
Abstract
Abstract
Background:
Breastfeeding is recommended by international bodies as the only source of infant nutrition during the first 6 months of life. Sometimes infants prefer to nurse on one breast for no obvious reason (hereafter called infant's unexplained breast preference [IUBP]). IUBP might reduce the rate of exclusive breastfeeding. The prevalence of IUBP is unknown because most of the literature on IUBP so far has been anecdotal. This study's objective was to investigate the prevalence and characteristics of IUBP among healthy infants in Al-Ahsa, Saudi Arabia.
Materials and Methods:
We conducted a population-based, cross-sectional study between March and August 2013 in the Al-Ahsa area, Eastern Province, Saudi Arabia. Healthy infants who had been born at full term (≥37 weeks of gestation) and were 2–24 months of age were included. We distributed 600 self-administered surveys to mothers who attended vaccination clinics in nine primary healthcare centers.
Results:
Of 478 mothers who responded to the survey, 121 (25.3%) reported unilateral breastfeeding. IUBP was the most common reason for unilateral breastfeeding, with a prevalence of 13.6% (65/478). IUBP developed at a median age of 1 month (range, 1 day–9 months) and was familial in 42.9% of cases. It was the only reason for formula feeding during the first 6 months of life in 18.5% of cases.
Conclusions:
IUBP is common, develops very early in life, and can be familial and a reason for formula feeding. However, these findings need to be confirmed in other studies of other populations.
Background
B
One of these problems is unilateral breastfeeding, in which one breast is less used than the other breast or not used at all for breastfeeding.2–7 Unilateral breastfeeding can have cultural reasons or be due to clinical causes such as a small or inverted nipple on one side, reduced milk flow from the nonpreferred breast, or infants being held in a painful position.2–8 Sometimes infants simply prefer to nurse on one breast for no obvious reason.2–6 Babies of several nonhuman primate species have similarly been observed to prefer nursing one breast.9–14 Henceforth in this article, this phenomenon is referred to as infant's unexplained breast preference (IUBP). There is evidence that IUBP can reduce the rate of exclusive breastfeeding2,4–6; however, the prevalence of IUBP in humans is unknown because most of the literature on IUBP so far has been anecdotal, with the exception of two studies.2,3
The first of these studies was conducted by Stables and Hewitt 2 in a hospital in London, United Kingdom in 1995. The researchers studied three human behaviors that could explain the development of an unexplained unilateral breastfeeding problem or preference occurring at the first breastfeeding among mothers who never had practiced breastedfeeding previously. These three human behaviors were infants' innate head-turning preference, mothers' preference to hold their infants on one side over the other, and mothers' handedness. The study included only healthy mothers without any breast problems whose infants were healthy, weighed ≥2.5 kg at birth, and were ≤72 hours of age. The three behaviors were analyzed in 32 mother–infant pairs for whom an unexplained unilateral breastfeeding problem/preference was reported and 28 mother–infant pairs for whom bilateral breastfeeding was reported. The researchers showed that unilateral breastfeeding was associated with infants' innate head-turning preference and that a mother's preferred holding side was opposite that of her dominant hand. It is difficult to ascertain whether this association is dependent or independent because right-handedness was more common and infants preferred to turn their heads to the right side.
The second study was conducted by Baslaim et al. 3 in Jeddah, Western Province, Saudi Arabia. The investigators conducted a retrospective analysis of data from 75 mothers who visited their surgical breast clinic over a period of 12 years (1998–2010). They found that the most common cause of unilateral breastfeeding was surgical/medical breast disease (37%) and the least common cause was IUBP (12%). Because the women were at a surgical breast clinic, this population might have had a much higherr incidence of breast problems than the population as a whole, so the prevalence of breast disease as a cause of unilateral breastfeeding might not be representative of a wider population. As these two studies were small and hospital based, we aimed to investigate the prevalence and characteristics of IUBP in a fairly large, population-based study.
Materials and Methods
Study design and data collection
This population-based cross-sectional study was conducted between March and August 2013 in the Al-Ahsa area, Eastern Province, Saudi Arabia. Saudi healthy infants who had been born at full-term (≥37 weeks of gestation) and were 2–24 months of age at the time of recruitment were included. The study involved a self-administered survey. One of the investigators (S.Y.A.), a certified breastfeeding counselor, developed an original survey in the Arabic language. Two other investigators (M.A.A. and A.M.O.), who are certified breastfeeding counselors and trainers, revised the survey.
A pilot survey was conducted with 20 mothers to obtain their opinions on the wording, clarity, and suitability of the survey, as well as the time required to complete it. These mothers reported that the survey required 5–8 minutes to complete and needed minor modifications. The final script was adjusted accordingly.
The final survey had three parts: (1) demographic questions; (2) a “yes/no” question regarding the occurrence of infant preferring nursing one breast; and (3) if the response to the previous question was “yes,” mothers were prompted to provide detailed information regarding IUBP. Mothers were asked to disclose their age, the age of their infants, and the name or description of any disease(s) that their infants might have. Some questions permitted only a single answer; others asked the mothers to check all that applied, including an “Other (Please Specify)” option. An English translation of the final survey is shown in the Appendix.
Collection of 500 completed surveys was thought to be achievable in a 6-month period. Vaccination clinics are available at 61 urban and rural locations in the Al-Ahsa area, and each vaccination clinic serves a specific catchment area. We distributed 600 self-reporting surveys to mothers who attended vaccination clinics in the nine primary healthcare centers whose staff offered their help. Thus, the sample selection was nonrandom. Mothers gave verbal consent, and data were obtained anonymously with no infants or mothers identifying information.
Statistical analysis
The responses of the 20 pilot survey mothers were excluded from the final analysis, as were surveys with unanswered “yes/no” question about infant's breast preference. We also excluded surveys with unanswered question about pregnancy duration in order to ensure that we included only infants born at ≥37 weeks of gestation. Unanswered questions were excluded from the denominators when calculating percentages. A chi-squared goodness of fit test was performed to test the deviation of the observed proportions of reasons for unilateral breastfeeding from that reported by Baslaim et al. 3 The same test was also conducted to determine the deviation of the observed percentages of left and right breast preference from the expected equal proportions. A chi-squared test of independence was used to make comparisons between the characteristics of IUBP cases and those of bilateral breastfeeding cases. A two-sided p value of <0.05 was considered statistically significant. Bootstrapping based on 1,000 bootstrap samples was used to calculate the 95% confidence interval (CI) for percentages and medians. Analysis was performed using Statistical Package for Social Sciences software (SPSS version 20; IBM, Armonk, NY).
Results
The survey response rate was 79.7% (478/600), as 45 mothers refused to participate, and 77 surveys were excluded for the following reasons: unanswered “yes/no” question about infant's breast preference (n = 10), no response regarding length of pregnancy (n = 35), infants born at <37 weeks of gestation (n = 30), or infants with major diseases (n = 2).
Of the 478 mothers whose answers were used in the analysis, 121 (25.3% [95% CI, 21.5–29.1%]) reported unilateral breastfeeding. Table 1 lists the self-reported reasons for unilateral breastfeeding and their prevalence. The most frequent cause of unilateral breastfeeding was IUBP (n = 65; 13.6% [95% CI, 10.5–16.9%]). Table 1 shows that the proportions of the reasons we found for unilateral breastfeeding deviated significantly from those reported by Baslaim et al. 3 (chi-squared goodness of fit, p < 0.001); in particular, Baslaim et al. 3 found a higher prevalence of breast disease as a cause of unilateral breastfeeding (37% versus 7% in our study).
Table 2 lists the characteristics that were reported in IUBP cases. Of the 65 mothers who reported IUBP, 26 (40.0%) said that they were worried about it, but only eight of them sought medical advice. The type of advice received was as follows: reassurance that IUBP was not a problem (n = 4), encouraged to feed more from the nonpreferred breast than they did (n = 3), and advice to express milk from the nonpreferred breast (n = 1).
Chi-squared goodness of fit p = 0.17.
IUBP, infant's unexplained breast preference.
Figure 1 depicts distribution of infants' age when IUBP started. The IUBP developed at a median age of 1 month (range, 1 day–9 months). The left breast was preferred by 58.5%, and the right breast was preferred by 41.5% of infants who showed IUBP (p = 0.17). Forty infants (61.5% [95% CI, 50.0–73.2%]) received mixed breastfeeding (i.e., breastmilk and formula milk) in the first 6 months after birth. Of these, mothers of 12 infants (30% [95% CI, 16.7–45.2%]) stated that they started mixed feeding only because of IUBP. The characteristics of IUBP cases and bilateral breastfeeding cases did not differ significantly (Table 3).
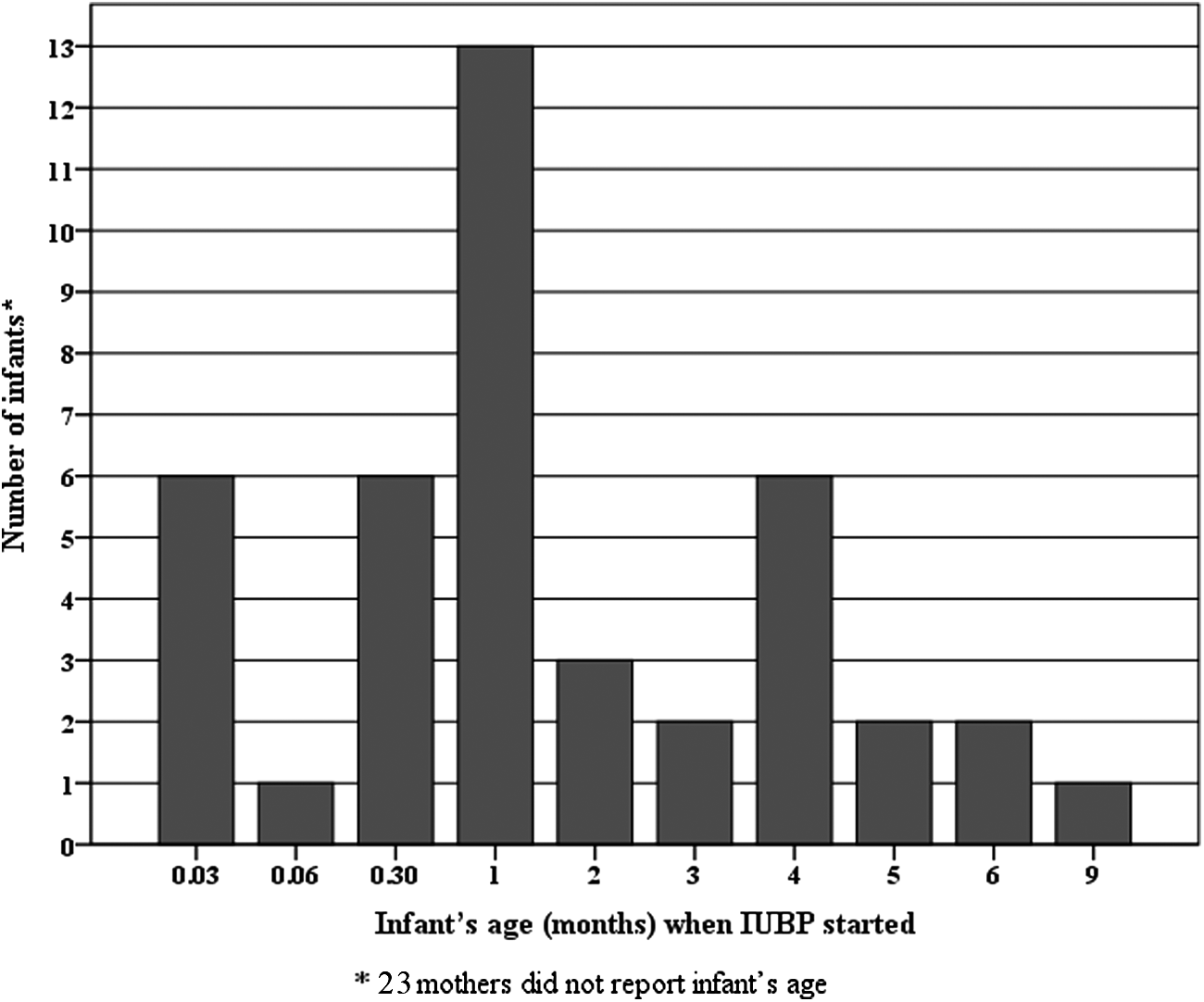
Distribution of infants' age when infant's unexplained breast preference (IUBP) started. *Twenty-three mothers did not report the infant's age.
IUBP, infant's unexplained breast pain.
Discussion
One-quarter of lactating mothers in our study population experienced unilateral breastfeeding. IUBP was the most common reason for unilateral breastfeeding in healthy Saudi full-term infants. It was found to develop in very early life, to sometimes be familial (42.9% of the cases), and to increase the likelihood of mixed breastfeeding.
Our finding that IUBP is the most common reason for unilateral breastfeeding contradicts the finding of Baslaim et al., 3 who determined that surgical breast disease was the most common cause. The conclusions probably differ because our study was population based, whereas the previous study 3 was hospital based. It would be expected that a surgical breast clinic would find surgical/medical causes to be the most common explanation for unilateral breastfeeding. We believe that our conclusions regarding the reasons for unilateral breastfeeding are more representative of the general population because our study had less selection bias.
The left breast was preferred by 58.5% and the right breast by 41.5% of infants who showed IUBP. This difference did not reach statistical significance (p = 0.17) because of the small number of IUBP cases (n = 65). A total number of 270 IUBP cases would be required in order to test whether this difference is statistically significant at two-sided alpha = 0.05 and power = 80%. Animal studies have also shown a predominance of left breast preference.9–14 However, Baslaim et al 3 found that the right breast was more often preferred (by 20% of their population). This finding could be due to the selection bias introduced by using a sample of mothers who visited a surgical breast clinic and therefore were likely to have advanced breast disease. Previous work has shown that the left breast is more affected by diseases than the right breast. 15
As in the 1995 study by Stables and Hewitt, 2 we found that IUBP can develop in very early life. The 1995 study found that IUBP is statistically more prevalent among primiparous than multiparous mothers who had never practiced breastfeeding previously. 2 The present study showed that there was only a nonsignificant trend for primiparous mothers to report IUBP more than multiparous mothers. This trend could be due to primiparous mothers being perhaps more anxious and therefore more likely to report IUBP or to multiparous mothers being perhaps more skillful in dealing with IUBP. Nevertheless, this finding should be investigated in future studies to try to identify the reasons for this difference. As in the 1995 study, 2 we found no association between IUBP and the sex of the infant or employment status of the mother. However, it should be noted that methods of the 1995 study 2 and the present study were different. The 1995 study asked about the first breastfeeding only among the infants at ≤72 hours of life, 2 whereas the present study asked about breastfeeding history among infants aged 2–24 months.
Unilateral breastfeeding may be associated with morbidities in both mothers and children.1,3,6–8 One reason for this association is that unilateral breastfeeding may reduce the rate of exclusive breastfeeding. The IUBP was the only reason for formula feeding during the first 6 months of life in 18.5% of cases. The IUBP may create a vicious cycle of reduced milk production. The nonpreferred breast will not be emptied. This increases the level of inhibitor of lactation hormone, which will inhabit milk production in the nonpreferred breast. 4 Reduced milk production will boost the unilateral breastfeeding. Additionally, the nonpreferred breast in mothers who feed unilaterally has been shown to be at greater risk for development of various breast diseases, including breast cancer.3,8 Therefore, there is a need to reduce the rate of unilateral breastfeeding, and mothers should be encouraged to seek lactation support/advice to help resolve this problem.
Several interventions have been proposed for overcoming the problem of IUBP, including expressing milk from the nonpreferred breast or using a “football hold” on the side of the nonpreferred breast.2,4,6 In a “football hold” the mother places her infant under her arm on the same side that the infant is nursing from (e.g., to nurse from the left breast, the infant is held under the left arm). It should be noted that none of these interventions has been evaluated in a clinical trial. In addition, the 1995 study showed that the football-holding position is not effective in achieving successful continuation of breastfeeding until an infant is 6 weeks old. 2 This might be the reason why no mothers in the present study who sought medical advice were advised to use the football-holding position. We agree with Stables and Hewitt 2 that there is a need for further research to determine the most effective intervention to address IUBP.
Investigating the biological explanations for IUBP was not within the scope of the present study. Three behaviors can be proposed as explanations for IUBP. The first is that approximately 90% of supine full-term infants like to turn their heads to the right, as they usually would when feeding from the left breast.16–19 The second is that more mothers tend to hold their infants on the left than on the right.16,20–22 The third behavior is mothers' handedness. These three behaviors were evaluated by Stables and Hewitt. 2 These researchers showed that unilateral breastfeeding was associated with infants' innate head-turning preference and that a mother's preferred holding side was opposite to that of her dominant hand. 2 Whether these findings are dependent on each other or independent is difficult to ascertain because right-handedness was more common among mothers than left-handedness, and infants preferred to turn their heads to the right side. 2 Moreover, these behaviors cannot account for all cases of IUBP because they are much more prevalent than IUBP, and not every infant in any given family showed IUBP. The IUBP may be innate; however, additional biological explanation(s) for IUBP need to be determined.
The present study has several limitations. First, it involved nonrandom probability sample selection, which might affect its generalizability. 23 Second, it has a potential for recall bias (differences in the accuracy of completeness of mothers' recollections of breastfeeding and associated factors) because it is a cross-sectional, self-reported study. 24 Third, a subtle torticollis, tight jaw, an early ear infection, or other historic, anatomic, or physiologic issues might have been overlooked because of the recall bias, and only eight (12.3%) of mothers consulted a health professional about IUBP. On the other hand, prevalence of IUBP might have been underestimated, as the study included infants less than 6 months old who might develop IUBP later in life. This would also affect calculation of median age of development of IUBP. Fourth, the small number of cases of IUBP precluded robust analysis of the data. Future studies should be large enough to include greater numbers of IUBP cases, which would allow them to identify statistically significant differences. Fifth, the study did not measure extent of breast preference. Sixth, language of the survey might influence the mothers' response. The mothers might respond differently if the word “refusing one breast” had been used instead of “preferring one breast,” which needs to be addressed in future study. However, Stables and Hewitt 2 have suggested asking the mothers about the preferred breast rather than the refused breast based on their finding that mothers with unilateral breastfeeding problem were more likely to report the preferred breast.
In conclusion, the present study is the first fairly large, population-based study of IUBP. We identified the prevalence and some characteristics of IUBP; these data could be utilized by breastfeeding support programs and for calculating sample sizes for future studies of IUBP. The results showed that IUBP is the most common reason for unilateral breastfeeding, with a prevalence of 13.6% in our study population. They also showed that IUBP can be familial, is more common for the left breast than for the right, develops in very early life, and reduces the rate of exclusive breastfeeding. However, these characteristics need to be confirmed in longitudinal observational studies and in a variety of populations.
Footnotes
Acknowledgments
We thank the mothers who participated. This study would not have been possible without the help of the staff of vaccination clinics in the following primary healthcare centers: Al-Battaliyah, BaniMa'an, Al-Jafr, Al-Omran, Al-Mansorah, Al-Shu'bah, Al- Rashidiya, Al-Salhiyah, and Almana General Hospital. The language editing of this manuscript by Macmillan Science Communication was financed by King Abdullah International Medical Research Center.
Disclosure Statement
No competing financial interests exist.