
Abstract
Abstract
Background:
Mothers of very-low-birth-weight (VLBW) infants often struggle to establish and maintain a milk supply. Children's Hospital of Orange County (CHOC Children's) data from 2005 to 2011 showed that while the total percentage of all neonatal intensive care unit (NICU) babies being discharged on breastmilk had remained stable, the percentage of VLBW babies with breastmilk at discharge had declined. This information resulted in a quality improvement initiative to remove barriers and implement programs shown to have the greatest impact on initiating and sustaining lactation in this patient subset. The objective of this initiative was to increase breastmilk availability at discharge for the VLBW population.
Materials and Methods:
A multidisciplinary program was initiated, which included NICU parent and staff education, clarification of roles, and improved access to pumping supplies. Physicians and nurses completed online education. An algorithm defining roles in lactation support was developed, and a resource team of trained bedside nurses was formed. Lactation consultant time was then refocused on the VLBW population. In addition, “Lactation Support” was added to the physician daily documentation to bring the topic to daily bedside rounds. Twice weekly lactation rounds between the lactation consultant and neonatologist addressed lactation concerns for each dyad. To address pumping issues, the loaner pump program was enhanced.
Results:
To assess the effectiveness of the initiative, breastmilk availability at discharge for the VLBW population at CHOC Children's was compared from baseline (2011) to the end of June 2015. VLBW breastmilk availability at discharge upon project initiation was 58.7% and increased by 36% to a final rate of 80% by 2013—a rate sustained through the first 6 months of 2015.
Conclusions:
The results of this initiative suggest that a multidisciplinary approach, including education, changes in workflow, and redefinition of roles, is effective in improving breastmilk rates at discharge in the VLBW patient population.
Introduction
T
However, despite the even greater need for breastmilk, mothers of preterm infants have lower breastfeeding initiation rates, and mothers of very-low-birth-weight (VLBW) infants are least likely to initiate and maintain lactation.1,2,5–8,10,11 This is primarily due to the fact that lactation in this population depends on the ability to initiate and maintain a milk supply by pumping and that mechanically expressing milk for a prolonged period makes it difficult to achieve and maintain adequate volumes. Milk volumes of mothers of preterm infants often decline between 2 and 6 weeks, which may occur well before hospital discharge. Furthermore, preterm infants are disproportionately born to socioeconomically disadvantaged mothers, a group already shown to have barriers to initiating and maintaining lactation.1,2,5–8,10,11
Barriers to lactation in the general population include employment status and return to work plans, socioeconomic status, culture and attitudes, lack of family support, and maternal confidence in breastfeeding abilities. 4 The preterm population faces additional challenges. 4 Pregnancy-related maternal medical complications may delay initial pumping. Lack of privacy within the neonatal intensive care unit (NICU) setting may inhibit mothers from pumping as frequently as necessary, and lack of an adequate hospital-grade pump at home may keep a mother from obtaining and maintaining a milk supply. 5 Mothers with a suboptimal supply may express disappointment over pumping such small volumes and quit the process altogether. In addition, the stress of having a baby in the NICU, separation from the infant, having a long distance to travel to the NICU, and/or the need to return to work may all inhibit successful lactation.2,5,7,11
Barriers within the hospital culture also impact lactation success. The need, or perceived need, to measure exact intake, the common misconceptions that the first feeding should be with the bottle, and that a preterm infant should do all bottle feedings to discharge home sooner all negatively impact breastfeeding success in this vulnerable population.
However, reports in the literature indicate that increased maternal support directed at behavioral factors has a positive impact on breastmilk availability for the preterm infant. 11 Such interventions include access to lactation consultants, immediate access to a hospital-grade pump, providing assistance in obtaining a pump for home, educational sessions for mothers during the antenatal period regarding role of breastmilk, a consistent and clear message regarding the importance of providing milk reinforced by all care providers, and peer counselors or support programs.5,8,11,12
Based on these concepts, the Children's Hospital of Orange County (CHOC Children's) sought to remove barriers by implementing programs shown to have the greatest impact on initiating and sustaining lactation.
Materials and Methods
Because of the importance of breastmilk in the preterm infant, CHOC Children's tracked the availability of breastmilk at the time of hospital discharge for all NICU patients as part of data submitted to the California Perinatal Quality Care Collaborative. Results showed that while the percentage of all NICU infants receiving any breastmilk at discharge remained constant at ∼78% between calendar years 2005 and 2011, the availability for the VLBW population had decreased from a high of 68% in 2008 to 58.7% in 2011 (Fig. 1). Therefore, a lactation quality improvement (QI) team was formed and met monthly to review progress and work on initiatives. It was determined that the team would work on initiatives that would promote lactation throughout the NICU (and the rest of the hospital), but that efforts would focus on the VLBW infant (<1,500 g) and particularly those cohorted in the CHOC Children's Small Baby Unit for infants born <1,000 g at birth. The goals of the team were to identify barriers to lactation, identify best practices to improve lactation rates, optimize available resources, and improve staff and family education. The initial team members included the lactation medical director (a neonatologist), the director of the Clinical Nutrition and Lactation Department (a registered dietitian and International Board Certified Lactation Consultant [IBCLC]), the two NICU lactation consultants, and the two NICU registered dietitians. Over time, the team expanded to include the NICU clinical nurse specialist, two NICU occupational and speech therapists, and a bedside NICU registered nurse (RN). Additional bedside nurses, neonatal nurse practitioners, and others were added on a project-specific basis as ad hoc or virtual (e-mail) members.

Percentage of patients with breastmilk available at neonatal intensive care unit (NICU) discharge 2005–2011.
The first initiative focused on IBCLC staffing and bedside RN training. One non-NICU IBCLC full-time equivalent (FTE) was reallocated to provide a total of 2 lactation FTEs for the 67-bed NICU. The team recognized that despite doubling IBCLC hours for the NICU, the bedside RN would be the key to successful lactation support and promotion and noted that there was a wide range in skills and comfort with lactation among the direct care providers. Research suggests that nursing knowledge or attitudes can influence mothers' breastfeeding decisions in the NICU, supporting the team's desire to provide training to the RN staff. 2 Initial education was provided through a mandatory online lactation module that emphasized lactation basics and included video instructions on pumping, hand expression, hands-on pumping, and initiating direct breastfeeding. Three optional didactic modules were also made available through the hospital online learning system with 189 staff completing module 1, 143 completing module 2, and 125 completing module 3. A NICU RN Lactation Resource team was identified with the goal of having bedside staff with additional lactation training to assist their peers due to the limited IBCLC resources. Eighteen NICU RNs volunteered for additional training, which was provided through several venues. Five 1-day, instructor-led didactic courses were offered. To promote further lactation education, CHOC Children's began to host the 5-day University of California San Diego Extension Lactation Educator Counselor training program (http://extension.ucsd.edu/studyarea/index.cfm?vCourse=RMED-40006) yearly and encouraged all staff involved with breastmilk or infant feeding to utilize the hospital tuition reimbursement program to attend the course. To date, over 70 CHOC Children's associates have completed the course.
In addition to staff education, a lactation care map was created that outlined key points of lactation care to be provided by the bedside RN and the IBCLC. The goal was to improve lactation care and breastmilk availability rates through using consistent messaging among all healthcare providers, ensuring around the clock availability of information, promoting early and timely initiation of milk expression, and optimizing the limited hours of the lactation consultants. An algorithm outlining basic lactation care and delineation of duties was created (Fig. 2).
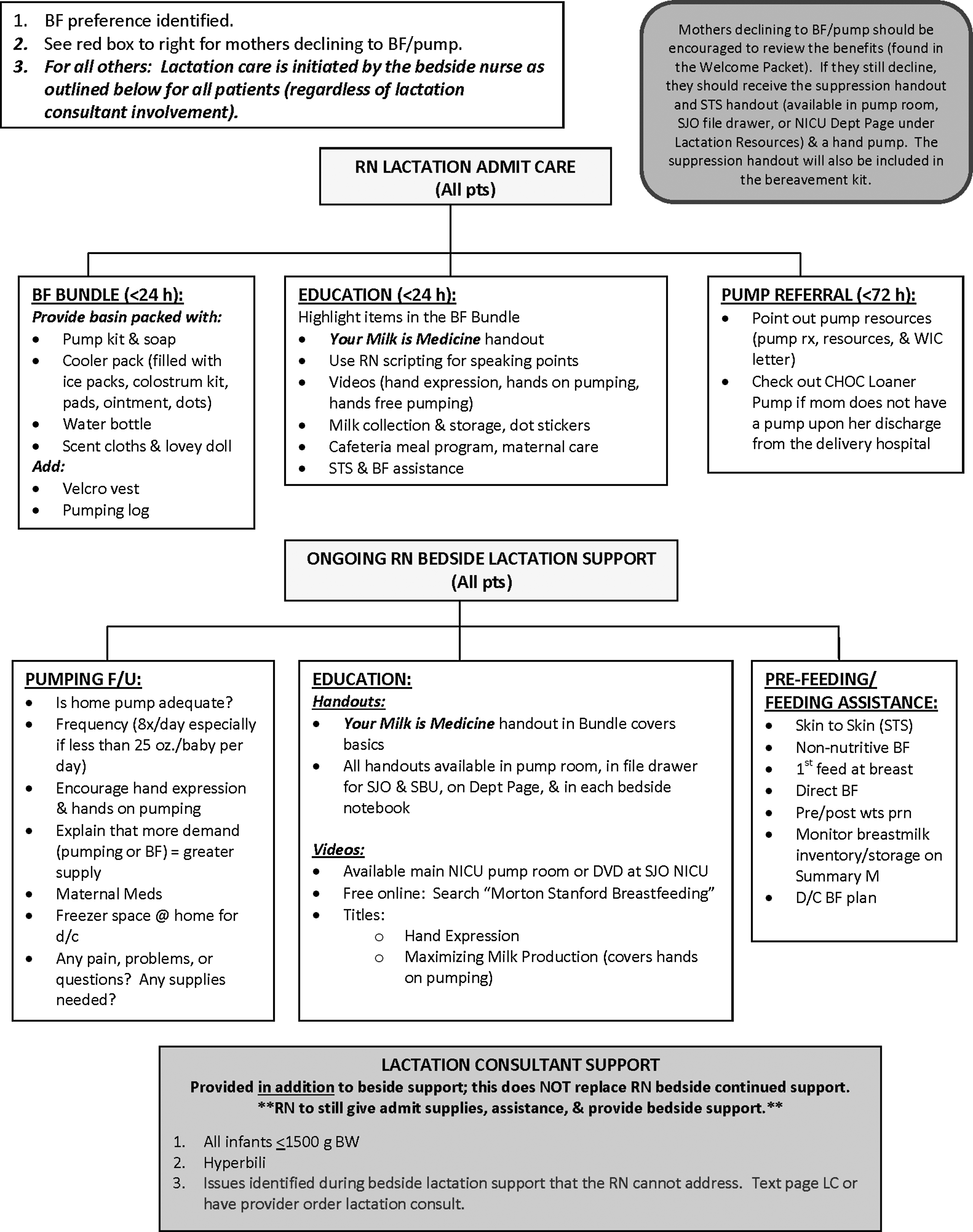
NICU lactation bedside care algorithm.
It was also understood that physicians could have a strong impact on supporting and promoting lactation.13,14 The QI team felt that having the attending physician discuss and reinforce lactation with the mother helped highlight its importance within the medical care the infant was receiving. To ensure consistency of messaging, all of the neonatologists completed an online lactation module (The Breastfeeding Friendly Consortium—Breastfeeding Training). A problem titled “Lactation Support” was added to the daily provider note, and lactation was discussed daily during bedside rounds that included parents. In addition, the attending neonatologist and the lactation consultants conducted twice weekly lactation rounds. The purpose was to identify mothers at risk for lactation failure so that the neonatologist could provide additional encouragement and support to the mother. This was felt to potentially be more authoritative than the same message from the bedside RN or IBCLC. The lactation rounds were initially all in person, but then moved to virtual rounds (through e-mail communication) for better time management when appropriate with in person rounds as needed.
Within the VLBW population, the need for a hospital-grade pump to initiate and maintain adequate milk supply is imperative and well supported by the literature.7,11 CHOC Children's had a program to loan hospital-grade breast pumps to NICU mothers on a short-term basis until a pump from their insurance company or the Special Supplemental Nutrition Program for Women, Infants, and Children could be obtained. However, frequent lost or unreturned pumps and the time burden the program was placing on the lactation consultants threatened the program. Pumps had been kept in the NICU, but were often loaned out without any paperwork and were not able to be tracked. Therefore, to sustain and ensure viability, the program was restructured. Loaner pumps in inventory were relocated to the centralized breastmilk preparation room known as the “Nutrition Lab.” The bedside RN could request a pump, which the Nutrition Lab staff would then deliver to the mother in the NICU and track all the way through the return of the pump to inventory. In addition, a grant was secured from the CHOC Children's Foundation to expand the pump inventory from 14 to 20. To assist mothers in securing a breast pump for home sooner (enabling them to return the loaner pump), the lactation QI team enlisted help from the case management department. Case management identified a list of medical equipment vendors for the various insurance plans and made the referrals within 72 hours of NICU admission, dramatically decreasing the turn-around time for a pump to be delivered to the home.
Lactation educational materials for the NICU mothers were also enhanced. Lactation videos and literature were placed in the NICU pumping rooms. In addition, educational materials were added to the prepacked lactation basins, which also included pumping kits and supplies.
To assess the effectiveness of the lactation QI team efforts, breastmilk availability at discharge for the VLBW population at CHOC Children's was compared from baseline (2011) to the end of June 2015. The NICU census remained consistent during the study period. Breastmilk availability was determined by review of the medical record for the 72 hours proceeding discharge to determine if any breastmilk was received. For data collected after initiation of the QI team (2013–2015), the following exclusion criteria were used: conditions where breastmilk use was contraindicated (n = 6 for maternal substance abuse; n = 2 due to need for specialty formula); patients who expired during hospitalization (n = 25); patients transferred to another hospital rather than discharging home (n = 32).
Results
VLBW breastmilk availability at the project initiation was 58.7% and increased by 36% to a final rate of 80% by 2013, which has been sustained through the first 6 months of 2015 (Fig. 3).

Percentage of very-low-birth-weight (VLBW) infants with breastmilk available at hospital discharge.
CHOC Children's uses pasteurized donor breastmilk when appropriate. There had been some concern or speculation that offering donor milk could remove some of the motivation for mothers to provide their own milk. Donor milk usage at CHOC Children's in the fiscal year (FY) 2013 was 11,000 ounces compared to 7,000 in FY 2015—a decrease of 36%, which correlated with the increased percentage of the diet from mothers' own milk rather than formula usage. Our findings supported data from the literature that indicate that use of donor milk reduces exposure to formula, but does not change proportion of diet from mothers' own milk. 15
Discussion and Conclusions
Our data suggest that a multidisciplinary team is effective in improving breastmilk availability at discharge in the VLBW infant population. If breastmilk is not available at the time of hospital discharge, the mother cannot hope to meet the American Academy of Pediatrics recommendation to continue breastfeeding until 1 year of age or beyond. Programs that support sustaining lactation throughout hospitalization are critical. We will continue looking for opportunities to enhance current initiatives. A reminder task list for the RN is being created within the electronic medical record to ensure completion of the tasks on the lactation algorithm. A rotating scholarship is being set up to send more bedside nurses to lactation training programs, and a small number of nurses who have already attended lactation training courses are receiving 20 hours of hands-on lactation training time with the NICU lactation consultants to enhance their knowledge and skills. However, we believe there is an opportunity to take our efforts a step further. Some data suggest that less than half of mothers of VLBW infants who provide expressed milk go on to direct breastfeeding. 11 Lack of direct breastfeeding may be tied to shortened duration of lactation. 11 Therefore, the next area of focus for this QI team will be to increase direct breastfeeding while in the NICU.
Footnotes
Acknowledgments
The authors would like to thank and acknowledge the CHOC Children's neonatologists, NICU registered dietitians, dietetic technicians, developmental team, and NICU nurses for their help and support of these lactation initiatives. These improvements would not have been possible without their input, cooperation, and hard work.
Disclosure Statement
The authors have nothing to disclose.