
Abstract
Abstract
Studies were examined to evaluate the impact of the Baby-Friendly Hospital Initiative (BFHI) on breastfeeding and early infant health outcomes in U.S. populations. Using the Social Ecological Model as a guiding theoretical framework, results were categorized into four interrelated multilevel factors: (1) maternal/infant dyad factors, (2) provider factors, (3) hospital organizational factors, and (4) policy/systems factors. Results from the review support the BFHI's success in facilitating successful breastfeeding initiation and exclusivity. Breastfeeding duration also appears to increase when mothers have increased exposure to Baby-Friendly practices, but deficiencies in breastfeeding tracking mechanisms have limited reliable breastfeeding duration data. Of the 10 steps of the BFHI, step 3, prenatal education and step 10, postnatal breastfeeding support are the most difficult steps to implement; however, those steps have the potential to significantly impact maternal breastfeeding decisions. The underlying mechanisms by which Baby-Friendly practices contribute to maternal breastfeeding decisions remain unclear; thus, studies are needed to examine mothers' experiences and perceptions of Baby-Friendly practices. Additionally, studies are needed to investigate the impact of the BFHI for women living in rural areas and in southeastern regions of the United States. Finally, studies are needed to examine early infant health outcomes related to the BFHI, especially for late premature infants (34–36 weeks) who are most vulnerable to poor outcomes and are in need of specialized breastfeeding support. Results from future qualitative and quantitative explorations could clarify how the delivery of Baby-Friendly practices leads to successful breastfeeding and infant health outcomes.
Background
E
Rates of breastfeeding in the United States are generally problematic, falling below Healthy People 2020 national breastfeeding goals for infants ever breastfed (goal = 81.9%, actual = 79.2%), infants breastfed at 6 months (goal = 60.6%, actual = 49.4%), infants breastfed at 12 months (goal = 34.1%, actual = 26.7%), and infants exclusively breastfed at 6 months (goal = 25.5%, actual 18.8%).3–5,8,9 In 2001, the World Health Organization (WHO) and the United Children's Fund (UNICEF) launched the Baby-Friendly Hospital Initiative (BFHI) to establish supportive environments and educational services that enhance initial breastfeeding experiences for mothers and infants.3,10,11 The overarching goal of the BFHI is to improve breastfeeding outcomes, including increased rates of breastfeeding initiation, breastfeeding exclusivity, and longer breastfeeding durations.12–14 Hospitals and birthing centers gain Baby-Friendly designation status by demonstrating implementation of the Ten Steps to Successful Breastfeeding (Appendix A) and compliance with the WHO's International Code of Marketing for Breast Milk Substitutes.11,16 The “Ten Steps” include 10 maternal support and breastfeeding promotion practices, and “The Code” includes limiting the advocacy and marketing of formula to new mothers, along with paying a fair market price for formula within the facility.13,14,16
Baby-Friendly practices are based on the premise that individual attitudes toward breastfeeding are largely influenced by breastfeeding education during the early prenatal period, positive birth and initial breastfeeding experiences, and continued provider support.5,10,17 Internationally, in countries such as Scotland, Belarus, Switzerland, and Brazil, evidence suggests that Baby-Friendly practices positively influence breastfeeding rates on a local or national level.18–23 However, documentation is fragmentary regarding the impact of the BFHI on early infant health outcomes and breastfeeding outcomes in the United States.1,24–27 While studies suggest that Baby-Friendly practices increase breastfeeding initiation and exclusivity rates, there is a lack of reconciliation on breastfeeding duration rates and causal mechanisms related to the BFHI's success.22,26,27 Additionally, evidenced-based guidelines for early infant health outcomes such as neonatal weight loss, hypoglycemia, hyperbilirubinemia, and hypothermia with respect to Baby-Friendly practices are inadequate.24,28,29 This is especially pertinent for late preterm infants (34–36 weeks) who are vulnerable to dehydration and rehospitalization due to feeding difficulties related to prematurity. Furthermore, no reviews of early infant health outcomes and breastfeeding outcomes related to Baby-Friendly practices in U.S. settings were located through literature searches of five academic research databases. The purpose of this integrative review is to examine updated evidence for the impact of the BFHI in the United States on early infant health outcomes and breastfeeding outcomes to determine strengths and limitations of the initiative, along with gaps in service for U.S. mothers and infants. The results of the review will inform future breastfeeding promotion interventions tailored to reduce breastfeeding-related health disparities in the United States.
Social Ecological Model
The BFHI has no underlying theory guiding its design; however, the Social Ecological Model (SEM) is an appropriate theoretical framework to explain how Baby-Friendly practices influence breastfeeding outcomes on multiple levels. The SEM guides health promotion interventions through a theoretical understanding of the relationship of multiple factors at the intrapersonal, interpersonal, organizational, and policy levels and their influence on health and health behavior.30,31 Examination of the interaction of multiple factors within the social environment, beyond the influence of a single level factor, provides deeper understanding of a phenomenon and offers insights to create effective and innovative solutions. 32
Baby-Friendly practices include multidimensional and multilevel factors that affect mothers' social and environmental experiences.31–33 As illustrated in Figure 1, application of the SEM to the BFHI explains how breastfeeding outcomes are influenced by factors on the patient (mother/infant dyad), provider, organizational, and systems levels.31,32 Intrapersonal maternal/infant dyad factors are the base of the model and include factors affecting mothers' attitudes, knowledge, beliefs, experiences, and perceptions of breastfeeding. These factors directly influence mothers' breastfeeding self-efficacy and motivation to breastfeed, and thus, affect breastfeeding and early infant health outcomes.5,34,35 Interpersonal provider factors mediate maternal attitudes and breastfeeding motivation and include social and educational support delivered by health providers.34,35 Staff education and training, as well as adequate time and staffing resources to properly implement the “Ten Steps” are interpersonal provider level considerations.26,30,36 Organizational hospital factors involve establishing a written hospital policy to support breastfeeding mothers, consistent organizational implementation of the “Ten Steps,” and provision of structural, social, and health provider support throughout all stages of pregnancy.26,30,36,37 Finally, policy/systems factors include the availability of breastfeeding information, and standardized breastfeeding definitions, charting, and tracking mechanisms.26,27,30,37,38
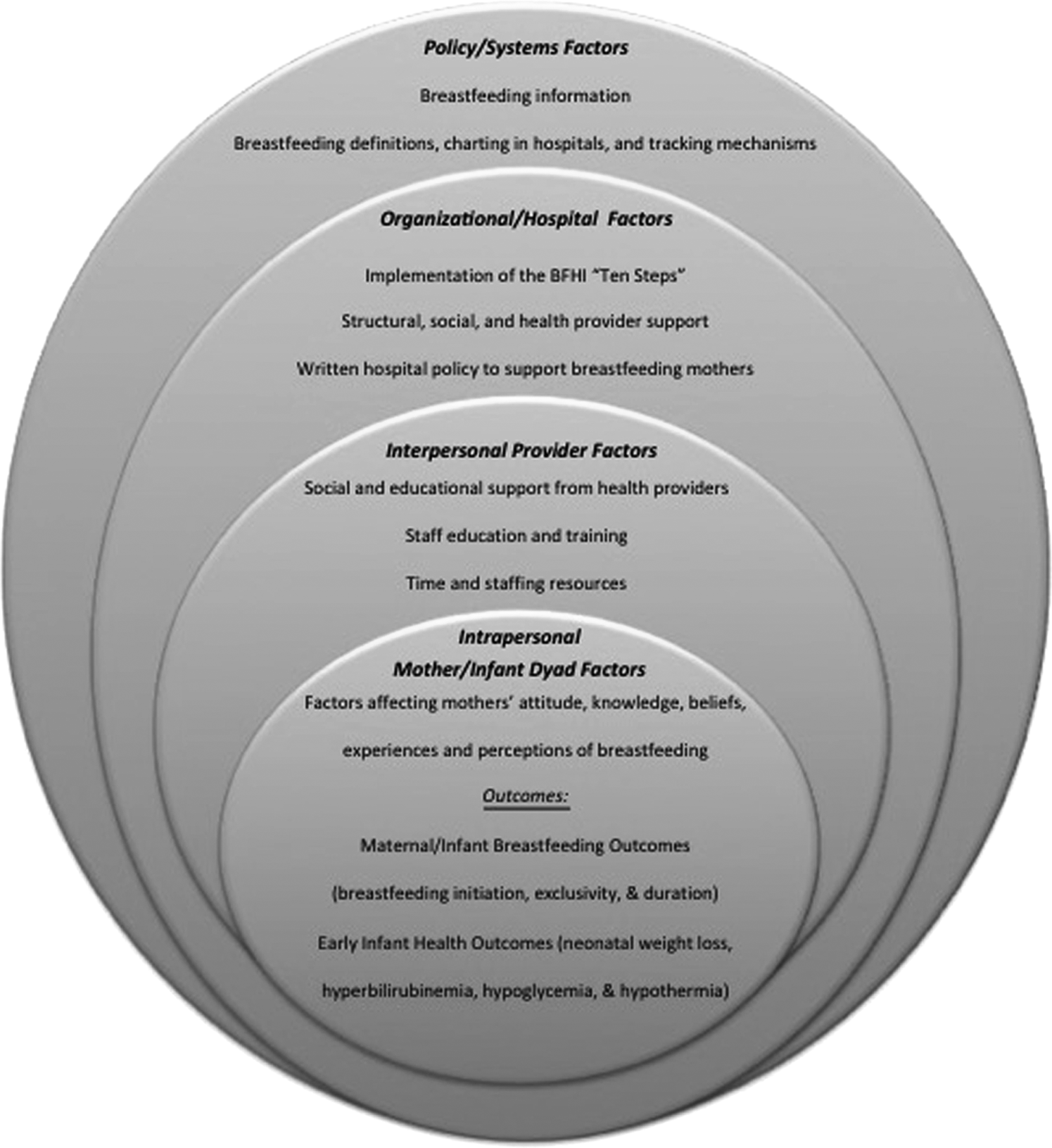
Conceptual model of an application of the Social Ecological Model to the Baby-Friendly Hospital Initiative. BFHI, Baby-Friendly Hospital Initiative; SEM, Social Ecological Model; Ten steps, ten steps to successful breastfeeding.
Baby-Friendly Practices Defined
Baby-Friendly USA is responsible for the initiative's implementation in the United States. 17 The 4D pathway to Baby-Friendly designation requires facilities to commit time, staff training expenses, and designation fee expenses.17,39 This pathway is a four-phase designation process involving changes in institution “policies, curriculum, action plans, quality improvement projects, staff training, and competency verification”,17, para.3 as well as a site visit to determine whether the facility has implemented all standards necessary to be awarded Baby-Friendly status. Moreover, successfully following the 4D pathway requires nurses to commit to the Baby-Friendly philosophy, as operationalized through the Ten Steps to Successful Breastfeeding.40,41 The “Ten Steps” document outlines the systematic changes necessary to support mothers and to influence breastfeeding attitudes.
As previously discussed, there is no specific underlying theory to support the tenets of the BFHI. Rather, the initiative was developed and launched by the WHO and UNICEF in 1991 after release of the Innocenti Declaration of 1990.42,43 The Declaration called for national governments and healthcare organizations to develop maternity care policies and procedures that implement the “Ten Steps” and “reinforce all actions that protect, promote, and support breastfeeding”.42, para.6 Specific tools to aid implementation of the initiative were then developed through expert opinion and field testing. 43 Additional staff education materials, a site self-appraisal tool, and a site assessment tool were also developed to help determine a facility's adherence to the Baby-Friendly standards.
For the purposes of this review, Baby-Friendly Practices are defined as breastfeeding promotion interventions in a birthing facility or hospital that align with the Ten Steps to Successful Breastfeeding. An operational definition of Baby-Friendly practices can be obtained by examining the guidelines and evaluation criteria outlined by Baby-Friendly USA, collecting data to determine a facility's adherence to the criteria, and collecting data on maternal/infant health and breastfeeding outcomes. 17 This includes the number of Baby-Friendly practices experienced by mothers, rates of breastfeeding initiation, exclusivity, and duration, as well as early infant health outcomes of neonatal weight loss, hyperbilirubinemia, hypoglycemia, and hypothermia. 17
Methods
Integrative review method
The integrative review is a broad review encompassing both empirical and theoretical literature, as well as experimental and nonexperimental studies. Whittemore and Knafl note that, “well-done integrative reviews present the state of the science, contribute to theory development, and have direct applicability to practice and policy”.44, p.546 “Methodological rigor”p.548 for an integrative review is upheld by maintaining the structured process for including a “formulation stage, a literature search stage, a data evaluation stage, a data analysis stage, and a presentation stage”.44, p.548
The problem identification stage for this review comprised discovery of the concept and population of interest, the context of the inquiry, and additional variables relevant to the investigation. 44 Second, determination of the literature sampling approach included five searched databases, literature from the past 5 years, other relevant studies identified through the ancestry method, and the general study inclusion/exclusion criteria. The data evaluation stage included critical appraisal of both empirical and theoretical reports and involved classification of the articles using the 2009 Oxford Scale for Levels of Evidence 45 for empirical studies and a Melnyk and Fineout-Overholt ranking scale 46 for qualitative studies. The data analysis stage included extraction of the data from the articles with the data ordered and organized into a matrix table format (available from author by request). 44 Finally, the Results section includes matrix data organized into a results table (Table 1) according to levels and factors of the BFHI associated with the SEM.
assoc., association; BF, Baby-Friendly; bili, Bilirubin; BMC, Boston Medical Center; FTT, failure to thrive; GA, gestational age; HCPs, healthcare providers; IBCLCs, International Board Certified Lactation Consultants; IFPS II, Infant Feeding Practices Study II; PRAMS, Pregnancy Risk Assessment Monitoring System; RMS, Ross Mothers Survey; SEM, Social Ecological Model; SES, socioeconomic status.
Literature search
A literature search for the review included identification of studies measuring early health outcomes and breastfeeding outcomes related to Baby-Friendly practices in U.S. settings using PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsychINFO, PsychARTICLES, and Scopus databases. The key term “Baby Friendly Hospital Initiative” was used for the initial search (N = 911, all years; N = 385; 2010–2015). A subsequent search included the field terms “Baby-Friendly” and “United States” yielded N = 187 articles. Titles and abstracts were reviewed for mention of health and breastfeeding outcomes in U.S. settings.
Studies from years 2010 to 2015 were included if measures of health or breastfeeding outcomes were addressed and the studies occurred in the United States. The ancestry method was used to extract frequently cited studies in the literature. 44 Five relevant studies conducted before 2010 were identified using this method.25,47–50 These studies were conducted at Boston Medical Center and provided valuable evidence related to Baby-Friendly practices and breastfeeding outcomes in racially/ethnically diverse and low-income populations. Additionally, these studies provide evidence for the impact of Baby-Friendly practices in the neonatal intensive care unit (NICU). The final sample included two information sources on U.S. breastfeeding policy and 16 articles of original research on Baby-Friendly practices and associated health and breastfeeding outcomes. A flow chart for study inclusion is presented in Figure 2.
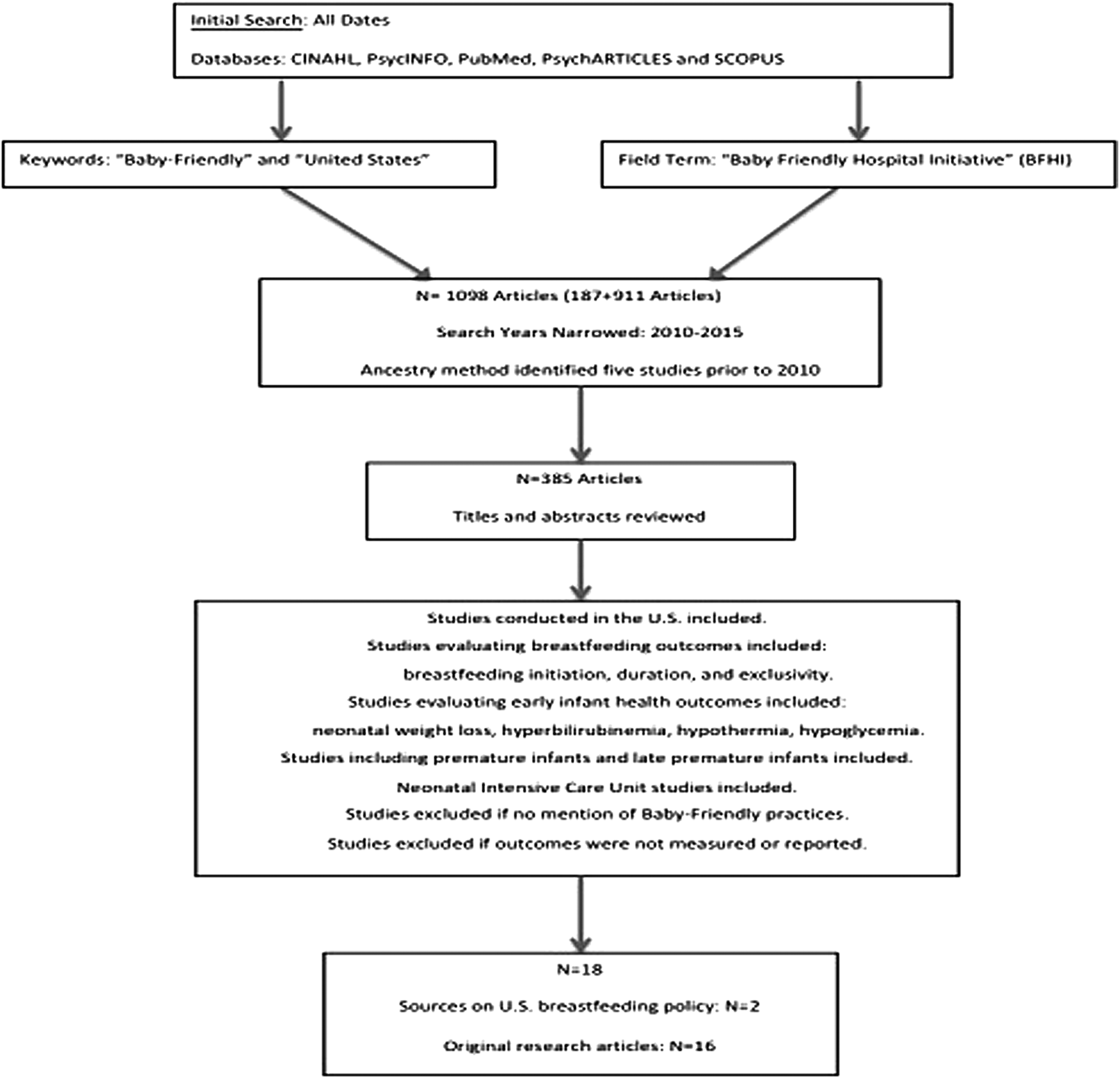
Flowchart for study inclusion in review.
Results
Baby-Friendly Results by SEM Level table (Table 1) represents data extracted from 18 total sources and provides information on breastfeeding outcomes, early infant health outcomes, experiences and perceptions related to the BFHI, and the impact of hospital policy and environment on outcomes. Application of the SEM allowed for stratification of the extracted data into outcomes and factors at the maternal/infant dyad level, the provider level, the hospital/organizational level, and the systems level. Further codification of maternal/infant dyad factors produced three sublevel categories of maternal/infant breastfeeding outcomes, early infant health outcomes, and maternal perceptions. Presenting the results in this manner emphasizes the interrelatedness of factors within the BFHI, facilitates identifying strengths and weaknesses at each level, and presents evidence of the documented breastfeeding and early infant health outcomes at each level.
Summary of Findings/Implications for Future Practice
Maternal/infant dyad factors
Evidence is well documented from U.S. studies that have evaluated and supported the effectiveness of the BFHI for increasing rates of breastfeeding initiation and exclusivity.25,26,49–54 Evidence also suggests that Baby-Friendly practices contributed to increased duration of breastfeeding, although these results should be interpreted with caution due to inconsistencies in charting and reporting of breastfeeding duration rates.38,47,48,53,54 Studies including racial/ethnic minorities, mothers with lower education, and low-income mothers have demonstrated that the BFHI positively affects breastfeeding outcomes in disadvantaged groups.26,50 However, no studies produced BFHI or breastfeeding impact results for women living in rural areas or southeastern regions of the United States.38,54
Evidence is limited for the impact of the BFHI on early infant health outcomes (neonatal weight loss, hyperbilirubinemia, hypoglycemia, and hypothermia). Baby-Friendly practices have been successful in the NICU environment, but late premature infants who remain in normal newborn nursing care may be more susceptible to a lack of appropriate breastfeeding support and may be at an increased risk for poor early infant health outcomes.29,49,51
While evidence supports implementation of the BFHI as a best practice standard, causal mechanisms for the success of Baby-Friendly practices in improving breastfeeding outcomes have not been identified.1,30 Potential causal mechanisms may include variation in practice delivery, variation in maternal attitudes and demographic variables, and how practice delivery influences maternal barriers or facilitators to acceptance of Baby-Friendly practices and breastfeeding. Studies examining mothers' perceptions and experiences with breastfeeding in Baby-Friendly environments are lacking; thus, it is unclear how those Baby-Friendly experiences or perceptions influence breastfeeding decisions. 30
Provider factors
The more training a healthcare provider received, the more likely the provider would comply with Baby-Friendly practices and commit to the Baby-Friendly philosophy.26,30,37,50 All healthcare providers, including lactation consultants and physicians, are important to support mothers in Baby-Friendly experiences and breastfeeding success.
Hospital/organizational factors
The dose–response relationship of number of Baby-Friendly practices a facility implements for successful maternal/infant breastfeeding outcomes emphasizes the need for consistency in hospital organizational factor implementation.26,37,47,52–54 Thus, there remains a need to emphasize consistent delivery of Baby-Friendly practices within facilities to ensure that mothers experience breastfeeding education and support across all maternal/infant stages.
Systems factors
The majority of evidence regarding breastfeeding outcomes in the United States is from retrospective observational survey design studies. History, maturation, and participant report biases present threats to validity when utilizing these retrospective self-report designs.55–57 Prospective studies are needed ideally with participants randomized to breastfeeding promotion interventions to track associated breastfeeding initiation and duration rates. 1 Breastfeeding duration is difficult to track due to inconsistencies in charting and a lack of postdischarge breastfeeding tracking systems. 27 There is a need for a unified tracking system in the United States, as well as a need for standardization of breastfeeding definitions and breastfeeding-related charting in hospitals and birthing facilities.
Limitations
This review was limited to studies conducted in the United States, thus potentially missing lessons learned from studies conducted in other countries. Additionally, articles were only included if outcomes were reported or measured. Studies addressing barriers or facilitators to implementation of the BFHI, without mention of outcome measures, were not included in the current review. Therefore, exclusion criteria could have limited the availability of qualitative evidence to address BFHI implementation factors.
Conclusion
Data for this review provide valuable insights to inform systematic modification of breastfeeding policies and initiatives associated with Baby-Friendly practices on multidimensional and systems levels. Results from the review support the BFHI's success in facilitating successful breastfeeding initiation and exclusivity. Breastfeeding duration appears to increase when mothers have increased exposure to Baby-Friendly practices, but deficiencies in breastfeeding tracking mechanisms result in limited reliable breastfeeding duration data.
The underlying mechanisms by which Baby-Friendly practices contribute to maternal breastfeeding decisions remain unclear; thus, studies are needed to examine mothers' experiences and perceptions of Baby-Friendly practices. Additionally, studies are needed to address Baby-Friendly and breastfeeding barriers for women living in rural areas or in southeastern regions of the United States. Finally, studies are needed to examine early infant health outcomes related to the BFHI.
Prospective studies are needed that include breastfeeding promotion initiatives, explore maternal experiences and perceptions with Baby-Friendly practices, and track maternal breastfeeding decisions. Results from future qualitative and quantitative explorations could further clarify how the delivery of Baby-Friendly practices leads to successful breastfeeding and improved infant health outcomes.
Footnotes
Acknowledgments
The authors would like to thank John D. Dinolfo, PhD (Professional Communication Scholar in Residence, Center for Academic Excellence and Writing Center, Medical University of South Carolina) for contributions to article development.
Disclosure Statement
No competing financial interests exist.
Appendix A
Ten Steps to Successful Breastfeeding:
1. Have a written breastfeeding policy that is routinely communicated to all healthcare staff. 2. Train all healthcare staff in the skills necessary to implement this policy. 3. Inform all pregnant women about the benefits and management of breastfeeding. 4. Help mothers initiate breastfeeding within 1 hour of birth. 5. Show mothers how to breastfeed and how to maintain lactation, even if they are separated from their infants. 6. Give infants no food or drink other than breast milk, unless medically indicated. 7. Practice rooming in—allow mothers and infants to remain together 24 hours a day. 8. Encourage breastfeeding on demand. 9. Give no pacifiers or artificial nipples to breastfeeding infants. 10. Foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or birth center.