
Abstract
Abstract
Background:
Suction pressure has been reported to be a key driving force of lactation. An infant's sucking at its mother's breasts is the major stimulus to post-natal prolactin (PRL) secretion, and PRL is the essential hormone for lactation and milk production. It is unknown what role suction pressure has in PRL secretion and milk supply postnatally.
Objectives:
To explore the relationship between the suction pressure, PRL level, lactation, and milk supply in breastfeeding mother-infant dyads.
Methods:
Healthy women with normal full-term infants were enrolled (n = 122). Data collection included suction pressure, PRL level, and the mother's perception of both the onset of her lactation and her milk supply at 1 month. Suction pressure was measured with a pressure sensor connected to a tube placed alongside the nipple. The chemiluminescence method was used to quantify maternal serum PRL level both before and after a breastfeed to explore the effect of suckling on PRL increment. The mother's perception of the onset of her lactation was evaluated by the mother's sense of fullness in her breast. The mother's perception of milk supply was evaluated by using the H&H Lactation Scale.
Results:
Data from 117 participants were included in this analysis. Low suction pressure, a shorter gestational age, a high pre-gestational body mass index (BMI), and high infant birth weight were associated with a smaller than average PRL increment. High suction pressure, longer sucking duration, and a low gestational weight gain were related to a mother's perception of an earlier onset of her lactation. However, low suction pressure, a high frequency of giving formula, a small PRL increment, and the mother's perception of a later onset of her lactation were correlated with her perception of an insufficient milk supply.
Conclusions:
Suction pressure varied directly with the post-natal PRL increment. Suction pressure was associated with the timing of the mother's perception of her lactation. Strong suction pressure by the infant is likely to enhance the mother's confidence in her lactation. Additionally, sucking duration, frequency of giving formula, maternal BMI, and infant birth weight played a role in early breastfeeding success.
Introduction
B
Numerous factors impact the onset of lactation and milk supply, and these factors can be roughly divided into two categories. Factors pertaining to early sucking, such as sucking behavior, 7 sucking frequency within 24 hours of birth, 8 and giving formula within 48 hours, 9 are reported to be correlated with the onset of lactation and milk supply. However, other factors, such as parity, maternal age, 10 maternal body mass index (BMI),10,11 administration of exogenous oxytocin, 11 and gestational glucose tolerance, 10 are all associated with the endocrine changes linked to lactation. However, it is unknown how the infant's sucking at the breast interacts with the endocrine response in lactation and with subsequent milk production.
It has been verified that post-natal prolactin (PRL) is the essential hormone that is necessary for the initiation of lactation and galactopoesis. 12 PRL secretion is stable from 7 to 24 hours postpartum. During this period, PRL levels are not affected by anesthetic or operative stress. 13 The strength, duration, and frequency of the infant's sucking at the mother's breast are the main stimuli for maintaining PRL secretion postnatally. 14 The suction pressure, generated as the posterior tongue moves downward during breastfeeding, has been imputed to be the main driving force transferring the milk from the breast. 15 Kron et al. discovered that infants whose mothers received obstetric sedation during labor had a lower suction pressure and consumed less milk than those born to mothers who received no obstetric sedation. 16 Therefore, suction pressure may be influential to PRL secretion, lactation, and milk supply postnatally. However, few studies have explored how the suction pressure interacts with PRL level, the initiation of lactation, and milk supply.
This study is intended to explore the relationship between suction pressure, PRL, and the mother's perception of both the onset of her lactation and her milk supply at 1 month in breastfeeding mother-infant dyads.
Methods
Subjects and recruitment
This observational study was carried out in The Affiliated Hospital of Nantong University. This is the largest comprehensive university teaching hospital in Nantong city. The hospital has more than 2,000 beds, in which the number of delivered infants accounts for 21% of the total births in Nantong. Healthy single-birth primiparas, aged from 20 to younger than 35 years, were recruited. The women delivered normal full-term infants and initiated breastfeeding. Puerperas with any of the following conditions were excluded: multiparity, breastfeeding contraindications, mother-infant separation, artificial feeding, breast surgery/injury history, mammary dysplasia, flat or inverted nipples, smoking, or obesity (pre-gestational BMI >27 kg/m2). Additionally, the mothers were required to be free from gestational diabetes mellitus, diabetes, hypertension, hypothyroidism, hypopituitarism, ovarian theca-lutein cyst, polycystic ovarian syndrome, postpartum hemorrhage, infectious disease, and any other condition that might impede successful breastfeeding or lactation.
Recruitment was from July 2014 until the target sample size was achieved in August 2015. The protocol was approved by the Ethics Committee of Nantong University (No. 2014-069) and was registered in the Chinese Clinical Trial Registration (No. ChiCTR-OOC-14005294). Written informed consent was obtained from all participants before enrollment. Verbal and written information regarding the aim and procedure was given to all participants; they were also informed that they were free to withdraw from the study at any time, without declaring any reason for doing so.
Data collection
Suction pressure
According to the method of Geddes et al., 15 suction pressure was measured through a tube (450 mm, 1.3 mm i.d. × 2.7 mm o.d.) placed alongside the nipple, with the other end of the tube connected to a pressure sensor (TCT-1202; Lenosensor Co., Ltd, Beijing, China). As per calibration certificate (No. Jing 01120018), the pressure sensor has a 0.5% accuracy and a 0.02% repeatability error. Using data analysis software (M400; Lenosensor Co., Ltd, Beijing, China), the pressure curve was depicted, and peak suction pressure (the maximum pressure), baseline suction pressure (the minimum pressure), and mean suction pressure (the average of all suction pressures within 30 seconds) were calculated for each infant.
To maintain the infant's readiness to suck, the measurement was taken 2 hours after the preceding breastfeeding. First, the infant's readiness to suck was evaluated by the Chinese Version of the Infant Breastfeeding Assessment Tool (IBAT). 7 The measurement began only if the infant was sucking with no stimulation, or just by unbundling, patting, or burping the infant. A specialist nurse ensured correct positioning, attachment, and sucking of the infant on the breast. The puerpera was lying on bed in a lateral position for the measurement. The detection period lasted for 30 seconds during a breastfeeding session. If the nurse had to unbundle, rub, or rock the infant vigorously at the beginning or during the feeding, or the infant could not be roused, we would define the infant as being unwilling to suck. We tried again at the infant's next feeding. Suction pressure was measured only once in the first 24 hours after delivery before the onset of lactation.
PRL
The blood sample of puerpera was collected within 20–24 hours postpartum when the breast has experienced several episodes of sucking stimulus. Considering the clearance of PRL, 17 we established a 2 hour minimum interval since the preceding breastfeeding to avoid its influence on PRL concentration. Blood was taken immediately before and 20 minutes after sucking. PRL was measured by using the chemiluminescence immunoassay method. 18 The PRL increment (PRL level after sucking − PRL level before sucking) was calculated to explore the effect of suction pressure on endocrine secretion.
Mother's perception of the onset of her lactation
Beginning at 24 hours and continuing every 4 hours, including the night hours until the onset of lactation, mothers were questioned regarding if and when they noticed a “sudden feeling of fullness” in their breasts19,20 to confirm the onset of lactation. It is a traditional method based on the maternal experience of when her breasts feel “noticeably fuller” on a 1–5 scale (where 1 = no change since giving birth, 3 = noticeably fuller, and 5 = uncomfortably full). 11
Mother's perception of her milk supply at 1 month
Milk supply was indirectly evaluated by the mother's perception by using the Chinese Version of the H&H Lactation scale, 7 which has been reported to predict breastfeeding duration and exclusivity. 4 Because lactation is stable (few changes in amount and composition of milk) at 1 month after delivery, 21 the mother's perception of her milk supply was evaluated at this time. Twenty items were measured on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores representing greater satisfaction in lactation. The content validity index of this instrument is 0.98; the internal consistency is 0.93; and the predictive validity is 0.42.
Prenatal, delivery, and postnatal data
A wide range of variables were investigated as potential confounders of the onset of lactation or milk supply. Demographic factors, including maternal education, household income, residence, marital status, and maternal age, were all considered. Prenatal data, method of delivery, and postnatal data, consisting of pre-pregnant BMI, gestational weight gain, frequencies of antenatal care, delivery mode, anesthesia, and maternal postnatal depression, were assessed. Furthermore, the following were also measured: infant birth weight, gender and gestational age (GA), the time of first sucking and skin-to-skin contact after delivery, sucking frequency and sucking duration within 24 hours, formula supplement within 24 hours, and postpartum length of hospital stay. Breastfeeding frequency 22 refers to the number of breastfeeds in a 24-hour period. If the sucking was intermittent, we would record sucking duration as one sucking episode. The mother's emotional well-being 3 days after delivery was measured by using the Chinese Version of the Edinburgh Post-natal Depression Scale (EPDS). 23 EPDS is a 10-item self-report scale designed as a specific instrument to screen postnatal depression. This scale measures feelings of guilt, sleep disturbance, low energy level, anhedonia, and suicidal ideation. Higher scores indicate more depressive symptoms.
Statistical analysis
The sample size was calculated based on the relationship between suction pressure and the mother's perception of the onset of her lactation. The method of Dupont and Plummer 24 was used to design the study in which the data were intended to be analyzed by linear regression. A two-sided level of significance of 0.05 and a power of 0.9 was set. Thirty-three samples were collected in the preliminary research, and a 0.35 regression weight was achieved between suction pressure and the mother's perception of the onset of her lactation. Factoring in a 10% increase in sample size to account for any dropout, and a 20% increase for the lack of precision in the measurement of the onset of lactation, 122 subjects were estimated to be needed.
The data were imported into Epidata3.1 and analyzed with Stata10.0. Continuous variables with normal distribution were presented as mean and standard deviation and abnormal distribution data with median and inter-quartile range. PRL levels were analyzed as log-transformed data. The regression method was adopted for missing data imputation.
Bivariate correlation was adopted to identify potential factors associated with PRL increment, the mother's perception of both the onset of her lactation and her milk supply.
To explore the relationship between PRL increment and suction pressure, a multivariate regression model was developed and adjusted for known potential confounders, including pre-gestational BMI, delivery mode, time to first breastfeeding, sucking duration, and frequency of giving formula. Additional subject variables identified in the bivariate analysis (p < 0.10), such as infant birth weight, giving formula before onset of lactation, and GA, were retained in the initial multivariate regression model as determined by a backward selection process (retention cut-off, p < 0.05). The same method was adopted for the analysis between suction pressure and the mother's perception of her onset of lactation; and between suction pressure and the H&H Lactation Scale.
Results
Mother and infant characteristics
Of the 529 evaluated subjects, 233 were eligible for inclusion. One hundred and eleven mothers (47.64%) declined to participate in this study. The predominant reason for refusal was their unwillingness to be disturbed during breastfeeding. There was no difference in the baseline information between those who accepted and those who declined to take part in the study: age (t = −1.42, p = 0.16), nationality (χ2 = 1.78, p = 0.18), place of residence (χ2 = 0.88, p = 0.35), education (χ2 = 0.66, p = 0.42), and employment (χ2 = 1.46, p = 0.23). Among the 122 enrolled, three mothers withdrew because of their unwillingness to have a blood sample drawn and two infants were unwilling to suck. The PRL data for these five were incomplete (Fig. 1). Finally, 117 subjects were included in the statistical analysis.
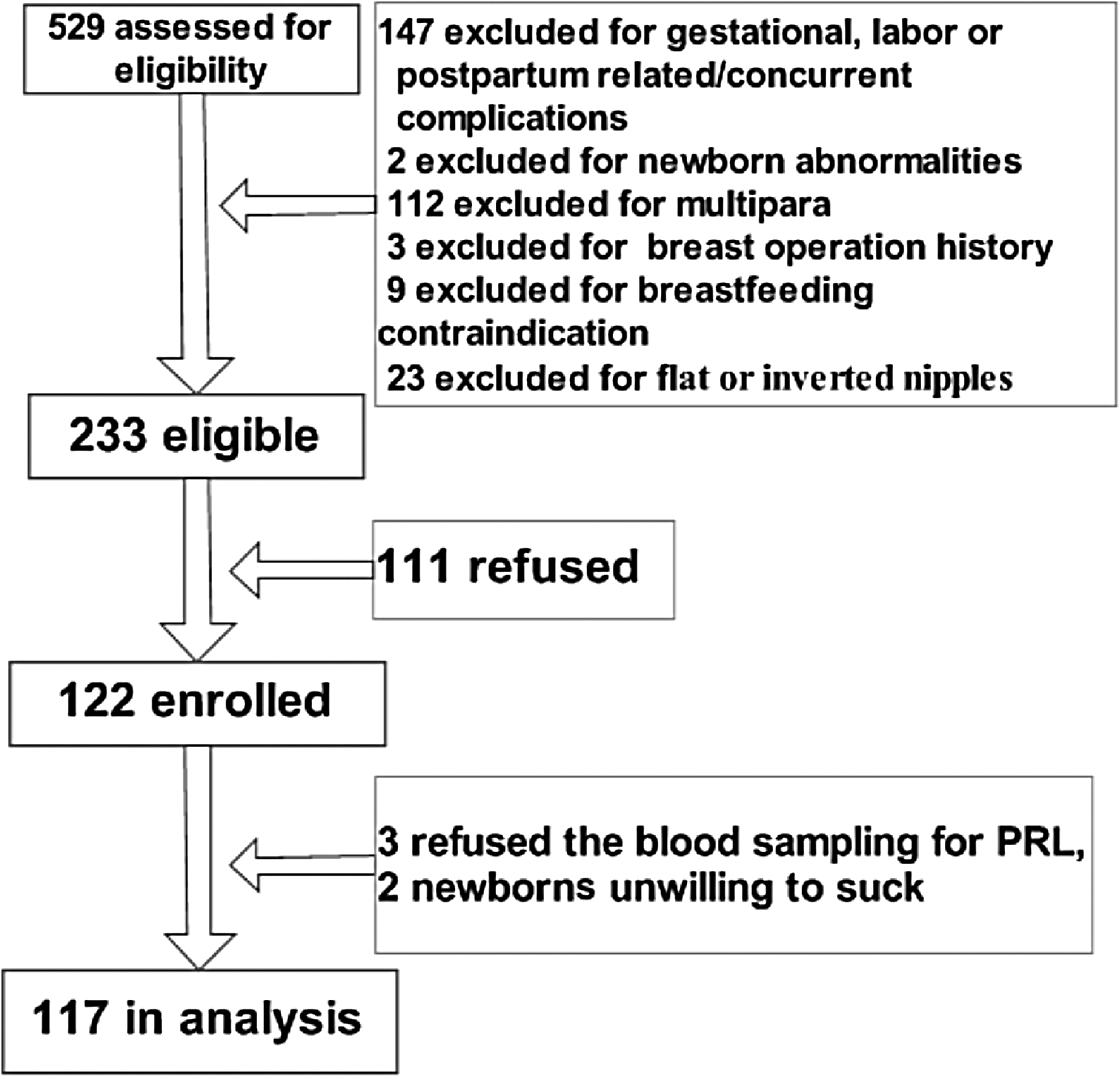
Study profile of mother-infant dyads flow. PRL, post-natal prolactin.
The peak, the mean, and the baseline suction pressures were −15.4 ± 7.2 kPa, −8.5 ± 4.1 kPa, and −1.7 ± 1.6 kPa, respectively. The level of PRL before sucking was 246.5 ± 81.5 μg/L, spiking to 314.3 ± 101.9 μg/L after sucking. The mother's perception of the onset of her lactation was an average of 59.5 ± 14.3 hours postpartum (Table 1). At 1 month, the exclusive breastfeeding rate was 44.4% (n = 52).
PRL increment = PRL level after sucking − PRL level before sucking.
M, median; Q, interquartile; PRL, post-natal prolactin.
Potential variables to PRL, mother's perception of both onset of her lactation and her milk supply at 1 month by bivariate correlation
Pre-gestational BMI, infant birth weight, delivery mode, time to first breastfeeding, sucking duration, giving formula before onset of lactation, postpartum hospital stay, and suction pressure were each related to PRL increment. Delivery mode, time to first breastfeeding, sucking duration, frequency of giving formula, PRL increment, and suction pressure were related to the timing of the mother's perception of onset of her lactation. Meanwhile, delivery mode, time to first breastfeeding, sucking duration, frequency of giving formula, PRL increment, and suction pressure were related to the mother's perception of her milk supply by bivariate correlation (Table 2).
Bivariate correlation was used to explore the potential variables of PRL increment, the mother's perception of both the onset of her lactation and her milk supply. PRL was analyzed in its log-transformed data.
BMI, body mass index; EPDS, Edinburgh Post-natal Depression Scale; GA, gestational age.
Relationships between suction pressure and PRL increment, mother's perception of both the onset of her lactation and her milk supply in multivariate regression models
Suction pressure, pre-gestational BMI, GA, and infant birth weight were statistically related to the PRL increment. Specifically, low suction pressure, short GA, increased pre-gestational BMI, and high infant birth weight were associated with a small PRL increment (Table 3). High suction pressure, long sucking duration, and low gestational weight gain were related to a mother's perception of an earlier onset of lactation (Table 4). However, low suction pressure, a small PRL increment, a high frequency of giving formula, and a mother's perception of a later onset of her lactation were related to the mother's perception of her insufficient milk supply (Table 5).
Pre-gestational BMI, GA, newborn birth weight, delivery mode, time to first breastfeeding, breastfeeding duration, giving formula before onset of lactation, and suction pressure were taken as independent variables when analyzed as potential variables to PRL increments. Four variables, pre-gestational BMI, GA, newborn birth weight, and suction pressure, were related to the PRL increment. PRL was analyzed in its log-transformed data.
Gestational weight gain, delivery mode, time to first breastfeeding, breastfeeding duration, frequency of giving formula, suction pressure, cracked nipple, and PRL increment were taken as independent variables when analyzed as potential variables related to the mother's perception of her onset of lactation. Gestational weight gain, sucking duration, and suction pressure were related to the mother's perception of her onset of lactation. PRL was analyzed in its log-transformed data.
Delivery mode, mother's perception of the onset of her lactation, time to first breastfeeding, breastfeeding duration, frequency of giving formula, volume of giving formula, suction pressure, and PRL increment were taken as independent variables when analyzed as potential variables related to the mother's perception of her milk supply. The mother's perception of the onset of her lactation, PRL increment, frequency of giving formula, and suction pressure were related to the mother's perception of her milk supply. PRL was analyzed in its log-transformed data.
Additionally, suction pressure, pre-gestational BMI, GA, and infant birth weight explained 36.3% of the PRL increment; suction pressure, sucking duration, and gestational BMI explained 43.2% of the mother's perception of the onset of her lactation; and suction pressure, frequency of giving formula, PRL increment, and the mother's perception of the onset of her lactation accounted for 40.5% of the mother's perception of her milk supply at 1 month (Tables 3–5).
Discussion
Suction pressure and PRL
PRL, secreted by the anterior pituitary gland, participates in the initiation of lactogenesis stage II (onset of lactation). The inhibitive effect of placental steroid hormones on PRL disappears shortly after the separation of the placenta, thereby triggering the onset of milk synthesis. 14 Continued sucking then becomes the major stimulus to PRL secretion postnatally, promoting the stabilization and maintenance of milk synthesis. 12 In the present study, our findings indicated that PRL levels rose with infant sucking, and the scale of increment in its serum concentration is predominantly related to the infant suction pressure (baseline, mean, and peak). Though there is a lack of direct evidence about the causal relationship between suction pressure and PRL secretion existing in humans, a previous study has implied that there is an association between the frequency of sucking, PRL level, and milk supply. Bruna et al. 25 reported a linear correlation between milk transfer and serum concentrations of PRL (r = 0.37, p < 0.05) in lactating goats after 15 minutes of the kids' sucking. Hill et al. 26 confirmed that PRL and frequency of breast stimulation positively influenced milk production in humans. After 20 minutes of the babies' sucking, PRL concentration peaked within 20 minutes. 26 Therefore, suction pressure plays its role in PRL increments after the separation of the placenta.
Interaction between suction pressure, mother's perception of both the onset of her lactation and her milk supply at 1 month
By multivariate regression, suction pressure was positively correlated to the mother's perception of her milk supply at 1 month. It is no doubt that postnatal sucking is responsible for the establishment and maintenance of lactation in the early postnatal weeks. Additionally, an infant's sucking sustains the mother's milk supply in line with her infant's demand. Despite difficulties in distinguishing the relative importance of suction pressure, frequency and duration of suction, Matthews pointed out that correct positioning, attachment, and effective sucking, 27 which guaranteed an airtight oral cavity and a negative oral pressure, were all essential to successful breastfeeding. Furthermore, Kron et al. observed that infants with a weaker suction pressure consumed less milk. 16 This indirect evidence, therefore, is consistent with our findings, which implies that suction pressure plays a role in lactation.
Another explanation of the relationship between suction pressure and milk supply might be that sucking vigor affected the mother's confidence in breastfeeding. Previous literature supported the contention that maternal breastfeeding confidence was a significant predictor of the duration and level of breastfeeding. 28 Duckett et al. 29 reported that breastfeeding intention, Perceived Behavioral Control (mother's judgment about the degree to which she can successfully implement breastfeeding), and the mother's perception of her milk supply were predictors of breastfeeding duration. These variables explained 30% of the breastfeeding duration.
The mother's confidence in breastfeeding could also account for the unexpected findings that suction pressure was predominately correlated with the mother's perception of the onset of her lactation. It is known that the onset of lactation is triggered by delivery of the placenta. However, the correlation of the onset of lactation to suction pressure in this study may be because the onset of lactation was judged by maternal perception, rather than by test-weighing or using a biomarker. Mothers are usually aware of their infants' sucking strength, so infants with a strong suction pressure may enhance their mother's confidence in the onset of her lactation and their satisfaction with breastfeeding. Therefore, suction pressure may be a cue that the mother can use to evaluate her breastfeeding. It indicates that, although physiological factors may be paramount, the mother's emotional satisfaction may exert an important effect.
However, to our knowledge, there are no previous reports about the interaction between suction pressure and PRL, the mother's perception of both the onset of her lactation and her milk supply at 1 month.
Role of the frequency of giving formula, maternal BMI, and infant birth weight
Findings suggest that a high frequency of formula supplement is related to a mother's perception of insufficient milk supply. It is reported that mothers became more likely to use formula or to use formula earlier if they have been exposed to formula company information. 30 The unnecessary use of formula supplements should be avoided to facilitate breastfeeding. 31
A high infant birth weight is correlated with an excessive maternal gestational weight gain, 32 and maternal overweight could diminish the PRL response to suckling postpartum. 33 Therefore, our finding that the infant birth weight was negatively associated with the increase in PRL concentration could be explained. Additionally, high pre-gestational BMI has been reported to be a risk factor for the duration of breastfeeding. 34 Hence, maternal BMI and infant birth weight might impact the maternal endocrine response and, in turn, the milk supply.
Implications for practice
The findings of our study have highlighted the importance of suction pressure to breastfeeding. Measures should be taken to ensure an effective sucking strength, such as correct positioning, attachment, and airtight intra-oral space. A mother's perception of her infant's sucking in the first week can have a marked influence on her confidence in breastfeeding success; this is also seen in her confidence in milk supply at 1 month, and hence in her likelihood of sustaining breastfeeding in the long term. The clinical message should be that everything should be done to encourage and sustain the mother's confidence in her breastfeeding efficacy, effectiveness, and success. Furthermore, our observations imply that an effective sucking stimulus includes both sucking strength and sucking duration. Interventions aimed at suction pressure and sucking duration might be considered for infants who are at a risk of insufficient milk supply. Finally, the giving of formula was associated with the mother's perception of her milk supply being insufficient at 1 month. Therefore, controlling the giving of formula is suggested in the early stages of breastfeeding.
Limitations
The onset of lactation and milk supply were evaluated by maternal perception. The weighing method before and after each breastfeeding within 24 hours was not used because of parent rejection. This may have biased the results. In consideration of the potential risk to sucking behavior and the parents' unwillingness to a prolonged measurement duration, the detection lasted for only 30 seconds. Other limitations for the present study were the small sample size and the low response rate (52.36% of the eligible mother-infant dyads participated in this study). Additionally, our observational study design limited the ability to determine the directionality between suction pressure, PRL increment, and milk supply. Future interventional studies deserve exploring their causal effect.
Footnotes
Acknowledgments
This work is supported by the Nursing Scientific Research Fund of Fudan University (program No. FNF201422). The authors would like to thank English teacher Richard Riggio and Meijuan Ge for their language assistance and Chao Yu for his technological support in PRL detection.
Disclosure Statement
No competing financial interests exist.