
Abstract

Introduction
T
A new framework to characterize the current American mother–infant dyad.
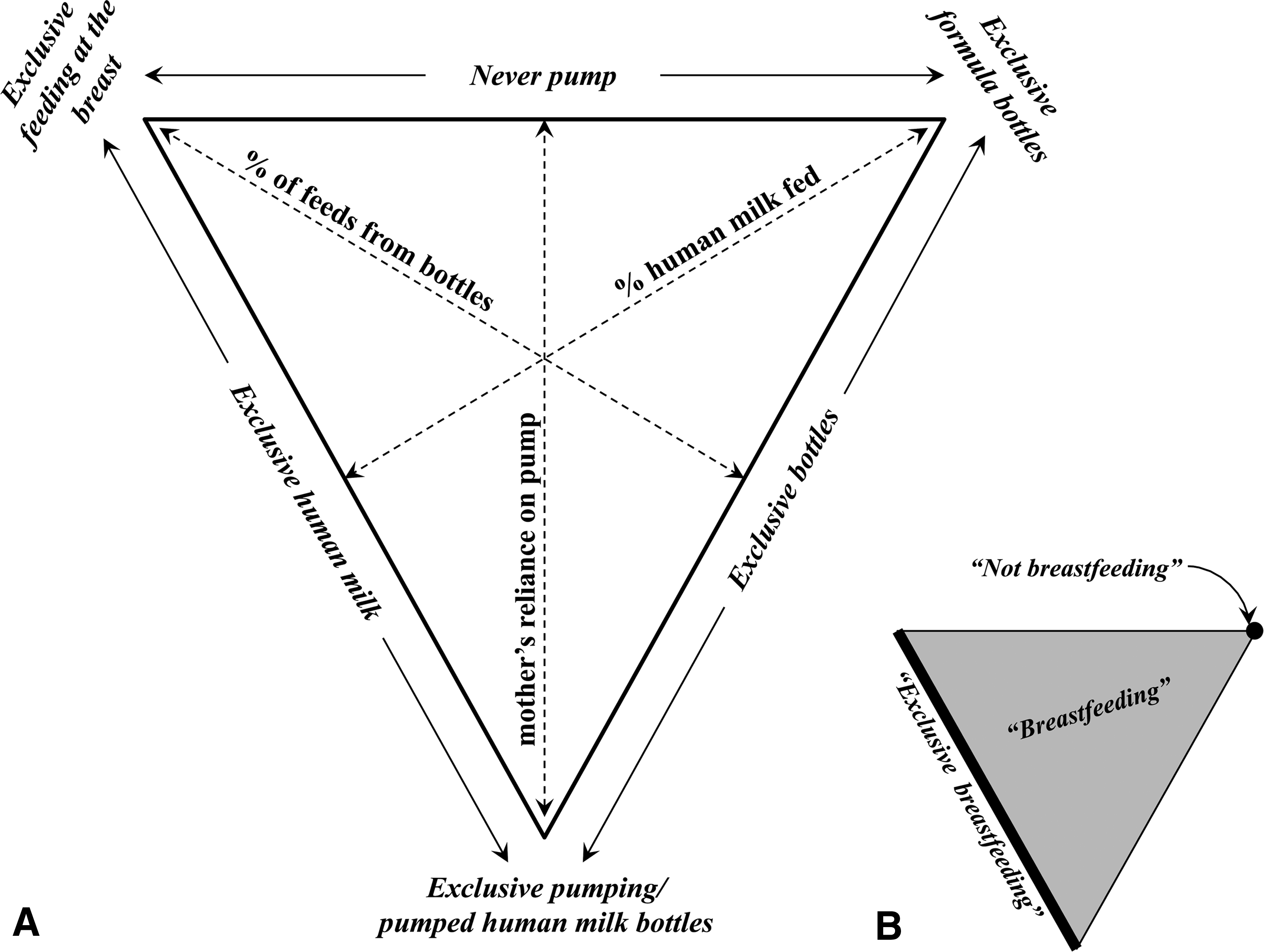
Researchers, health professionals, and policymakers now must consider three distinct practices: feeding at the breast, removing milk from breasts with pumps, and feeding pumped milk to infants (Fig, 1A). The terms “breastfeeding” and “exclusive breastfeeding” (Fig. 1B) are no longer adequate to describe or prescribe practices for providing human milk to infants because they include both feeding at the breast and feeding pumped milk but ignore pumping. For example, a mother who only feeds her infant at the breast and a mother who only feeds pumped milk (Fig. 1A) are both “exclusively breastfeeding” and their infants are both “exclusively breastfed.” A mother who feeds mostly infant formula and a nominal amount of pumped milk is “breastfeeding,” and her infant is “breastfed.” As a consequence, available data are insufficient to distinguish the contributions of feeding at the breast, feeding pumped human milk, feeding formula, and pumping to outcomes for mother and infant.
Limited available data indicate that pumping is pervasive and here to stay. The only U.S. national data available on pumping come from a longitudinal national survey cohort, the Infant Feeding Practices Study II (IFPS II), conducted from 2005 to 2007. 3 Among IFPS II mothers who fed human milk, fully 92% pumped their milk at some point in the first year postpartum, 6% never fed their human milk directly at the breast, and more than half of mothers who pumped started pumping in their first week postpartum. 2 The Affordable Care Act, 4 which mandates coverage of breast pumps, was implemented after the IFPS II data were collected. Thus, pumping rates are likely now higher because mothers who were previously unable or unwilling to purchase pumps are now more likely to acquire and use them.
Until public support for feeding at the breast rises and obstacles to feeding at the breast fall, the use of pumps and bottles to provide human milk will likely continue to increase. Thus, it is urgent that health professionals, researchers, and policymakers understand how and why mothers pump their milk, how and why they and other caregivers prepare and bottle feed that milk, and how these practices affect long-term feeding practices and health outcomes.
What Is Known, and What Must Be Known, About the Determinants, Practices, and Potential Consequences of Pumping and Bottle Feeding Human Milk
Data from the IFPS II,2,5–8 from our mixed-methods, longitudinal investigation,9,10 and from other investigators11,12 provide early insights into the potential consequences of pumping and bottle feeding human milk. These data support the possibility that pumping and bottle feeding human milk modify the benefits of feeding at the breast to infants and may confer additional risks.
Pumped milk may not provide the same immunological protection as milk from the breast and may pose risk of infection. Experimental indicates that pumped milk has more contamination11,12 and less immunologic activity 13 than milk fed at the breast. Infants in the IFPS II who were bottle-fed pumped milk had more episodes of coughing and wheezing 14 than those fed at the breast.
Infants fed pumped milk may have suboptimal growth compared with infants who fed directly at the breast. This may result from both suboptimal nutritive properties of pumped milk and suboptimal methods by which it is bottle-fed to infants. Available experimental data suggest that pumped milk is lower and more variable in its energy and fat concentration15–17 than milk directly from the breast. Furthermore, infants in the IFPS II who were bottle-fed human milk early in infancy emptied their bottles more often 7 and gained weight more rapidly 8 by the end of their first year than infants who were fed at the breast. Our qualitative work may shed light on this phenomenon. Infants in our sample were fed human milk less responsively from bottles than they were at the breast (e.g., at prescribed times and with prescribed bottle amounts). 9 It is also notable that infants in a recent prospective cohort who were bottle-fed pumped milk in the hospital were less likely to be fed human milk at 6 months than infants who had only been fed at the breast in the hospital. 18
To understand how pumping and bottle feeding human milk may affect short- and long-term health, growth, and developmental outcomes for infants, a range of experimental and observational data is needed. More experimental data are needed that characterize the nutritive, microbial, and immunologic properties of pumped milk as fed to infants. These data must include careful consideration of mothers' practices for pumping their milk, as well as mothers' and other caregivers' practices for storing, transporting, preparing, and feeding pumped milk. For example, some mothers are feeding human milk that was pumped weeks or months earlier,9,19 but it is unknown whether pumped milk that has been stored for long periods meets the nutritional and immunological needs of older infants. Furthermore, observational data are needed that describe when, how much, and how often infants are fed pumped milk, as well as the short- and long-term health, growth, and developmental outcomes that may result.
It is striking that no data on the potential impact of pumping on the health and well-being of mothers are available to inform national recommendations. 20 Our qualitative data suggest that mothers who work outside the home do most of their pumping at work.9,10 However, mothers in the IFPS II who pumped at work did not feed human milk as long as those who fed at the breast at work. 5 It is unknown how contextual factors in the workplace affect mothers' practices for producing and providing their human milk. In turn, it is not known how mothers' experiences with pumping at work affect their well-being and performance at work. Inasmuch as the health and well-being of mothers are prioritized in public health, national recommendations and policies targeted to mothers must now be informed by an understanding of how mothers might be affected by the practice of pumping.
A Proposed Framework for Studying Pumping and Bottle Feeding Human Milk
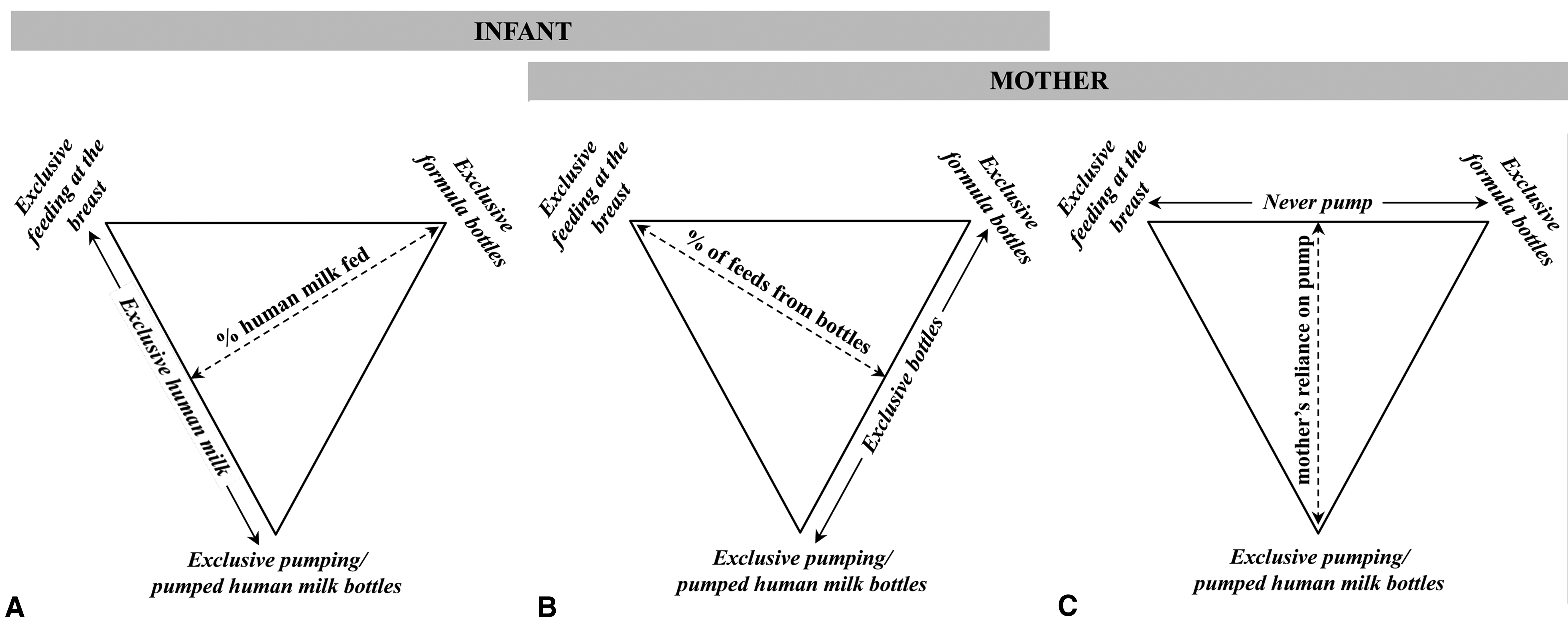
Conducting this important research will require, at a minimum, a change in how mothers and infants are described in systematic research. Infants should now be described by not only the proportion of human milk they are fed, but also how often human milk feedings come from bottles (Fig. 2A) and how often they are fed at the breast versus from bottles (Fig. 2B). Mothers must now be described by how often they remove milk from their breasts both by feeding their infants at the breast (Fig. 2B) and by pumping (Fig. 2C). This distinction is crucial because available data indicate that it can no longer be assumed that mothers start and stop producing human milk at the same time that their infants start and stop consuming it.9,19 For example, mothers might feed their infants from a frozen stock of surplus pumped milk long after they have stopped feeding at the breast.
Using the new framework to measure and study distinct practices, illustrating how the framework presented in Figure 1 may be used to study distinct practices that impact mothers, infants, or both.
Future research using terminology such as that suggested in Figure 2 could distinguish how a mother's health outcomes may relate to her practices for feeding at the breast versus her practices for pumping, or how much human milk she produced versus when she stopped producing it. Detailed data collection on pumping practices might elucidate unknown potential risks or benefits of pumping practices to mothers' health and well-being. Furthermore, future research using this suggested terminology could distinguish how infants' outcomes related to how much human milk they consume versus how much they are fed at the breast. Detailed data collection could clarify whether risks to infants' health might be attributed to formula feeding, bottle feeding, or unknown risks associated with being fed high proportions of pumped milk.
Conclusions
It has rapidly become common practice for mothers to use breast pumps to produce human milk and bottles, cups, and other caregivers to feed it to their infants. National recommendations have incorporated this shift without the support of data that describe these practices or their potential consequences for mothers and infants. Evidence is now emerging that raises both concerns and important questions that must be answered with systematic research. This research must distinguish among practices for providing and feeding human milk when categorizing mothers and their infants, including careful characterizations such as those shown in Figures 1 and 2. Given the current landscape for feeding human milk in the United States, further research in the field that does not consider and distinguish mothers' methods for providing and feeding human milk will be incomplete.
Footnotes
Disclosure Statement
No competing financial interests exist.