
Abstract
Abstract
Introduction:
Recent results indicate that human mastitis and painful breastfeeding may be characterized by a mammary bacterial dysbiosis, a process in which the population of potential pathogens increases at the expense of the normal mammary microbiota. The objective of the present study is the evaluation of three different doses of Lactobacillus fermentum CECT5716 to reduce the load of Staphylococcus in the breastmilk of women suffering from painful breastfeeding.
Materials and Methods:
A randomized double-blinded controlled study with four study groups was performed. Three groups received the probiotic strain for 3 weeks at doses of 3×109 colony-forming units (CFU)/day, 6×109 CFU/day, or 9×109 CFU/day. The fourth group received a placebo of maltodextrin. The main outcome of the study was Staphylococcus counts in breastmilk. The secondary outcomes were Streptococcus, Lactobacillus, and total bacteria counts in breastmilk, immunoglobulin A and interleukin 8 concentrations in breastmilk, and breast pain scores.
Results:
At the end of the study, a significant decrease in the Staphylococcus load was observed in the probiotic groups compared with the baseline loads (p=0.045), whereas the control group maintained similar levels over time. A significant difference in the pain score was observed among the groups receiving the three probiotic doses compared with the control group (p=0.035, p=0.000, and p=0.028, respectively). A dose–response effect could not be observed because the three doses tested induced similar effects, and no significant differences were detected.
Conclusions:
We conclude that L. fermentum CECT5716 is an efficient treatment for breast pain during lactation associated with a high level of Staphylococcus in breastmilk.
Introduction
E
Mastitis is an inflammatory condition of the breast that is usually associated with lactation. The reported incidence varies from 3% to 33% and may or may not be accompanied by infection. 3 Staphylococcus has been considered the most common etiological agent of mastitis. 2 Staphylococcus aureus is related primarily to acute mastitis cases, which usually include both local (breast redness, engorgement, and pain) and systemic symptoms. However, breastfeeding women may also experience local symptoms, such as nipple/breast pain and breast engorgement not associated with fever, or other systemic symptoms. These symptoms occur in approximately 10% of all breastfeeding women and are termed subacute mastitis.2,4 This type of mastitis is typically caused by coagulase-negative staphylococci, mainly Staphylococcus epidermidis, and other bacterial agents such as Streptococcus and is generally misdiagnosed as “noninfectious” or “mammary candidiasis.” 2 In healthy conditions, breastmilk has been shown to contain physiological microbiota5–7 in which Lactobacillus, Streptococcus, Staphylococcus, Enterococcus spp., Bifidobacterium, and Enterococcus represent the predominant bacterial groups.5,8,9 Recent results indicate that human mastitis may be characterized by a mammary bacterial dysbiosis, a process in which the population of mastitis agents increases at the expense of the normal mammary microbiota. 2
Some of the lactic acid bacteria isolated from the breastmilk of healthy women exhibit the capability to inhibit the growth of a wide spectrum of pathogenic bacteria through the production of antibacterial compounds, competition for adhesion locations, and co-aggregation events, among others,10,11 and also exhibited immunomodulatory properties. 12 A previous study demonstrated that Lactobacillus fermentum CECT5716, a probiotic strain previously isolated from breastmilk, can be used as an effective treatment of mastitis by reducing pathogen counts in breastmilk. 13
The objective of the present study is the evaluation of three different doses of L. fermentum CECT5716 to reduce the Staphylococcus load in the breastmilk of women suffering breast pain not associated with acute mastitis.
Materials and Methods
Study design and protocol
A randomized double-blinded controlled study with four study groups was performed. Women suffering breast pain with lactation were recruited. Written informed consent was obtained from the women. The inclusion criteria were as follows: women with painful breastfeeding and milk bacterial counts at least 3 log10 colony-forming units (CFU)/mL. The exclusion criteria included fever, antibiotic treatment, mammary abscesses, Raynaud's syndrome, or any other mammary pathology. Exclusion criteria during the study were lack of compliance with the study protocol, antibiotic treatment, adverse effects, or voluntary decision by the women to cease participation.
The sample size was estimated based on the effect on the main outcome of the study, the bacterial counts in breastmilk. Based on previous results, 13 the study was designed to exhibit sufficient power (80%) to detect a reduction of 1 log in total bacterial counts in breastmilk after treatment with a 0.05 significance level. The number of women necessary was 20 per group.
One hundred forty-eight women were selected and distributed into four study groups, according to a randomization generated by a computer program (SIGESMU®; Ediciones DiazdeSantos, Madrid, Spain). Three groups received the probiotic strain for 3 weeks at doses of 3×109 CFU/day for Experimental Group I (EGI), 6×109 CFU/day for Experimental Group II (EGII), and 9×109 CFU/day for Experimental Group III (EGIII). The fourth group, the control group (CG), received a placebo of maltodextrin. Pills containing 3×109 CFU per pill of L. fermentum CECT5716 or maltodextrin were prepared. EGI consumed one probiotic pill per day with food, EGII consumed two probiotic pills (one pill every 12 hours taken with food), EGIII consumed three probiotic pills (taken with breakfast, lunch, and dinner), and CG consumed three pills of placebo (breakfast, lunch, and dinner). The probiotic was provided in identical pills labeled in plain white with a code number that referred to the manufacturing batch. Pills were kept at 4°C throughout the study. The concentration of viable Lactobacillus in the probiotic pills was stable throughout the study.
This study was performed in accordance with the Declaration of Helsinki, and the protocol was approved by the Regional Ethics Committee of the Sistema Andaluz de Salud, based in Seville, Spain.
Study outcomes and data collection
The main outcome of the study was Staphylococcus counts in breastmilk. Secondary outcomes were Streptococcus, Lactobacillus, and total bacteria counts, immunoglobulin A (IgA) and interleukin 8 (IL-8) concentrations in breastmilk, and breast pain scores.
Breastmilk samples were collected after 0, 1, 2, and 3 weeks of treatment. For breastmilk sample collection, the nipple and mammary areola were cleaned with soap and water, and an antibacterial (chlorhexidine) solution was applied. Breastmilk samples were obtained by manual expression; after the first drops were discarded, milk samples were collected in sterile tubes. Samples were preserved at −20°C and processed within 1 week.
A Food Frequency Questionnaire was completed by the women at the beginning and at the end of the intervention.
Breastmilk bacteria quantification
To estimate the concentration of total bacteria in breastmilk, appropriate dilutions of breastmilk in a peptone saline solution were spread in quadruplicate onto plates of PC agar (Oxoid, Basingstoke, United Kingdom). The cultures were incubated in anaerobiosis at 37°C for 48 hours. After the incubation, the colonies grown on the culture medium were counted, and the number of viable microorganism (in CFU) per milliliter of milk was calculated.
Staphylococcus, Streptococcus, and Lactobacillus counts were measured by quantitative polymerase chain reaction. The E.Z.N.A.® Stool DNA kit (Omega Bio-Tek, Norcross, GA) was used for bacterial DNA isolation. In brief, 0.5 mL of 0.5 M EDTA Tergitol™ (Dow Chemical Co., Midland, MI) surfactant (0.1% [wt/vol]) was added to 1 mL of breastmilk, and the solution was mixed and incubated for 10 minutes at room temperature. After incubation, samples were centrifuged at 14,000 g for 10 minutes at room temperature, and the supernatants and fat residues were completely removed. 14 Bacterial pellets were homogenized with 200 μL of sterile water, and each sample was transferred to a tube containing 200 mg of glass beads for DNA extraction following the instructions of the E.Z.N.A. Stool DNA kit protocol.
DNA quantification was performed by quantitative polymerase chain reaction using SYBR® green as a fluorophore (PerfeCTa® SYBR Green SuperMix with ROX™ [Quanta Biosciences, Gaithersburg, MD] for Streptococcus and Staphylococcus and Brilliant III Ultra-Fast SYBR Green QPCR Master Mix [Agilent Technologies, Santa Clara, CA] for Lactobacillus) and specific primers for each group.15–17 A common thermal profile was applied for all amplifications: 95°C for 5 minutes followed by 40 cycles of 95°C for 30 seconds, 55°C for 30 seconds, and 72°C for 35 seconds. A final melting curve was performed from 55°C to 95°C. For amplification reactions, 2 μL of DNA from every sample and bacterial group was used as template in 20 μL of final volume. Ct values (threshold cycle) were interpolated in specific calibration curves to calculate the bacterial concentrations (in CFU/mL).
IgA and IL-8 quantification in breastmilk
IgA and IL-8 concentrations were measured in breastmilk samples by enzyme-linked immunosorbent assay quantification kits following the manufacturer's instructions (Bethyl Laboratories [Montgomery, TX] and Diaclone [Besançon, France], respectively).
Pain questionnaire
The evolution of the symptoms was evaluated at 0, 1, 2, and 3 weeks of treatment. Women were asked to score their breast pain from 1 (extremely painful) to 10 (no pain).
An adaptation of the McGill Pain Questionnaire 18 validated in Spain was used. 19 The Questionnaire has four dimensions or scales of measures of intensity: Sensory Intensity Value, Affective Intensity Value, Current Intensity Value, and Evaluative Intensity Value. The scales of the Questionnaire were calculated as the sum of their items. Those items were recorded as 1 if the participant described the pain or as 0 if the participant did not report that type of pain. Thus, the sensory intensity scale can range from 0 to 33, as the full scale is formed by 33 items. The Affective scale varies from 0 to 19, and the scales of Current Intensity and Evaluative Intensity can range from 0 to 6 and 5, respectively.
Statistical analysis
Initially, statistical tests for differences in the effect of the treatment were performed using parametric (analysis of variance test) and nonparametric (Kruskal–Wallis) test statistics (depending on the assumptions that were met) when data were continuous or using the chi-squared test for binary or categorical responses. Finally, a more robust and accurate analysis via statistical modeling was performed to determine the effect of the treatment adjusted by the time and the covariates stated in the previous paragraph. Furthermore, the association of the biochemical parameters with the pain scores was studied by including these parameters as covariates when modeling outcomes related to pain. The models applied to the data were linear mixed models 20 for continuous data when the residuals were normally distributed, Poisson mixed models when the data were related to the number of events observed, and logistic mixed models when the outcomes to be analyzed were binary responses. 21 The tests were performed at the two-sided 5% significance level, and 95% confidence intervals were obtained for the estimates. The statistical software used to perform the analysis were SPSS version 19 (IBM, Armonk, NY) and R version 3.0 (http://www.R-project.org/).
Results
Population
Two hundred women were informed about the study, but only 148 women agreed to participate and were randomized for inclusion in the study. Finally, 113 women (30 in CG, 26 in EGI, 27 in EGII, and 30 in EGIII) received the treatment. Women with total bacteria counts in breastmilk of <103 CFU/mL were excluded. Before completion of the 3-week intervention, 17 women discontinued treatment due to the following: antibiotic treatment for mastitis (n=1 in CG, 2 in EGI, 2 in EGII, and 2 in EGIII), own perception of lack of improvement (n=2 in CG, 2 in EGI, and 1 in EGII), antibiotic treatment for tonsillitis (n=1 in EGII), or loss to follow-up (n=1 in CG, 1 in EGI, and 2 in EGIII). The data for these women were included in the analysis.
Therefore, data from 98 women were finally included in the analysis (27 in CG, 23 in EGI, 24 in EGII, and 24 in EGIII). A flow chart of the participants in the study is presented in Figure 1. The baseline characteristics of women of all groups were similar with the exception of the time of lactation, which was significantly lower in EGI: it was approximately half of the mean days for EGII and EGIII and with a difference of 40 days on average with respect to CG (Table 1). Interaction between treatment and this covariate was included in the modeling data analysis.
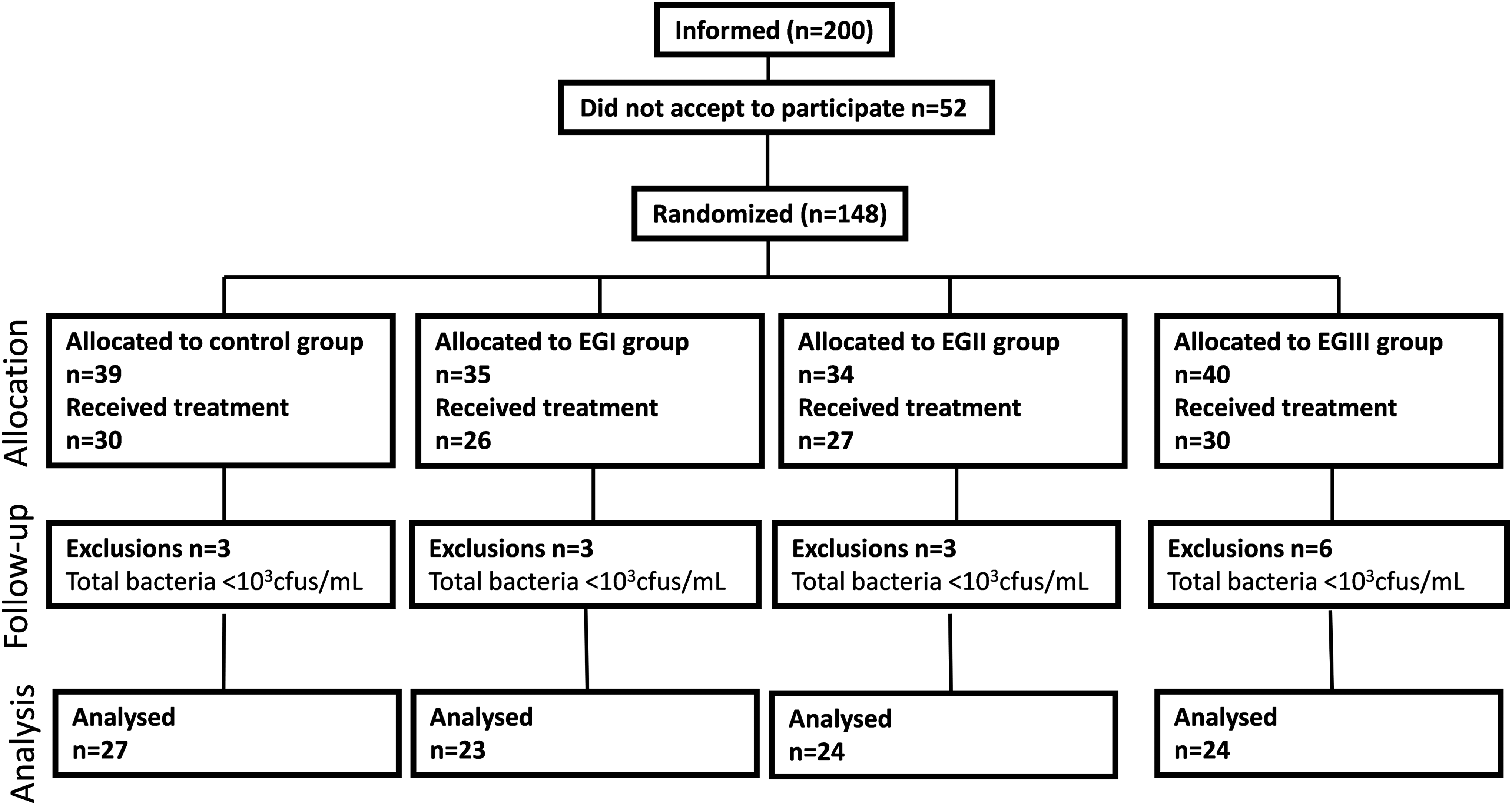
Flow chart of participants. EGI, EGII, and EGIII, the three experimental groups receiving 3×109, 6×109, and 9×109 colony-forming units (cfu)/day, respectively.
Data are mean±standard deviation values, percentages, or mean (confidence interval) as indicated.
Analysis of variance.
Chi-squared test.
Kruskal–Wallis test.
EGI, EGII, and EGIII, the three experimental groups receiving 3×109, 6×109, and 9×109 colony-forming units/day, respectively.
Participants were asked to fill in a questionnaire regarding their diets during the study period. In general, no significant differences were noted in the diets of women among the study groups or between baseline and the end of the intervention. Therefore the significant effects observed for outcomes cannot be attributed to the participants' different dietary habits.
Bacterial counts
At the end of intervention, a significant decrease in the bacterial load, estimated as 0.764, was observed in EGI compared with CG and with respect the initial point of the study (p=0.011). This result contrasts with that observed in CG, which exhibited a significant increase in the total bacterial load at 21 days of intervention with respect to the starting point of the study (Table 2). It is interesting that we noted an interaction between days of breastfeeding and bacterial load; as breastfeeding duration increased, there was a significant decrease in the bacterial load (p=0.027). Additionally, the levels of IL-8 also appear to be closely related to the bacterial load, as the latter increased as the IL-8 level significantly increased (p=0.000).
Data are mean±standard deviation values, in log10 colony-forming units/mL of milk).
p<0.05 versus basal (time 0).
p<0.05 versus control group (CG)
EGI, EGII, and EGIII, the three experimental groups receiving 3×109, 6×109, and 9×109 colony-forming units/day, respectively.
A significant decrease in the Staphylococcus load was observed at the end of the study compared with baseline loads (p=0.045) in the experimental groups, whereas CG maintained similar levels (Table 2). The estimated mean value of reduction was −1.387 for EGI, −1.736 for EGII, and slightly lower for EGIII (–0.589). Higher values of IL-8 were significantly associated with higher Staphylococcus loads (p=0.029). An interaction with the presence of nipple cracks was detected in EGI and EGII. In these groups, the reduction in the load of Staphylococcus was greater among women without nipple cracks than among women with nipple cracks (p=0.017 for EGI and p=0.039 for EGII). This interaction was also observed in EGIII, although it did not reach statistical significance (p=0.191).
With respect to Streptococcus load in breastmilk, although lower loads were observed on average for women in EGI, EGII, and EGIII versus CG, differences were statistically significant only for EGII (p=0.044) (Table 2). Higher levels of IL-8 was significantly correlated with higher Streptococcus loads (p=0.007).
No significant changes were detected in the Lactobacillus counts.
Immune parameters in breastmilk
IL-8 was measured in the breastmilk samples. In EGI, a progressive significant decrease over time was observed with respect to the IL-8 values, and the difference was significant compared with CG (p=0.003). In EGII, a decreasing trend was observed at 21 days of treatment (p=0.067) (Table 3). A strong association was detected between bacterial load and IL-8 levels. This relationship was observed for total bacteria, Staphylococcus loads, and Streptococcus loads (p=0.000, p=0.008, and p=0.007, respectively); as bacterial load increased, the level of IL-8 significantly increased between 0.125 and 0.082 units for each unit of bacterial count. Women with nipple cracks exhibited higher values of IL-8 than those without (p=0.020), and this association was independent of group.
Data are mean±standard deviation values.
p<0.05 versus control group (CG).
p=0.067 versus CG.
p<0.05 versus basal (time 0).
EGI, EGII, and EGIII, the three experimental groups receiving 3×109, 6×109, and 9×109 colony-forming units/day, respectively; IgA, immunoglobulin A; IL-8, interleukin 8.
IgA values were only recorded at the beginning of the treatment and at the end of the intervention (Table 3). At the beginning of the study, IgA levels in EGI were significantly higher than in CG (p=0.027), but at the end of the intervention, a decrease in the values was detected in EGI (p=0.036).
Evaluation of breast pain
A score of the discomfort on a scale from 1 to 10 was obtained from participants at each visit, where 1 indicated significant pain and 10 indicated no pain (Fig. 2). At baseline, there is no difference in the pain scores for the four groups (Fig. 2). Each individual group showed improvement in the pain score over time, measured on Days 7, 14 and 21, compared with baseline score (p=0.000). The three experimental groups, EGI, EGII, and EGIII, showed improvement in the pain scores over time compared with CG (P=0.035, p=0.000, and p=0.028, respectively). The effect of probiotic treatment was noticeable from the first week. An association between bacterial load and pain score was detected, as an increase in total bacterial loads led to a decrease in the score pain (p=0.029). This association was also detected for Staphylococcus load, although the interaction did not reach statistical significance (p=0.057).
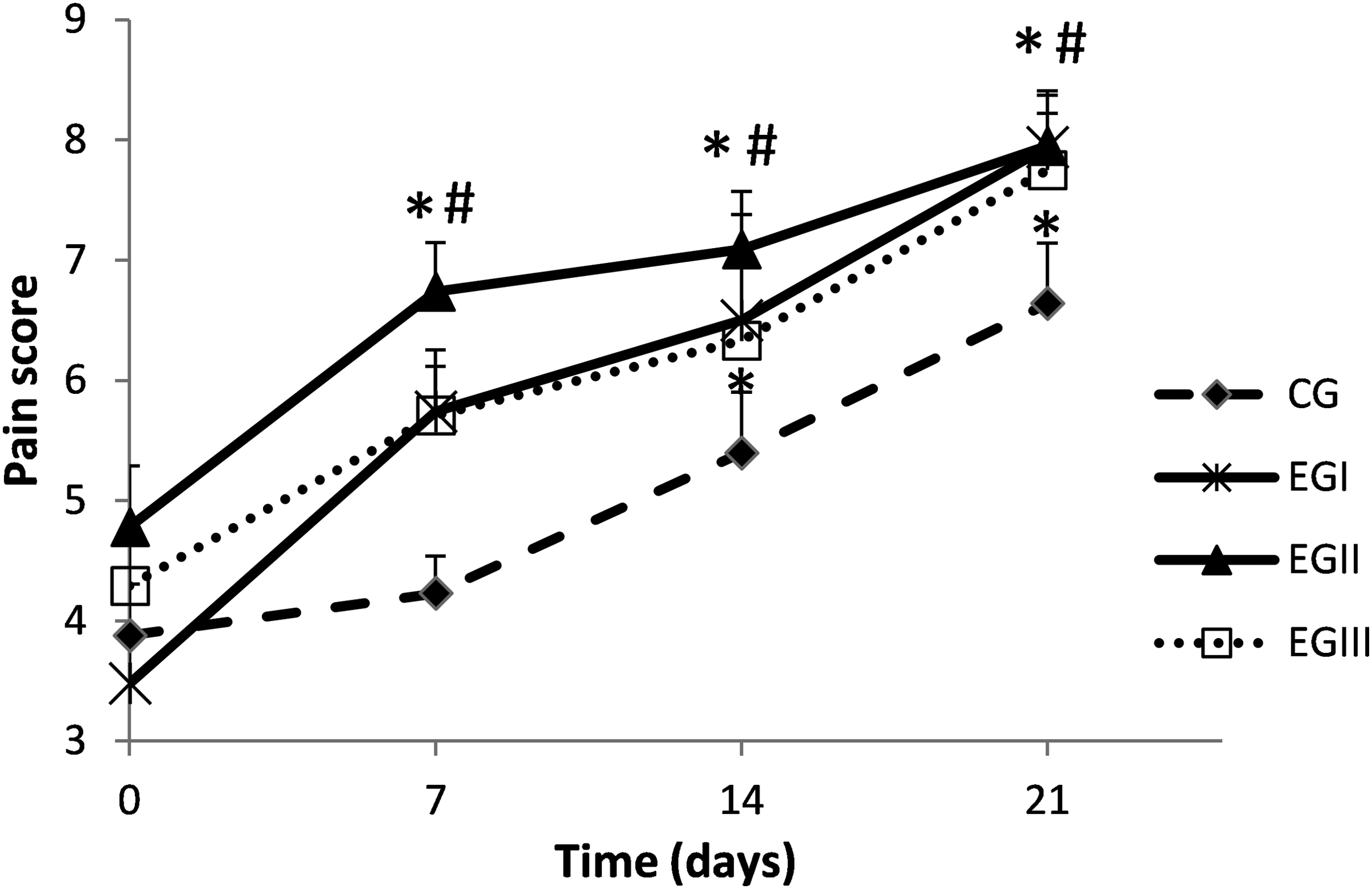
Evolution of pain over time from the pain rating scale. Data are mean±standard error of the mean values. *Significant difference, p<0.05 versus basal (time 0). #Significant difference, p<0.05 for each probiotic treatment versus the control group (CG) at each time. EGI, EGII, and EGIII, the three experimental groups receiving 3×109, 6×109, and 9×109 colony-forming units/day, respectively.
An adaptation of the McGill Pain Questionnaire was used to evaluate the pain perception. This questionnaire evaluates four dimensions of pain: Sensory Intensity Value, Affective Intensity Value, Current Intensity Value, and Evaluative Intensity Value (Table 4).
Data are mean±standard deviation values for each scale at each time of the study and for each treatment.
CG, control group; EGI, EGII, and EGIII, the three experimental groups receiving 3×109, 6×109, and 9×109 colony-forming units/day, respectively.
For the Sensory Intensity scale, the estimated mean values indicated significantly lower pain for the experimental groups EGI, EGII, and EGIII than for the CG (p=0.000, p=0.001, and p=0.040, respectively). IL-8 was identified as a covariate that influences the Sensory Intensity scale, as the load of IL-8 increased 1 unit as the average value of the pain scale increased by 0.63 (p=0.037). At the beginning of the study, women mainly described their pain on the punctate/incisive pressure subscale; between 83% and 92% of women selected at least one item in this subscale.
For the Affective Intensity scale, a significant effect of the treatment was observed in EGI and EGII (p=0.011 and p=0.010, respectively). The subscale of anger/disgust was typically used to describe the feelings related to the pain; between 78% and 100% of women in the study described this feeling at the beginning of the study. At the end of the intervention the percentage of women reporting this item in the experimental groups was 42% lower than in CG. Items on the subscale of fear (fearful, frightful, terrifying) were selected by 57–85% of women at the beginning of the intervention. At the end of the treatment the percentage of women reporting this item in the experimental groups was 62.3% lower than in the CG. Similar results were observed in the case of feelings related to grief and anxiety.
The treatment exhibited a significant effect on the evaluative intensity of pain (temporary, intermittent, increasing, constant, persistent). In particular, EGI and EGII reported a 30% reduced incidence on this scale versus CG (p=0.035).
No significant changes were detected on the Current Intensity scale.
Occurrence of gastrointestinal disorders and pharmacological treatments
The occurrence of diarrhea or flatulence was recorded in the questionnaire completed by women. No significant differences were detected with respect to diarrhea (p=0.718) or flatulence (p=0.905) incidence among the groups.
Analgesic consumption decreased progressively throughout the study in all groups; however, women in EGIII consumed significantly fewer analgesics than women in CG (p=0.046).
Discussion
Traditionally, S. aureus has been considered the most common etiological agent of mastitis; however, recent studies have suggested that other microorganisms, such as coagulase-negative Staphylococcus, are related to mastitis and breast pain during lactation.4,22 Previous studies demonstrated the capability of certain Lactobacillus strains to reduce the bacterial load in the breastmilk of women suffering mastitis. 13 One of these strains is L. fermentum CECT5716, a strain isolated from human milk. The present study evaluated the effect of three different escalating doses of the L. fermentum CECT5716 strain on bacterial load in the breastmilk of women suffering breast pain symptoms compatible with subacute mastitis. The Lactobacillus consumption significantly reduced the Staphylococcus load in breastmilk. The total bacteria and Staphylococcus loads were significantly correlated with the perception of breast pain of the women, demonstrating that alterations in breastmilk microbiota are directly related to the symptoms of pain in this disease. The bacterial load was also strongly correlated with the level of IL-8 in breastmilk. This cytokine elicits the infiltration of immune cells to the site of infection, and its concentration in human milk has been proposed as an effective indicator of mastitis. 23 The presence of physiological microbiota in human milk is a relatively recent discovery,5,6 and the number of studies dealing with the microbiological aspects of human mastitis is few. The present work demonstrates the correlation between the bacterial load of certain bacterial groups in breastmilk and the occurrence of breast pain during lactation.
According to these associations between Staphylococcus load and breast pain, the reduction in the bacterial load induced by the administration of L. fermentum CECT5716 significantly reduced breast pain in women. A strength of this study compared with previous research is the inclusion in the protocol of intermediate measures of different parameters. This design, besides the advantages of a model of repeated measures, has allowed us to demonstrate that the effects were noticeable from the first week of treatment. Another strength of the study is the inclusion of a validated pain questionnaire that evaluated the sensorial aspects of pain as well as the affective dimension of pain. In this sense, women in the study described their pain before intervention with adjectives related to anger, fear, and anxiety. The Lactobacillus treatment significantly improved this assessment in the women. This is an important aspect of the study because the emotional distress causes by mastitis can lead to the cessation of breastfeeding.
Although a significant increase in Lactobacillus counts in breastmilk could not be detected in women consuming the Lactobacillus strain, the presence of the strain in breastmilk after oral administration has been previously demonstrated. 13 The relatively low counts of Lactobacillus versus Staphylococcus in the breastmilk samples suggest that the mechanism for the decreased pain is unlikely to be simply a “competition phenomenon.” Some authors have suggested that host innate immune responses activated in the mammary gland are a critical feature of mastitis disease and that mastitis could be the result of an inflammatory response to an otherwise innocuous bacterium. 24 In fact, although S. epidermidis was common in the breastmilk of women suffering mastitis, strains of this species can also be found in milk of healthy women.6,8,22 With respect to the role of the immune system in mastitis, the effect of probiotic strains on this pathology has been related to an effect on the immune response.25,26 L. fermentum CECT5716 has been shown in previous studies to possess immunomodulatory capabilities. For example, the strain exhibited anti-inflammatory activity in animal models of inflammation27,28 and immuno-enhancing activity in an intervention study in humans. 29 The immunomodulatory properties of L. fermentum CECT5716 may contribute to the effect of the strain on mastitis.
A dose–response effect could not be observed because the three doses tested induced similar effects, and no statistically significant differences were detected. The fact that three doses tested range over the same magnitude order, 9 log, could be a limitation of the study. We cannot exclude the possibility that a significantly higher dose of Lactobacillus could lead to a dose-related response. We conclude that the current dosing of lactobacilli, at a level of 3×109 CFU/day is effective and sufficient to produce a decrease in staphylococcal load in breastmilk leading to improvement in pain symptoms in women suffering from breast pain associated with Staphylococcus in the breastmilk.
Footnotes
Acknowledgments
The authors wish to thank Matilde Palomares Cuadrados, Maria José Gomáriz, Rosa Hoyas Romero, Isaura González, Maria Jesús Gil, and Carmela Santamaría Palacios, midwives of Spanish Health Services and Breastfeeding Support Associations (Mamilactancia and Grupo Apoyo Multilactancia), for their collaboration in the study and Llenalia García Fernández (SEPLIN, Soluciones Estadísticas) for the statistical analysis of the data. J.A.M.-L. was the recipient of a fellowship from the Fundación Universidad-Empresa (Universidad de Granada, Granada, Spain). This work is part of his doctoral thesis entitled “Lactobacillus fermentum CECT5716: An ally during lactation” (Programa de Doctorado en Nutrición y Ciencias de los Alimentos [B14.56.1]).
Disclosure Statement
J.A.M.-L., M.P.D.-R., A.D.V., A.S., L.S., O.B., J.F., and M.O.M. are employees of Biosearch, which is the owner of the patent for L. fermentum CECT5716. M.A.D.-L., R.C., P.D., and M.D.R.-L. declare no competing financial interests exist.