
Abstract
Abstract
Objective:
The purpose of this study was to determine if there is a difference in neonatal hematocrit at 24 hours of life in full-term newborns for which delayed cord clamping is performed above versus below the perineum.
Materials and Methods:
One hundred one patients with singleton pregnancies >37 weeks of gestation presenting for delivery were randomized to delayed cord clamping above or below the perineum. At 24 hours of life, neonatal hematocrit was determined, and the difference was compared using statistical analysis. Secondary outcomes measured were need for phototherapy, transfusion, and neonatal intensive care unit (NICU) admission.
Results:
Of 101 patients recruited for the study, 53 were randomized to the above group, and 48 were randomized to the below group. Twenty-seven patients in the above group and 26 patients in the below group completed the study. The above group had an average neonatal hematocrit of 52.7% (± 2.58%). The below group had an average neonatal hematocrit of 55.8% (± 2.42%). There was no statistical difference between groups (p = 0.10). Similarly, differences in secondary outcomes did not reach statistical significance. Three infants in the above group and one infant in the below group required phototherapy. None of the infants required blood transfusion. Three infants in the above group and one infant in the below group required NICU admission.
Conclusions:
When comparing delayed cord clamping above versus below the perineum, there is no difference in the neonatal hematocrit at 24 hours of life.
Introduction
S
DCC below the perineum, or pelvis, is an accepted clinical practice. It is done as a means to increase the amount of blood entering into the newborn's circulatory system. 3 Cord clamping above the perineum is also an accepted practice in uncomplicated term vaginal deliveries as it allows for immediate maternal–infant contact.
DCC has been noted to reduce the need for neonatal transfusion, especially in preterm infants. 4 In addition, the higher hemoglobin levels in newborns serve as a source of newborn iron stores to assist during the first 6 months of life.5,6 Infants born with lower iron stores may be at risk for iron deficiency during the time of exclusive breastfeeding. DCC has been shown to improve fetal hemoglobin levels around the time of birth. 7 Previous studies have typically been performed with the infant kept either at or below the level of the placenta. The concern has been that gravity plays a role in placental transfusion, and placing the newborn on the maternal abdomen can reduce or stop blood flow through the umbilical cord. 6 Potential adverse effects related to DCC include increased postpartum hemorrhage (this effect has not been supported by evidence) and increased risk of therapy for newborn jaundice (which has been noted in some studies). 8 A contemporaneous study by Vain et al. 9 was performed with neonates held on the maternal abdomen or chest and showed no difference in their primary outcome of placental transfusion.
DCC above the perineum has not been well studied in terms of its effects on neonatal hematocrit. It is therefore unclear if positioning the infant above the placenta on the maternal abdomen would have any influence on the effectiveness of the transfer of blood. If no difference in neonatal hematocrit is found, this study can be extended to those infants born via preterm spontaneous vaginal delivery to encourage skin-to-skin contact between mom and baby while waiting to clamp the cord. This contact could be beneficial to both mom and baby, as premature infants are often handed off to the awaiting neonatal intensive care unit (NICU) team for resuscitation or other necessary assessments and/or interventions, and the opportunity for that initial contact is missed.
Our hypothesis was that there would be no difference in neonatal hematocrit at 24 hours of life in healthy infants of ≥37 weeks of gestation when DCC was performed on the maternal abdomen when compared with below the perineum.
Materials and Methods
We conducted a randomized controlled trial on the labor and delivery ward of our hospital from March 2012 to October 2013. Institutional Review Board approval was obtained through the University of Texas at Houston to be conducted at Memorial Hermann Hospital. Our goal was to determine if there is a difference in neonatal hematocrit at 24 hours of life in full-term newborns for which DCC is performed above versus below the perineum. Secondary objectives were to determine need for NICU admission, blood transfusion, and phototherapy. We hypothesized that there would be no clinically significant difference in these outcomes.
Patients were consented when they presented to the hospital and the decision was made to proceed with spontaneous vaginal delivery. Inclusion criteria were females with single, intrauterine pregnancies at ≥37 weeks of gestation. Exclusion criteria were patients with acute febrile illnesses or chronic medical problems such as hypertension, diabetes mellitus, renal disease, or medically managed seizure disorders, as well as pregnancy-related complications such as pre-eclampsia, intrauterine growth restriction, chromosomal/anatomical abnormalities, and placental abruption.
Patients were randomized into one of two groups: DCC above the perineum (Group A) versus DCC below the perineum (Group B). Participants were enrolled after admission to labor and delivery by either of the Co-Investigators after determining they met appropriate inclusion/exclusion criteria and were anticipated to have a vaginal delivery. After obtaining consent, group assignment was performed by choosing above or below group assignment, which had been preselected using a random number generator maintained electronically by a single investigator. An online program called Research Randomizer was used. Participants and providers present in the delivery room were unable to be blinded due to the observable difference in infant positioning. No information regarding study group assignment was given to other providers involved in subsequent care of the mother or infant. Staff performing the newborn bloodwork was blinded to study group assignment. All data collection was performed by one of the Co-Investigators.
In those patients randomized to Group A, after delivery the infant was placed on the mother's abdomen, and the cord was clamped 60–75 seconds after delivery. In those randomized to Group B, the infant was held below the perineum, and the cord clamped and cut 60–75 seconds after delivery. The distance below the perineum was not measured during the study period. Providers were asked to keep the infant at least below the lower limits of the maternal buttocks on the delivery bed so the distance was at least 10 cm below the maternal perineum. The lower limit was not specifically stipulated but was dictated by the provider's reach and the cord length. To ensure accurate timing of cord clamping, a designated nurse served as the timekeeper, alerting the physician when 60 seconds had elapsed.
Neonatal blood was obtained at the time of routine newborn screening via heel-stick, approximately 24 hours after delivery, to check the hematocrit. The sample size was based on a previous study by Rabe et al., 3 who were also evaluating neonatal hematocrit after DCC for 30 seconds compared with repeated cord milking with the intention of detecting a 10% difference with a p value of 0.05 and a power of 80% for a two-sided t test. That study determined that 26 patients in each group were needed for a total of 52 subjects. Allowing for a dropout rate of 20%, we determined that we would need 32 patients in each group for a total of 64 patients. Due to a higher than anticipated dropout rate, our sample side was subsequently increased to 101 patients in order to achieve at least 26 dyads in each group. Student's t test for two independent samples was used to compare continuous data, and the Z test for proportions was used to compare categorical data.
Results
The study recruited 101 patients from March 2012 to October 2013. Fifty-three patients successfully completed the study: 27 in the above group and 26 in the below group. Figure 1 shows the reasons subjects were removed from the study after enrollment.
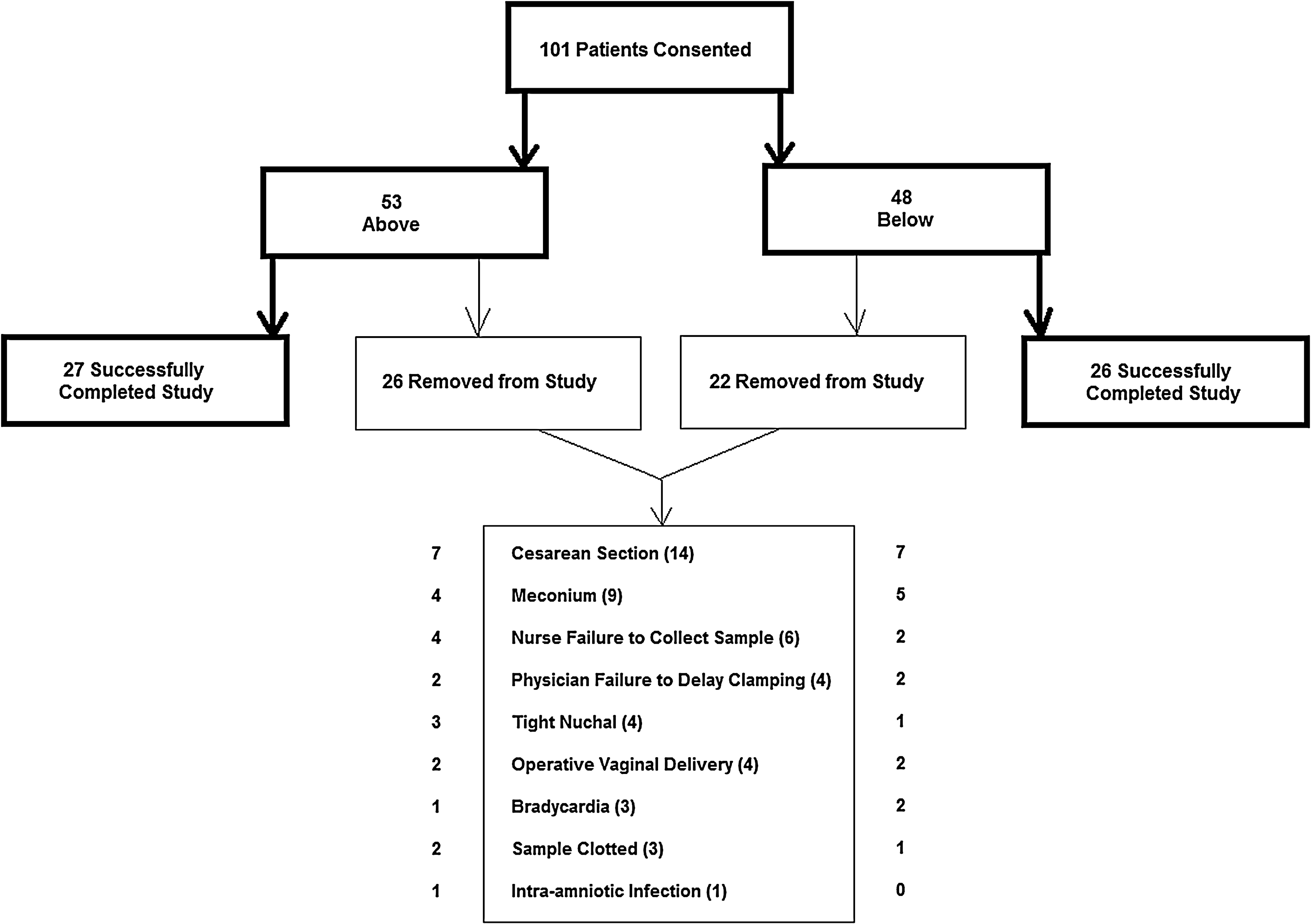
Flowchart showing group allocation and reasons for removal from the study.
Maternal demographics and infant birth data are shown in Tables 1 and 2, respectively. There were no significant differences in the maternal or neonatal characteristics. Primary outcome of neonatal hematocrit was compared using Student's t test. Neonatal hematocrit was obtained with routine newborn heel-stick approximately 24 hours after delivery. The above group had an average neonatal hematocrit of 52.7% (± 2.58%). The below group had an average neonatal hematocrit of 55.8% (± 2.42%). The difference was not statistically different between the two groups (p = 0.10).
NICU, neonatal intensive care unit.
Secondary outcomes included need for phototherapy, transfusion, and NICU admission. This information was obtained by chart review after discharge. None of these outcomes showed a statistically significant difference. Three infants in the above group and one infant in the below group required phototherapy. None of the infants, in either group, required blood transfusion. Three infants in the above group and two infants in the below group required NICU admission. Reasons for NICU admission included respiratory distress, tachypnea, hypoglycemia, poor feeding, and excessive weight loss of >10% (Table 2).
Discussion
This study shows that when comparing DCC above versus below the perineum for 60–75 seconds after vaginal delivery, there is no statistically significant difference in the neonatal hematocrit at 24 hours of life. This supports the immediate and continuous maternal–infant contact after uncomplicated vaginal birth, through the first hour of life and until after the initial breastfeeding. Despite the concern that gravity is needed to increase the transfer of blood to the newborn when delayed clamping is performed during skin-to-skin contact, this was not proven in our study. Although the specific breastfeeding initiation and continuation rates for the study cohort were not collected, the overall breastfeeding initiation rate for our institution at the time of the study (between March 2012 and October 2013) was 74.3% (ranging from a monthly rate of 67.2% to 84.4%). Our exclusive breastfeeding rates at discharge were low at an average of 27.8% with a monthly low rate of 19% and high rate of 40%. Our study cohort would not have been expected to have different initiation rates. We are unable to discuss the impact of the different DCC locations on breastfeeding continuation at the time of discharge as this was not in our study objectives. This would provide an interesting area for future research.
This study did not demonstrate a difference in our secondary outcomes, including need for phototherapy, transfusion, or NICU admission between the two groups, although our study was not powered to detect such a difference. A similar study, 7 conducted during the same time period as ours, also showed no difference in neonatal hematocrit at 36–48 hours of life when DCC was performed on the maternal abdomen or chest.
One weakness of our study is that the participating dyads and delivering physicians were not blinded. Due to the nature of the study, blinding of the patients and medical staff present at the time delivery was not possible. However, the staff collecting the newborn hemoglobin and hematocrit were blinded to group assignment. Maternal knowledge of study group allocation could not change the hematocrit value. The exact location of the placenta was not gathered in this study so the distance either above or below the perineum may not be reflective of the distance above or below the placenta, which could potentially alter study results.
Another weakness of the study is that the data on all eligible subjects were not obtained secondary to physicians forgetting to delay cord clamping, nurses forgetting to collect neonatal samples, or the samples clotting after collection. A total of 13 such events occurred in our study. It is unclear how the study data would be affected had hematocrits been obtained in these subjects.
In addition, our dropout rate was 48%, much higher than the 20% we initially predicted. Many of those dyads that were dropped from the study were subsequently ineligible for DCC above or below the perineum at our facility due to cesarean delivery (n = 14), meconium (n = 9), tight nuchal cord (n = 4), operative vaginal delivery (n = 4), and bradycardia (n = 3). As the dropout rate was similar for both groups it would not be anticipated to change the results. We had to enroll more patients than initially anticipated to meet our goal of 26 dyads in each group.
Although it appeared that doctors, nurses, patients, and families enjoyed DCC above the perineum, further studies are needed to determine patient satisfaction with DCC on maternal abdomen as this was not part of our study design. As we have demonstrated no statistical difference in hematocrit or adverse events with DCC above versus below the perineum in infants of ≥37 weeks of gestation, further randomized controlled trials are needed to determine if similar outcomes are noted in preterm infants. DCC on the maternal abdomen could be beneficial to premature infants and their mothers. These newborns are often handed off to the awaiting NICU team for resuscitation or other necessary assessments and interventions, and the opportunity for initial contact is missed.
Some strengths of our study include our enrolled population, which was predominately Medicaid with a high prevalence of maternal iron deficiency anemia. These infants born to mothers with chronic anemia are likely to contain less total body iron stores. Thus the finding of no statistically significant difference in newborn hematocrits between study groups in our population adds additional information to the body of knowledge on this topic.
In conclusion, although DCC either above or below the perineum is an acceptable practice, DCC with the infant properly stimulated, dried, and warmed on the maternal abdomen appears to be safe and has multiple additional benefits, including thermoregulatory, cardiovascular, and glucose stability for the newborn and improved attachment and breastfeeding success for the dyad.
Footnotes
Disclosure Statement
No competing financial interests exist.