
Abstract
Abstract
Introduction:
The development of the intestinal gut is largely influenced by early nutrition. Infant immunity is challenged by the exposure of the gut to foreign bodies, which mediate inflammation of the gut. This study assessed the levels of gut inflammation in relation to the percentage of breastmilk consumed/the exclusivity of breastfeeding in South African infants. This is the first study to examine markers of gut inflammation in infants in relation to exclusivity of breastfeeding measured by a gold standard method.
Methodology:
Twenty-four black South African infants were included in this study. The categorization of different degrees of exclusivity of breastfeeding was made using an objective gold standard method developed by the International Atomic Energy Agency (deuterium dilution method). Markers of gut inflammation were measured noninvasively by sampling stool from the infants averaging 6 months of age. Gut inflammation was investigated by running multiple Droplet Digital™ (Bio-Rad, Hercules, CA) polymerization chain reaction tests profiling a panel of five mRNA probes (interleukin-8 [IL-8], S100 calcium-binding protein A8 [S100A8], Toll-like receptor-4, human leukocyte antigen on chromosome 6 region 6p21.31, and defensin alpha 8). These mRNA biomarkers expressions were tested in proportion to number of glyceraldehyde 3-phosphate dehydrogenase (GAPDH) copies as GAPDH is constitutively expressed in most cells.
Results:
Two previously described robust mRNA markers of gut inflammation (S100A8 and IL-8) were found to correlate significantly to the percentage of breastmilk intake (r2 = 0.4302, p = 0.0004 and r2 = 0.3633, p = 0.002, respectively) in the range of 75–100% in 22 samples analyzed.
Conclusions:
This study using objective methodology has shown that higher percentages of breastmilk intake are associated with significantly lower levels of gut inflammation. This further supports the health benefits observed in exclusively breastfed infants.
Introduction
T
Human breastmilk has important protective benefits against bacterial infections due to its immune properties. 9 Evidence exists that growth faltering in Gambian infants was associated with impaired gut intestinal barrier function. 11 Breastfeeding induces a gut microbiota rich in bifidobacteria, which contribute to the development of the immune response and the lower incidence of diarrhea and allergy in breast-fed infants compared with formula-fed infants. 12 A recent study comparing gut microbiota in breastfed and formula-fed Korean infants showed an higher, nearing doubled, percentage increase of bifidobacteria in breastfed infants in comparison with formula-fed infants. 13 Further suggestions of underlying gut perturbations leading to diarrhea are found in a South African study in a population with similar disadvantages as ours that showed that in both human immunodeficiency virus (HIV)-exposed and HIV-unexposed infants, those infants who were exclusively breastfed had fewer, shorter episodes of diarrhea compared with those infants who were mixed fed or never breastfed. 14
Various methods are available to determine the degree of gut inflammation in adults and children. In order to measure this in infants, the only feasible method is a noninvasive method. Various noninvasive methods do exist, including, among others, measuring the ratio of lactulose:mannitol in urine samples 15 and measuring fecal calprotectin. 16
In this study we selected a sensitive methodology of extracting human mRNA from exfoliated cells shed from the gut and then a digital drop polymerization chain reaction for maximum amplification. Five inflammatory markers were then selected from a range of inflammatory biomarkers used in previous studies.17–19
Earlier studies examining the impact of exclusive breastfeeding on the gut have been hampered by the inaccuracy of the categorization of exclusive breastfeeding because this is traditionally based on maternal recall. The stable isotope technique (deuterium dilution method) recently developed under the auspices of the International Atomic Energy Agency 20 offers researchers the ability to accurately assess exclusive breastfeeding. Studies in India and Cameroon that examined exclusive breastfeeding rates using the deuterium dilution method as well as maternal recall found a large discrepancy between the two, with the maternal recall considerably over-reporting exclusive breastfeeding.21,22
This deuterium dilution method, which involves deuterium oxide administered to the mother, has made it possible to distinguish between an infant's breastmilk intake and intake from other sources such as formula, cow's milk, teas, juice, and water. This facilitates an objective determination of exclusive breastfeeding and in this study allowed us to determine different levels of percentages of breastmilk intake as proxies of different degrees of exclusivity of breastfeeding. This technique measures the volumes of breastmilk output by the mother and thus the milk intake by the infant. In this methodology the deuterated water consumed by the mother subsequently mixes with the mother's body water, and this equilibrates and is distributed uniformly in the body. 23 A breastfeeding infant then consumes the deuterated water in his or her mother's breastmilk. This technique requires saliva samples to be collected from the mother and infant before the dose is given and over a period of 14 days after the initial dose is given to the mother. The saliva is subsequently analyzed for deuterium levels, which are fitted to a model for water turnover in the mother and infant and can be used to determine what percentage of the infant's intake was breastmilk. 20
This study therefore set out to describe the influence of exclusivity of breastfeeding (objectively measured) on markers of gut inflammation measured using noninvasive methodology.
Materials and Methods
Study population
Mother–infant pairs were participants of a parent study determining breastmilk intake using the deuterium dilution method. The inclusion criteria of the parent study, which recruited 100 mother–infant pairs, required infants to be term infants from well, breastfeeding African mothers. Ethical approval was obtained from the Biomedical Research Ethics Committee, University of KwaZulu-Natal (protocol number BE211/11). Of these 100 mothers a convenience sample of the first 35 mothers and infants was recruited for co-enrollment in this substudy, during the period January–September 2013. Additional consent was obtained from the mothers to participate in the substudy, which involved collection of a stool sample from the infant between 5 and 6 months of age.
The study was conducted in a primary healthcare center approximately 10 km from the Durban city center in South Africa. This center serves the community of Cato Manor, which has an estimated population of about 93,000 people, many of whom are unemployed and reside in informal dwellings. 24 This typical urban disadvantaged community was used for the study as it represented infants who are at risk because of poor sanitation and water supply as well as inadequate nutrition and therefore a critical population in whom determining the influence of breastfeeding is important.
Sample collection
Stool samples were collected fresh from plastic-lined diapers and transferred to 2-mL BD (Franklin Lakes, NJ) cryovials using disposable wooden sticks. Samples were frozen within 6–8 hours of collection and stored at −80°C until analysis. Stool samples were shipped and processed using methodology described by Agapova et al. 17 by the laboratory of one of the co-authors (M.M.) at the University of Washington (St. Louis, MO).
Saliva was collected using cotton wool swabs. The swabs were placed into a syringe and drained into test tubes. The samples were collected before consumption of deuterated water and after consumption over a period of 14 days for mother and child. 20
Biomarker analysis
Frozen stool (pea-sized) (200 mg) was transferred to a 2-mL tube containing seven to 10 2.3-mm-diameter zirconium/silica beads (Research Products International Corp., Mt. Prospect, IL) over dry ice. Easy NucliSENS® MAGlysis buffer (bioMérieux, Boxtel, The Netherlands) (1 mL) was added, and the mixture was “bead-beated” with a FastPrep-24 tissue homogenizer (MP Biomedicals, Santa Ana, CA) for two consecutive 45-second runs and then centrifuged (at 13,200 rpm for 10 minutes). Supernatant (200 μL) was used for automated RNA isolation by the NucliSENS easyMag® extraction instrument (bioMérieux) following the manufacturer's instructions. Samples were quantified on a NanoDrop™ (Thermo Fisher Scientific, Waltham, MA) to confirm presence and concentration of the total RNA.
Droplet Digital™ polymerization chain reaction (ddPCR™), a highly sensitive methodology, was performed using the QX100™ Droplet Digital system (Bio-Rad, Hercules, CA), which accurately provides the absolute quantification of the target sequences. The following biomarkers were selected for analysis: interleukin 8 (IL-8), S100 calcium-binding protein A8 (S100A8), Toll-like receptor-4 (TLR-4), human leukocyte antigen on chromosome 6 region 6p21.31 (HLA-DR), and defensin alpha 8 (DEFA5). These markers were selected based on literature searches and evidence gained from prior studies performed at the laboratory of co-author M.M. Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was selected as a standardized measure of the total human mRNA in the samples. 25
Reaction mixtures of 20 μL were prepared using 6 μL of RNA (20 ng/μL or less), 10 μL of ddPCR Supermix for Probes (Bio-Rad), 0.08 μL of SuperScript® III reverse transcriptase (200 U/μL; Invitrogen™, Thermo Fisher Scientific), 0.16 μL of RNaseOUT™ (40 U/μL; Invitrogen), 1 μL of 20× TaqMan® gene expression assay (Applied Biosystems, Inc., Thermo Fisher Scientific), and 2.76 (simplex) or 1.76 (duplex) μL of RNase-free water. Taqman probes were labeled with either VIC™, a proprietary green fluorescent dye (Life Technologies, Grand Island, NY) or FAM (6-carboxyfluorescein). All samples were tested in duplicate. Droplets were generated according to the manufacturer's guidelines with the QX100 Droplet Digital generator before cycling in a C1000 Touch™ thermal cycler (Bio-Rad) at 50°C (30 minutes), 95°C (10 minutes), 40 cycles of 94°C (30 seconds) followed by 60°C (1 minute), and 98°C (10 minutes). Plates were held at 4°C between amplification and droplet reading.
The data from the QX100 Droplet Digital reader was analyzed with QuantaSoft (Kosice, Slovakia) software. Fluorescent droplets were deemed positive by manually set thresholds based on results from negative control wells containing RNase-free water instead of RNA and were standardized for each assay run.
The mRNA expression for each biomarker was standardized against GAPDH concentrations. GAPDH is used in many experimental investigations as the GAPDH gene is often stable and constitutively expressed at high levels in most tissues and cells. Comparisons between mRNA from infants who were exclusively breastfeeding and mixed feeding were made using breastmilk intake values. Pearson's correlation coefficients and t tests were performed using Microsoft (Redmond, Wa) Excel™ and OpenEpi (www.openepi.com) software.
Results
All infants were born at full term. Normal vaginal delivery was the main mode of delivery. Infants' birth weights ranged from 2.5 to 4.5 kg. Half the cohort of infants were born to HIV-infected mothers who as per standard South African Ministry of Health guidelines were all receiving antiretroviral therapy, whereas the remaining infants were unexposed. CD4 counts in the HIV-infected mothers ranged from 150 to 760 cells/cm3 of blood. Exposed infants received nevirapine for their first 6 weeks of life. As per South African guidelines, all HIV-exposed infants are tested by DNA-polymerase chain reaction for HIV infection; none of the HIV-exposed infants was infected.
Breastmilk intake percentages ranged from 75% to 100%, with the intake being a percentage of the total dietary intake.
Of the 35 infants enrolled in the study, 11 infants were not included in this study because of incomplete data: six were missing breastmilk intake values, and five had incomplete biomarker data. The 11 infants not included in the study did not differ in any of the variables examined when compared with the 24 included in the study.
Of the five biomarkers analyzed only two (S100A8 and IL-8) were robustly expressed on all 24 samples with readable GAPDH values. Two infants had values that were significant outliers (more than 4 standard deviations from the mean), and therefore the biomarker results for these two infants were removed in all the analyses. Plotting of S100A8/GAPDH and IL-8/GAPDH with breastmilk intake values revealed significant negative correlations: r2 = 0.4302, p = 0.0004 and r2 = 0.363, p = 0.002, respectively (Fig. 1). HLA-DRA and TLR-4 (data not shown) were only detected in 15 samples but showed similar significant negative correlations with breastmilk intake percentage: HLA-DRA, r2 = 0.201, p = 0.03; TLR-4, r2 = 0.300, p = 0.003. The fifth biomarker (DEFA5) was not adequately detected in relation to GAPDH levels in any of the 24 samples.
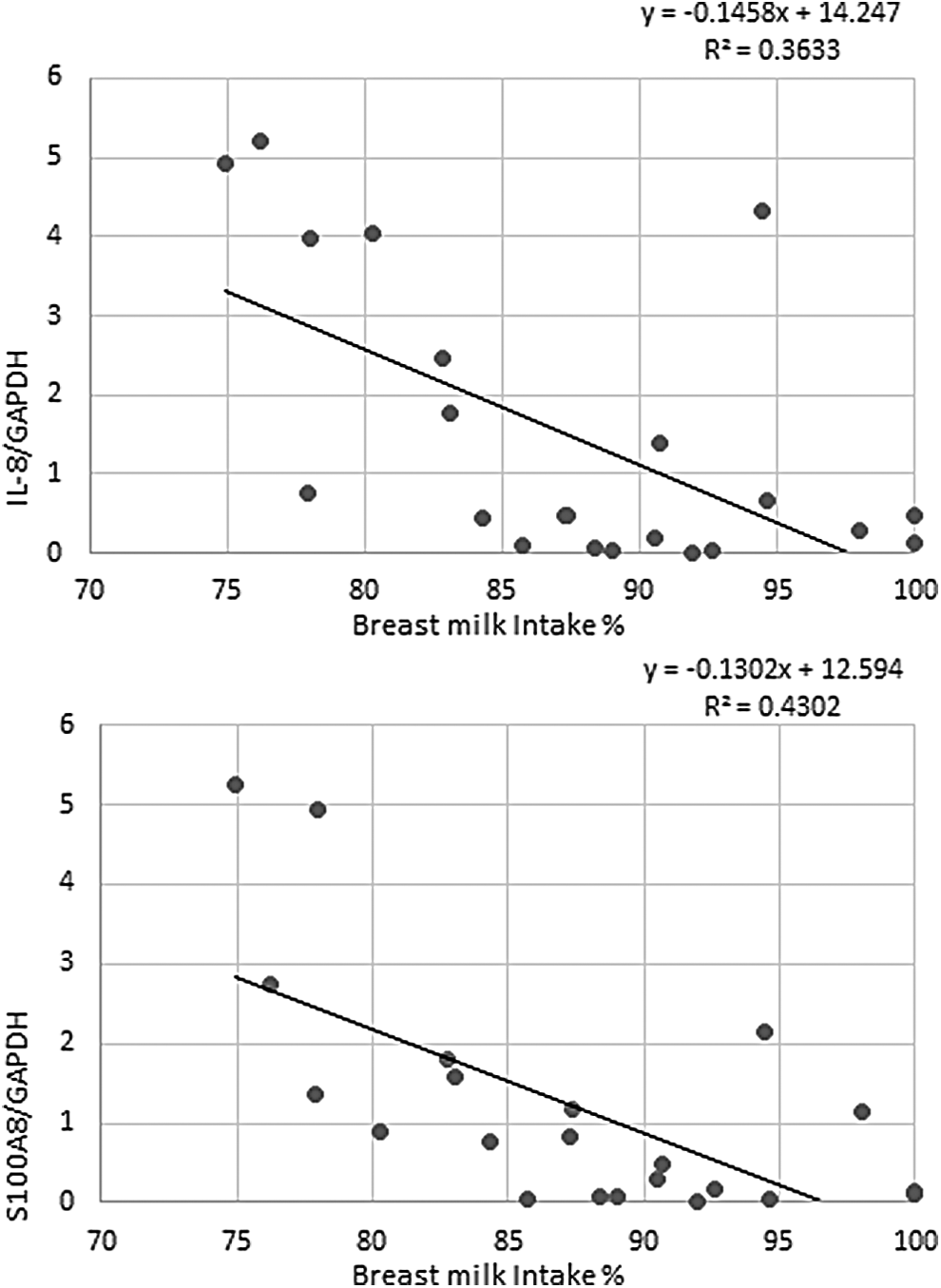
Target/glyceraldehyde 3-phosphate dehydrogenase (GAPDH) expression in relation to percentage breastmilk intake. The mRNA markers
To further test the association of breastmilk intake percentages with the two biomarkers, S100A8 and IL8, breastmilk intake percentages were divided into two groups: the top 11 values and the lower 11 values (i.e., ≥88% and <88%). Means of the S100A8 (0.42 ± 0.66 and 1.94 ± 1.70, respectively) and IL-8 (0.70 ± 1.27 and 2.24 ± 1.97, respectively) markers were then compared with these percentage breastmilk intake categories using a two-sample independent t test and gave significant p values at the 95% confidence level (p = 0.0161 and p = 0.0415, respectively).
These biomarkers showed no correlation with all other variables collected: hygiene, HIV exposure, delivery mode, age, gender, and birth weight.
Discussion
Our examination of markers of gut inflammation showed minimal to no inflammation in the infants who had high levels of percentage of breastmilk intake, and a dose–response was seen with slightly higher levels of inflammation, the lesser the percentage of breastmilk intake. Our results confirm the findings of previous studies. Decreased inflammation has been previously found in infants who are exclusively breastfed compared with mixed fed at 3 months of age. 26 Exclusive breastfeeding has previously been associated with less low-grade inflammation, as estimated by serum fibrinogen levels in healthy children and adolescents reported to be exclusively breastfed. 27
The most important strength of this study is that we accurately differentiated different degrees of exclusivity of breastfeeding/levels of percentage of breastmilk intake using the gold-standard deuterium dilution method. Another strength of our study was that we successfully extracted human DNA/RNA using a noninvasive method of stool sampling in infants as young as 6 months of age. Furthermore, markers of gut inflammation were successfully expressed using stool samples. The success of this methodology was further verified using GAPDH as a means of normalization for interspecimen differences in concentration of human mRNA. There are very few studies that have successfully validated noninvasive mRNA technology. We were, moreover, able to validate this methodology in infants.
The observation made in this study that the lower the percentage of breastmilk intake, the greater the risk of gut inflammation is important as it provides further mechanistic evidence to suggest why exclusive breastfeeding results in fewer infections and less perturbations of immunity. It provides additional information for policy makers to advocate for the promotion of exclusive breastfeeding.
A limitation of this study is that although we had longitudinal data on other factors that could influence the gut, such as antibiotic exposure, significant diarrhea episodes, etc., because of the small sample size we obviously could not control for these other variables. Nevertheless, the results indicate that the exclusivity of breastfeeding remains a strong influence regardless of intervening events that could have affected the gut milieu. An additional limitation is that there was a small variation in breastfeeding practices, which limited the ability to show an association over a wide range. We recommend that follow-up studies should include children who also receive no breastmilk or minimal breastmilk to provide a better understanding of the influence of exclusivity of breastfeeding on gut inflammation biomarkers.
Conclusions
This study using objective methodology has shown that higher percentages of breastmilk intake are associated with significantly lower levels of gut inflammation as detected by biomarkers. These results therefore provide further mechanistic support for the health benefits observed in exclusively breastfed infants.
Footnotes
Acknowledgments
The authors wish to acknowledge the staff based at Cato Manor Clinic. We wish to extend gratitude to the study staff Gcinile Maphanga, Zanele Msomi, Isabel Ordiz, and Charlene Baxendale for their invaluable support. The authors extend further acknowledgement to the patients who participated in this study; without their dedication this study would not have been feasible. The study was funded by the University of KwaZulu-Natal Post-Doctoral Scholarship Programme, the Mark Manary laboratory, and the International Atomic Energy Agency.
Disclosure Statement
No competing financial interests exist.