 8.40 ± 1.77 in a study by Yenal et al., 9.4 ± 0.7 in Duman's study, and 8.4 ± 1.8 in a study by Kumar et al.13,25,26 The lower mean scores in terms of breastfeeding success compared to other studies may stem from the fact that the present study was conducted with mothers who had no previous breastfeeding experience. In addition, in the study, the predictors of LATCH scores were not analyzed; this is a weakness.
The mean score of the mothers in the study on the late postpartum breastfeeding self-efficacy scale was found to be 59.10 ± 7.21. In a study by Yenal et al. with mothers with (59.1%) and without breastfeeding experience, the breastfeeding self-efficacy scale mean scores were found to be 59.49 ± 8.46. 13 Keemer's study with mothers with (57.9%) and without breastfeeding experience exhibited a breastfeeding self-efficacy scale mean score of 51.18 ± 12.48. 27 In a study by Alegria et al. with mothers in the early postpartum period, primiparas were found to have scores of 47.30 ± 11.18, while multiparas had scores of 52.87 ± 10.66. 28 The similarity of the results of the study in terms of the breastfeeding self-efficacy perception of the mothers, they be experienced or not, may stem from the fact that breastfeeding self-efficacy was evaluated in the late postpartum.
It was found in the study that self-efficiency in late postpartum period was lower in mothers who had given birth vaginally than in mothers with cesearean births. These results show a similarity to those of Wutke and Dennis. 29 It is thought that this situation may stem from an increased late postpartum perception of breastfeeding sufficiency as a result of more effort in breastfeeding in mothers who had a ceserean.
No correlation was found between the status of having a breast problem in the postpartum period and the mothers' perception scores on the late postpartum breastfeeding self-efficacy scale. In contrast to the result of this study, Gürol's study revealed a negative correlation between breastfeeding self-efficacy scores and nipple pain/trauma and it was seen that as the breastfeeding self-efficacy score rose, there were fewer incidents of nipple pain or trauma. 21 The differing results may stem from the fact that in the present study, breast problems were examined throughout the postpartum period, whereas in Gürol's study, the evaluation was made on the basis of current breast problems.
A strong positive correlation was found between the mother's breastfeeding success at the first observation, the mother's success at the second observation, and the perception scores on the breastfeeding self-efficacy scale. As the breastfeeding success scores rose, so did the breastfeeding self-efficacy perception scores. The results of the study show similarity to the findings of Yenal et al. and Gürol. In the systematic review by Meedya et al., it was reported that the duration of breastfeeding in the first 6 months postnatal depended upon the willingness of the woman to breastfeed and her self-efficacy perception.11,13,21 Such studies support our results and verify the positive correlation between breastfeeding success and self-efficacy.
Conclusion and Recommendations
This study, which was conducted to determine the correlation between breastfeeding success in the early postpartum and the perception of self-efficacy and breast problems in the late postpartum, revealed that there was a strong positive correlation between the breastfeeding success mean scores in the early postpartum and the breastfeeding self-efficacy scale total mean scores in the late postpartum. It was found that mothers with a high degree of breastfeeding success had a higher perception of self-efficacy and experienced fewer breast problems.
These results show that midwives may assess mothers' success in breastfeeding in the early postpartum period to be able to determine which women constitute a risk in terms of breast problems. The degree of success mothers in the risk group have with their breastfeeding may be increased to ensure that their perception of breastfeeding self-efficacy can be raised.
When it is considered that the study was carried out on primiparas and mothers with no prior breastfeeding experience and that it shows a lower self-efficacy perception and a lesser degree of breastfeeding success, it might be recommended that this group of mothers is provided more support in their breastfeeding and that the study be repeated in different populations. Further research is required to investigate whether low latch scores correlate to different problems other than problems associated with low self-efficacy scores.
Footnotes
Acknowledgments
This research was supported by the Research Fund of the Adnan Menderes University. Project Number: ASYO-13002. Assist. Prof. PhD. Aslı Süner from Ege University Biostatistics Department was paid to support the statistics. The authors thank the women who agreed to participate in this study for their effort and contribution.
Disclosure Statement
No competing financial interests exist.