
Abstract
Abstract
Introduction:
World Health Organization breastfeeding guidelines for HIV-infected mothers are exclusive breastfeeding for 6 months and then continued breastfeeding for 12 months, provided the mother is receiving antiretroviral prophylaxis. Many African women perceive that breastmilk alone is not sufficient for their infant's nutritional requirements for the first 6 months of life, and mixed feeding is a common practice.
Methodology:
A stable isotope technique was used to determine breastmilk output volumes and maternal body composition objectively at five different time points in the first year of the infant's life.
Results:
Breastmilk output volumes were high for HIV-infected mothers: 831 ± 185 g/day at 6 weeks; 899 ± 188 g/day at 3 months; 871 ± 293 g/day at 6 months; 679 ± 281 g/day at 9 months; and 755 ± 287 g/day at 12 months. These high output volumes had no negative impact on the mother's fat-free mass. The breastmilk output volumes for HIV-uninfected mothers were not significantly different to the outputs for HIV-infected mothers at any of the time points (p > 0.05): 948 ± 223 g/day at 6 weeks; 925 ± 227 g/day at 3 months; 902 ± 286 g/day at 6 months; 746 ± 263 g/day at 9 months; and 713 ± 264 g/day at 12 months.
Conclusion:
This study using objective methodology shows that breastmilk outputs of HIV-infected mothers were relatively high (and within published reference ranges), and mothers are able to provide sufficient breastmilk for their infants without compromising their own fat-free mass.
Introduction
T
Mixed feeding is common practice in South Africa, even where infants start with exclusive breastfeeding 4 (or exclusive formula feeding). The risks associated with exclusive breastfeeding compared with mixed feeding with formula and solid foods have been reported.5,6 Infants who were exclusively breastfed were less likely to become infected with HIV than the latter, and mortality was reduced.
A gold-standard stable isotope method has enabled objective determination of the infant's breastmilk intake and, by inference, the breastmilk output of the mother.7,8 The method also simultaneously yields information about the mother's body composition. Breastmilk intake volumes determined from the stable isotope technique were found to be comparable to the test weighing method. 9 This latter method is thought to underestimate the intake of breastmilk due to insensible water losses during feeding; it disrupts the normal pattern of feeding and is therefore inconvenient for the mother, especially when she is feeding at night and on demand, and these feeds may be excluded. 10
Maternal body composition during lactation is of interest in a population that is poor and especially if the mother is HIV-infected, since maternal weight loss and loss of fat-free mass in HIV-infected mothers can put an increased burden on the mother's nutritional status. 11 Hence, this study also investigated maternal body composition according to the maternal HIV status. Many African studies have focused only on weight changes during lactation, for example in Rwanda, 12 Zambia, 13 and a study of five African sites, including one in Durban, South Africa. 14 A review of the published studies of body composition of lactating women found that the results were very variable, showing both increases and decreases in maternal weight during lactation. 15 Some studies have used maternal weight and BMI as indicators, and studies related to breastfeeding have yielded mixed results and followed up mothers for different periods of time.16,17 A variety of methods are available to determine maternal body composition. Some studies have assessed maternal body fat by skinfold thickness,18,19 but these are reported to be subject to errors in measurement. 20 Underwater weighing 21 and the Bod Pod 17 can also be used to determine body density and body fat. In a study in South Africa, maternal body composition during lactation was measured by bioimpedance spectrometry from 8 to 24 weeks post-delivery. 22
The deuterium dilution method can also be used to determine maternal body composition in terms of whole-body fat and fat-free mass and was used in a study looking at whether nutritional supplementation would alter fat-free body mass in lactating mothers, which is of particular importance for HIV-infected mothers. 23 To the authors' knowledge, there are few studies that have measured post-delivery maternal fat-free mass changes in conjunction with determination of the breastmilk output volumes, using the deuterium dilution technique for both measurements. Two studies of lactating mothers were carried out in different communities in Kenya, but both studies had limited sample sizes of only 10 mothers.24,25 A study in Mexico used the deuterium dilution technique to measure maternal body composition, but breastmilk intake volumes were determined by the test weighing technique. 26 Neither of these studies looked at the effect of lactation on maternal body composition in the context of HIV-infected mothers. Therefore, this study will add important information to the field.
Materials and Methods
Study population
The study site was the Umkhumbane Community Health Centre (also known as the Cato Manor Clinic) in Cato Manor, Durban, South Africa, which is situated approximately 8 km from the city center. The area is characterized by high unemployment and high HIV prevalence rates, and contains a mixture of both formal and informal dwellings, many of which do not have access to a piped water supply and flush toilets in their homes. Infants in this disadvantaged community are therefore at risk when using mixed or replacement feeding.
Mothers were recruited from antenatal or postnatal visits at the Cato Manor Clinic to participate in the Improved Nutrition Program, which took place concurrently at the clinic and was conducted by the Department of Paediatrics and Child Health of the University of KwaZulu-Natal. The program aimed to educate, support, and encourage mothers to breastfeed their infants regardless of maternal HIV status, and covered topics such as correct positioning of the infant, common breastfeeding problems, introduction of complementary foods, gardening, and general life skills. Mothers who participated in the Cato Manor Clinic Improved Nutrition Program with a new baby and met the study's inclusion and exclusion criteria were invited to take part in this study (The Breast Milk Intake Study), which involved five visits at the following time points post-delivery: 6 weeks, and 3, 6, 9, and 12 months. After being informed about the study requirements and procedures, all mothers signed a consent to participate. Recruitment continued until 100 mother–infant pairs were enrolled and had completed at least one study time point. Ethical approval (BE211/11) was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (UKZN-BREC).
Inclusion criteria for the mother were initially that the mother was healthy, had no HIV or other infectious disease, intended to breastfeed her baby for 12 months, was participating in the Improved Nutrition Program, intended to live in the neighborhood of the clinic for 12 months after delivery, and was African. However, the number of women recruited with these criteria was low. Hence, an amendment was approved by the UKZN-BREC to allow asymptomatic HIV-infected mothers to participate in the study from March 2013. Exclusion criteria for the mother were pregnancy and a body mass index (BMI) <18.5 kg/m2. Inclusion criteria for the infant were full term, and a birth weight >2.3 kg. Exclusion criteria for the infant were twins, any defect that interferes with feeding, and chronic illness (e.g., congenital heart disease, cerebral palsy, etc.).
Maternal HIV status was determined from the clinic records (infant's Road to Health card), but 2/100 mothers in the study did not want to disclose their HIV status. Of the resulting 98 mothers, 40 were HIV-infected. The mean BMI was 27.2 ± 5.1 kg/m2 for the 40 HIV-infected mothers and 26.7 ± 4.7 kg/m2 for the 58 HIV-uninfected mothers at enrolment. The difference in means was not statistically significant.
Methods
Breastmilk output volumes were determined using the dose-to-mother deuterium dilution method, whereby the mother drinks a 30-g dose of deuterium oxide, which mixes rapidly with her body water. 7 Saliva samples are taken from the mother and infant prior to the dose and over a period of 14 days thereafter. The deuterium enrichment in the mother's and infant's saliva is measured compared to their pre-dose saliva sample using a Fourier Transform Infrared Spectrometer (FTIR), and these values are then fitted to model curves using the Solver function in Microsoft Excel®, which minimizes the sum of the squares of the differences of the FTIR and model values. Values for the breastmilk intake of the infant and, by inference, the breastmilk output of the mother are then calculated from these data. 7
Maternal body composition can be determined from the same deuterium dilution method used for measurement of breastmilk intake volumes. 7 Since the mothers drink a dose of deuterium and the natural logarithm of the mother's deuterium enrichment when plotted against time gives a straight line, the intercept on the y-axis gives the deuterium enrichment at time 0. The pool space or volume distribution of deuterium, VD, is calculated from the deuterium dose given to the mother divided by the deuterium enrichment at the intercept. This value is then adjusted, as some of the deuterium is also involved in non-aqueous isotopic exchange, mainly in proteins. This is estimated to amount to 4.1% of the pool space. Hence, the mother's total body water (TBW) is calculated as: TBW (kg) = VD/1.041. Fat-free mass is then calculated using the mother's hydration coefficient, which is a constant 73.2% water in adults as follows:
Fat-free mass (kg) = TBW (kg)/0.732.
Percentage fat-free mass can then be calculated using the mother's body weight.
The WHO 24-hour recall was used to determine mother's report of infant feeding, 27 and infants were classified as exclusively breastfed if they received breastmilk, vitamins, mineral supplements, and medicine only, in line with the WHO definition of exclusive breastfeeding. 28
Statistical analysis
Sample size
The sample size had been set up to assess the breastmilk output of mothers accurately, and it was initially assumed that there would be only HIV-uninfected mothers. Since the change in study resulted in 40% HIV-infected mothers being recruited, it was realized that it would be possible to examine differences in breastmilk output in the two different groups of mothers. With the sample size, there was an 80% power to detect a 200 g/day difference in breastmilk output between HIV-infected and HIV-uninfected mothers, which was considered to be a meaningful difference.
Data analysis
Box and whisker plots were constructed using Microsoft Excel and the two-sample independent t tests were calculated at the 95% confidence level using Open Epi Software. Bivariate linear regression analyses were carried out using Stata v13 (StataCorp, College Station, TX).
Results
Breastmilk output
During the analysis of the deuterium results and computation of breastmilk intake volumes, 9/332 values measured were excluded, as the breastmilk, non-milk oral, or total water intake was >1700 g/day. This value has been used as the exclusion criterion in other studies, 29 and values >1500 g/day are to be investigated further in line with the guidelines for the method. 30 One value for total water intake was very low (108 g/day at 12 months), and this value was therefore not included in the statistical analysis. In addition, 17 results did not fit the model, some of which were due to incomplete sample collection or sampling errors and could not be included in the results. The number of measurements that were excluded is not unusual for a method as complex as this, and similar levels are reported in other published studies. 31 Figure 1 shows the breastmilk intake volumes for all infants over the period 6 weeks to 12 months. In bivariate linear regression, these breastmilk intake volumes were not associated with infant birth weight, infant sex, maternal age, maternal BMI, or maternal education at any of the five time points (p > 0.05).
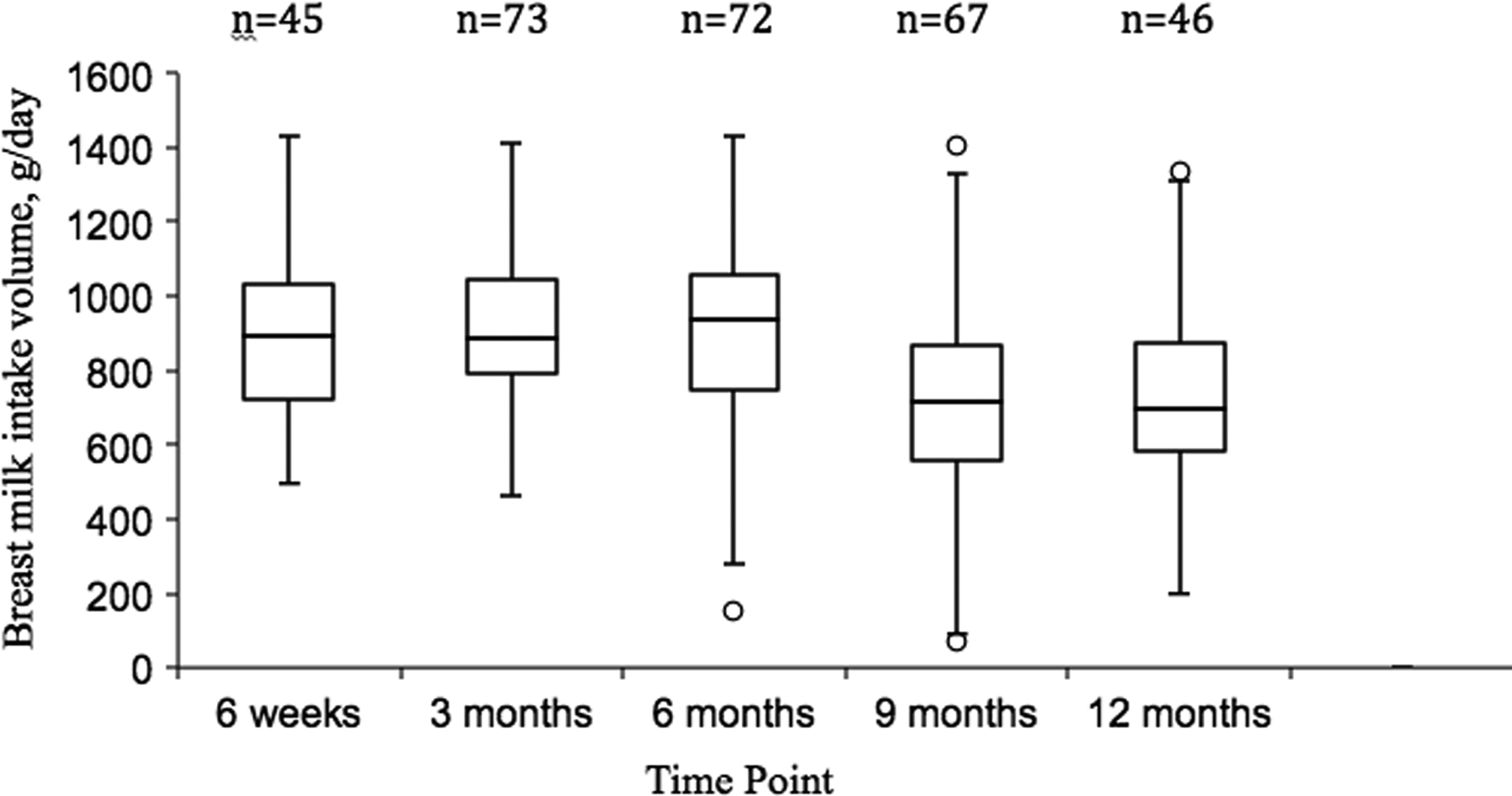
Box and whisker plot of breastmilk intake volumes for all infants over the course of the study.
Mean breastmilk intake volumes for HIV-infected and -uninfected mothers and corresponding infant weights are shown in Table 1. The means of the breastmilk intake volumes according to maternal HIV status at each time point were compared, and no difference was statistically significant. The HIV-infected mothers' reports of infant feeding gave 90.5%, 92.9%, and 70.4% as exclusively breastfeeding at 6 weeks, 3 months, and 6 months, respectively; and the HIV-uninfected mothers' reports gave 83.3%, 86.0%, and 54.5% as exclusively breastfeeding at 6 weeks, 3 months, and 6 months, respectively.
Mean ± standard deviation.
t Test for BMIV.
BMIV, breastmilk intake volume.
Fat-free mass measurements
During the analysis of the deuterium results and the computed fat-free mass values, 5/342 values measured were not valid and were therefore not included in the statistical analysis. In addition, nine results did not fit the model, some of which were due to incomplete sample collection or sampling errors and could not be included in the results.
Table 2 shows the change in maternal fat-free mass between two adjacent time points and over the full observation period from 6 weeks/3 months to 12 months, according to the maternal HIV status. A two-sample independent t test was used to compare the mean change in maternal fat-free mass, and there was no statistically significant difference in the means.
Mean ± standard deviation.
FFM, fat-free mass.
Discussion
The dose-to-mother deuterium dilution technique is considered by some to be a gold standard for measuring breastmilk output volumes. 32 The breastmilk output volumes measured using this technique were high for both HIV-infected and -uninfected mothers for the first 6 months in comparison to the volumes reported in a pooled study of breastmilk intake in 12 countries using the same deuterium dilution technique. 29 These pooled results gave mean breastmilk intake volumes of approximately 700 g/day at 1–2 months, 820 g/day at 3–4 months, and 810 g/day at 5–6 months, which were lower than those obtained in this study for HIV-infected and -uninfected mothers. The mean infant weights at the comparable time points of 3 and 6 months were lower than for the current study, which corroborates the higher breastmilk intake volumes seen in the present population, since other studies have reported a strong positive correlation between breastmilk intake volumes and infant weight. 33 The 9–10-month intake in the pooled study was >900 g/day (n = 75) but came from only three of the countries (Malawi, Papua New Guinea, and Zambia) and is higher than in the present study. The 11–12- and 12–24-month intake came from two countries (Gambia and Papua New Guinea; n = 53) and was 800 g/day for 11–12 months and 630 g/day for 12–24 months compared with the present study's mean of about 713–755 g/day at 12 months, depending on HIV status. These results are more difficult to interpret, since the effect of complementary feeding after 6 months is such as to make comparison between study populations more difficult. Furthermore, in the pooled study, the mean infant weights from 10 months were much lower than the mean infant weights at 8–9 months were, indicating that the results from the time points after 10 months were restricted to particular infant populations with much lower mean weights. 29
A recent study also using the dose-to-mother deuterium dilution technique in Sri Lanka 34 reported lower breastmilk intake volumes than the values obtained in the present study and, similar to the results from the pooled study, 29 showed lower infant weights at comparable time points. For example, the 2- to <4-month breastmilk intake in Sri Lanka could be compared to the 6-week intake in South Africa if infant weights were taken into account rather than age. A longitudinal study of breastmilk intakes in exclusively breastfed infants using the test weighing method found a strong positive association between infant weight and the amount of breastmilk consumed by the infant. 35 They compared their results with other studies and found a range of 600–900 mL/day breastmilk consumption during established lactation. A normal breastmilk intake is taken to be 150–200 mL/kg/day up to 5 kg. 36 Hence, for the mean infant weight of 4.86 kg at 6 weeks, normal total breastmilk intake should be 729–972 mL/day. In the present study, the breastmilk intake volumes at 6 weeks for both HIV-infected and -uninfected mothers both fall in this range and can therefore be seen as adequate for infant feeding.
The changes in maternal fat-free mass were relatively small at all time points, and there were no significant differences in the means of HIV-infected compared to -uninfected mothers. In a poor pastoral community in Kenya where food insecurity was common and access to healthcare was limited, a study showed that BMI in lactating women decreased significantly, and maternal weight also decreased over the study period, although this did not reach significance. However, it is difficult to interpret these results due to the small sample size (n = 10) 25 and the very different body composition compared with the current study—this Kenyan study reported a mean BMI that decreased from 19.8 ± 1.3 to 18.5 ± 1.0 kg/m2, whereas in the present study, mothers had a mean BMI at 6 weeks of 26.8 ± 4.5 kg/m2. In addition, the breastmilk output volumes in the Kenyan study were much lower (552 ± 22 mL/day) than the volumes in the current study. In the present study, the mothers had a minimum BMI of 18.5 kg/m2. Hence, it is possible that the results are not applicable to mothers with lower BMI values, even though there was no significant correlation in the present study between maternal BMI and the breastmilk output of the mother at BMI values >18.5 kg/m2. Furthermore, other studies have shown that there is no significant relationship between the mother's BMI and breastmilk output, even at BMI values <18.5 kg/m2. 37
In a study in the same area in South Africa as this study, lactating mothers lost weight and fat-free mass over the study period of 2 weeks to 6 months, but there was not a significant difference in the amount of fat-free mass lost compared to the formula-feeding mothers. 38 A study of the change in the maternal body composition over the period 2 weeks to 6 months in mothers who had/had not received nutritional supplementation 23 showed that mothers had no significant change in BMI, fat-free mass, and fat mass over the study period, which also indicates that the mothers in this area are not undernourished. Hence, the present findings confirm that even high breastmilk output volumes are not detrimental to a mother's health, as there was no significant loss of fat-free mass, and mothers can be encouraged to breastfeed regardless of HIV status.
Limitations
A limitation of the deuterium dilution method is that although it accurately assesses breastmilk intake over the period of observation, it may not represent breastfeeding practices outside this 14-day period. Breastfeeding patterns can vary according to the infant's needs and may not be constant over time. The study was powered to detect a difference in breastmilk output volume of 200 g/day, which was chosen to be a meaningful difference between HIV-infected and -uninfected mothers. This value may seem a rather large value, but in this study, anything less than this value would not be clinically significant, given that the mean breastmilk output volumes were relatively high in the first 6 months (>800 g/day).
Conclusion
This study using objective methodology shows that breastmilk outputs of HIV-infected mothers were relatively high (and within published reference ranges) and mothers are able to provide sufficient breastmilk for their infants without compromising their own fat-free mass. These data endorse the WHO and South African guidelines to encourage 12 months of breastfeeding for HIV-infected mothers.
Footnotes
Acknowledgments
The authors wish to acknowledge the assistance of Gcinile Maphanga, Zanele Msomi, Bathabile Zungu, and Nokukhanya Nzama in completing questionnaires and saliva sampling; Penny Reimers for breastfeeding counseling; Dr. Eshia Moodley for assistance with general study management; eThekwini Municipality for use of the study site; the mothers and infants who participated in this study; and Prof. Benn Sartorius for statistical analysis.
The study was funded by the International Atomic Energy Agency Research Contract No. 16844 and RAF 6039, University of KwaZulu-Natal College of Health Sciences, and the Medical Research Council.
Disclosure Statement
The authors declare no conflicts of interest.