
Abstract
Abstract
Background:
Breastfeeding rates in the United States are suboptimal. Health professionals (HPs) have a unique opportunity to support breastfeeding because of the frequency and timing of their visits with mothers and infants as well as their call by professional organizations to do so. The objective of this study was to understand HPs' perceived roles and experiences with providing breastfeeding-related care.
Materials and Methods:
In-depth qualitative interviews were conducted with 34 HPs (obstetricians, midwives, pediatricians, nurses, and lactation consultants) who care for pregnant or lactating women. Interviews were audio-recorded, transcribed, and verified for accuracy; content analysis was used to identify themes using a grounded theory approach.
Results:
The overarching theme was discontinuity in breastfeeding care across the continuum. Most HPs relied on other HPs to provide breastfeeding care, which resulted from and contributed to problematic gaps in care that were reported. A minority of HPs attempted to bridge gaps in breastfeeding care or improve continuity. Contributing to the discontinuity were a lack of time, lack of skills, inconsistent messages, and low communication across stages of care. HPs were unsure whether their help was effective and whether required follow-up was completed.
Conclusions:
Despite HPs' recognition of breastfeeding as the best choice for infant feeding, breastfeeding care may be disjointed and a barrier to achieving breastfeeding recommendations. These problems should be investigated and systemically addressed in future research so that maternal–infant dyad breastfeeding care can be improved.
Introduction
B
Health professionals (HPs) have a unique opportunity and responsibility to provide breastfeeding support. Both the American Academy of Pediatrics 1 and the American Congress of Obstetrics and Gynecology 5 strongly support breastfeeding and advocate for their members to be at the forefront of providing such support. Previous studies have cited barriers to HPs providing breastfeeding care, in particular a lack of skills or training and too little time among physicians.6,7 Across the prenatal to postpartum continuum many HPs have contact with mothers and their infants, and each interaction presents an opportunity to educate about or assist with breastfeeding. Breastfeeding is a dyadic behavior, but in the United States care is typically separated for the mother and infant: the obstetrician provides care for the mother and the pediatrician for the infant. These and other HPs, such as nurses and lactation consultants (LCs), interact with the dyad during different periods across the continuum.
Previous research among women and HPs suggested that lack of continuity and gaps in care for women postpartum negatively affected how mothers experienced recovery and body changes after delivery. 8 This research did not specifically investigate breastfeeding care. Other research has indicated inadequacies in breastfeeding care at prenatal visits 9 and postpartum 10 from the mothers' perspectives, but there is little understanding about how HPs themselves experience providing breastfeeding care. Thus, our aim was to understand from HPs' perspectives their experiences providing breastfeeding care across the continuum, barriers they may encounter, and how they manage breastfeeding care within the often complex context of the healthcare system.
Materials and Methods
Data presented here came from a previously described qualitative study 11 with HPs who provided care during the prenatal, perinatal, and postnatal periods. Our aim was to understand HPs' experiences providing breastfeeding care to all women within the settings and systems in which they practiced. We present the results for this aim with key methodological details.
HPs were recruited in two central New York counties via flyers and e-mails sent to HPs in obstetrics, midwifery, family medicine, and pediatric practices' listservs. Recruitment materials indicated that the goal was to learn about HPs' experiences providing care to pregnant and breastfeeding mothers to develop strategies to help them breastfeed longer. Chain-referral was used to reach community-based HPs. Purposive sampling was used to select professionals from a variety of practice types who provided care at different periods across the care continuum. A semistructured in-depth interview was conducted with each participant with written informed consent before each interview. An interview guide (key questions relevant to this study are given in Supplementary Table S1; Supplementary Data are available online at www.liebertpub.com/bfm) with exploratory probes facilitated data collection, but interviews were largely participant-driven. The institutional review boards at Cornell University and the Rochester General Hospital Research Institute approved this study.
Interviews were conducted by C.D.G., took place in locations that participants chose, and averaged 53 (range, 30–110) minutes long. The interviewer collected demographic information about the HPs via questionnaire and recorded field notes about interview details immediately after each interview that were used to provide context when coding transcripts. All interviews were audio-recorded, transcribed verbatim, and checked to ensure accuracy. C.D.G. and S.L.R. independently conducted analysis of transcripts using a grounded theory approach and ATLAS.ti 7 (Scientific Software Development GmbH, Berlin, Germany) to assist with the iterative coding process. The coders used regular peer-debriefing 12 to discuss and come to agreement about coding and analysis, and data collection ceased once data saturation—the point at which no new information was obtained with additional data collection—was reached. The final analysis represents a joint interpretation of the data among the authors.
Results
Participants
Thirty-four HPs, including 29 women, were interviewed. They were 31–84 years old and had spent < 5 to > 30 years in their current professions. Participants were primarily white (n = 30), three were black or mixed race, and two were Hispanic. Practice settings were diverse, including prenatal, perinatal, and pediatric care within hospitals, public health, and community settings (Table 1), in a mix of rural, small town, suburban, and urban settings. Participants identified as LCs had other training as nurses, social workers, and physician's assistants. Both nurse practitioners and all three family physicians provided prenatal and postnatal care for mothers.
Discontinuity of care
The overarching theme that emerged from these interviews was a discontinuity in breastfeeding care. The most salient subthemes were gaps within the healthcare system structure and reliance on other HPs to provide breastfeeding care. Gaps in the system contributed to HPs' reliance on others, and reliance on others also led to gaps in breastfeeding care. HPs' perceived lack of time and skills to provide breastfeeding care also contributed to gaps in care and their reliance on others. Together these circumstances resulted in breastfeeding care discontinuity, including HPs' report of inconsistent breastfeeding messages and possible missed opportunities to provide breastfeeding care for mothers and infants (Fig. 1). The subthemes related to discontinuity of care are described below.
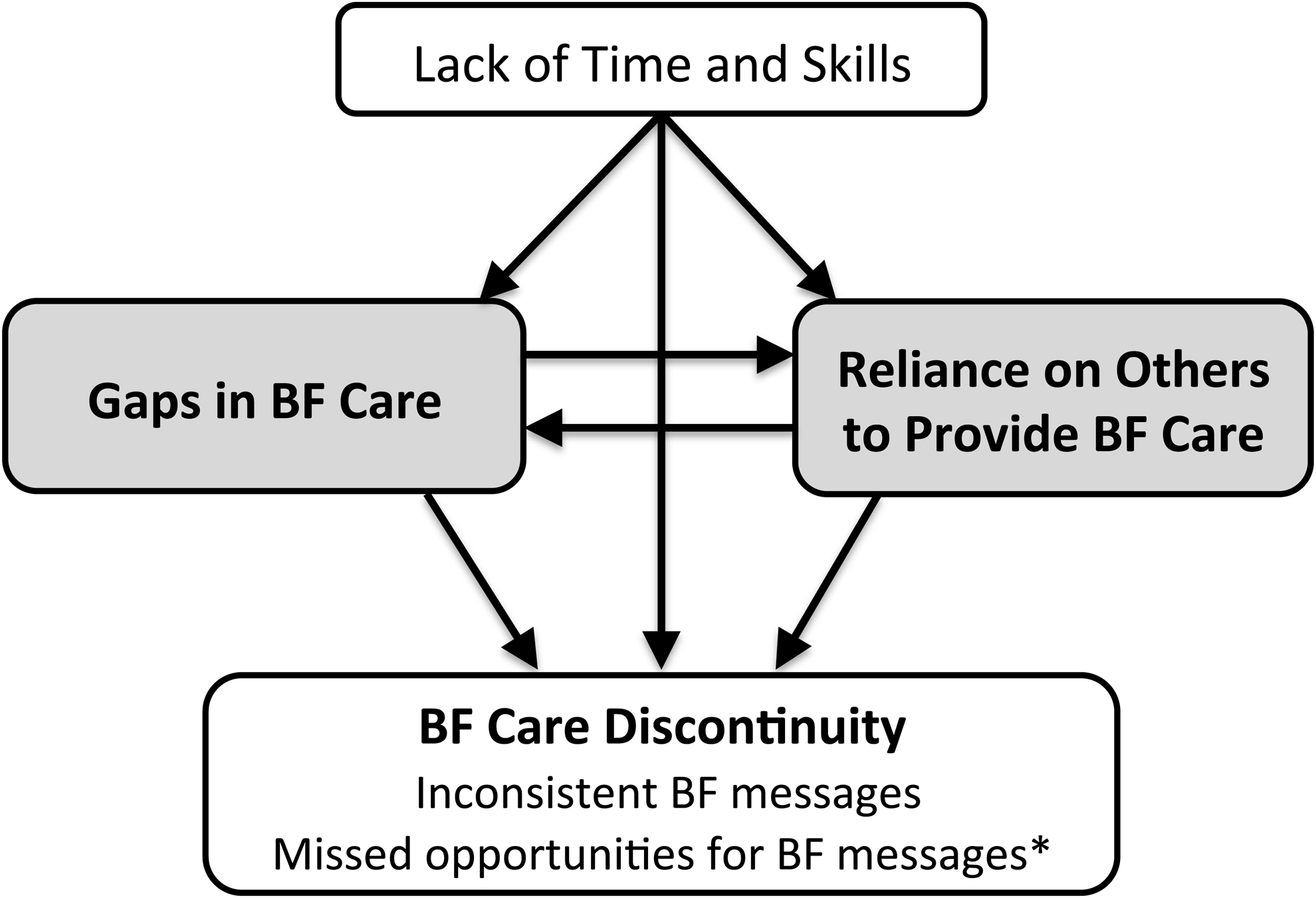
Discontinuity of breastfeeding care resulted from gaps in care, health professionals' reliance on others, and lack of time and skills among health professionals. *Indicates an idea inferred by data; BF = breastfeeding.
Gaps within healthcare system structure
HPs perceived that the structure of the healthcare system contributed to the discontinuity in breastfeeding care. The most commonly discussed problem was the gap in care after delivery (Table 2). HPs who provided prenatal care for women typically did not see women again until 6 weeks postpartum (quotation [Q] 1, nurse practitioner [NP]), and pediatric care providers felt that their visits were too infrequent to support breastfeeding adequately (Q2, medical doctor [MD]). Thus, a critical period was missed when women encountered difficulties with or stopped breastfeeding.13,14 LCs recognized that women also needed support beyond the first few weeks postpartum (Q3, LC) and talked about the important roles of LCs in pediatric offices and Special Supplemental Nutrition Program for Women, Infants, and Children breastfeeding peer counselors. HPs expressed continued breastfeeding care as a “hope” because each HP often did not communicate with the mother's next provider.
CNM, certified nurse midwife; LC, lactation consultant; MD, medical doctor; NP, nurse practitioner; Q, quotation; RN, registered nurse.
Lack of continuity was perceived to arise not only from gaps in care across time, but also from gaps within each stage of the care continuum. HPs who provided prenatal care discussed that patients often see multiple providers, such as in a group practice (Q4, certified nurse midwife [CNM]). Few HPs perceived this as problematic, but one suggested that “perhaps continuity [of providers] would help our patients breastfeed” (08NP). In the hospital, gaps were evident, particularly with nursing care across time (with shift changes) and across nursing specialties. This occurred when different staff members provided care for mothers and their infants (Q5, registered nurse [RN]).
Some HPs felt unable to assess their own effectiveness providing breastfeeding care. Their uncertainty about their effectiveness resulted from not seeing the patients again or knowing their outcomes. This was especially true for hospital-based HPs, who did not have relationships with patients before admission or after discharge (Q6, RN), and for HPs who provided prenatal care but did not see patients until 6 weeks postpartum.
Continuity for the breastfeeding dyad was perceived as more intact by family physicians, as they established relationships with women prenatally and provided follow-up care postdischarge. Hospital LCs reported trying to help bridge gaps in care with services women could call for breastfeeding help (Q7, LC).
Reliance on other HPs
One of the main contributors to discontinuity was that no HP was in charge of breastfeeding care across the entire care continuum:
The problem with breastfeeding is there's no captain of the ship … And it's—there's just nobody that takes that, takes the lead on it. (26MD)
The “no captain of the ship” theme was most clearly presented as HPs who relied on other HPs to assist with providing breastfeeding care (see Supplementary Fig. S1). For example, prenatal care providers relied on instructors of prenatal classes, intake nurses, LCs, nurses in the hospital, and pediatricians. Hospital nurses relied on LCs, who in turn relied on pediatric offices and community resources. Pediatric providers felt that prior providers should have done more prenatally and in the hospital. Each type of HP relied on others across time and across disciplines because of constraints within the healthcare system structure as well as HPs' own skills in breastfeeding care and beliefs about their roles in providing it.
Time: limited or not the right time
Time with patients was a key barrier (Table 3) and a major reason that HPs relied on other HPs across the care continuum. Prenatal care providers discussed the limitations of time at prenatal visits, when much needed to be covered in a short time (Q1, CNM; Q2, MD). Time challenges at pediatric visits were also barriers to breastfeeding care, especially because this time would not be reimbursed (Q3, MD; Q4, MD). HPs in the hospital setting also discussed a lack of time to address breastfeeding, including during hospital rounds. The nursing staff also felt a time crunch in inpatient care (Q5, RN).
CNM, certified nurse midwife; LC, lactation consultant; MD, medical doctor; NP, nurse practitioner; OB, obstetrics; Q, quotation; RN, registered nurse.
Some HPs believed that the timing of their interactions was not right to provide breastfeeding information because there were either more important things to be addressed or other barriers existed. For example, prenatal care providers believed that focus on the pregnancy and delivery took priority over breastfeeding (Q2, MD). On the other hand, hospital-based nurses and LCs discussed the mothers' “postpartum fog” and exhaustion as barriers to providing adequate information and assistance (Q6, RN). Furthermore, it was perceived that women's breastfeeding decisions were better addressed before hospital admission (Q7, LC).
Lack of skills or not their role
HPs also relied on others because they perceived they lacked the right skills or because they did not consider it part of their role (Table 3). With the exception of LCs, HPs endorsed a general sense of breastfeeding as either a shared responsibility by all HPs (Q1, MD) or as someone else's responsibility (Q2, MD). Pediatric providers generally perceived breastfeeding care as their role but varied in their perceived skills.
Hospital nurses usually believed that helping with breastfeeding was part of their role, but they also perceived varying abilities to do so. Some nurses perceived themselves as the “first line” to help with breastfeeding, and if they ran into challenges they would call in LCs for assistance. Other nurses felt less confident in their ability to provide help and perceived their role was to guide new mothers to know what questions to ask the LCs (Q3, RN).
Inconsistent messages
The lack of continuity in care across time and across disciplines could relate to inconsistencies in breastfeeding messages (Table 4). There was awareness of how different opinions about and approaches to breastfeeding care could be confusing to patients and detrimental to their success with breastfeeding (Q1, LC), as well as to patient–HP relationships (Q2, MD). One example of inconsistencies was that some HPs believed it was better for the mother to send her baby to the nursery (Q3, MD), whereas others encouraged rooming-in (Q4, LC). Inconsistent messages were also possible from a single HP. The most salient instances of this were about the balance of encouraging breastfeeding while “not setting them up” to feel guilty if mothers ceased breastfeeding (Q5, MD; Q6, LC).
CNM, certified nurse midwife; LC, lactation consultant; MD, medical doctor; OB-GYN, obstetrician-gynecologist; Q, quotation.
Potential strategies to improve continuity
There was general agreement that HPs needed to provide more education and preparation prenatally for women to breastfeed (Table 4). Prenatal care providers said “it doesn't come up as often as it should.” Some stated that they asked about plans to breastfeed in the first trimester but then did not bring it up again either until the third trimester or in the hospital (Q1, CNM). Nurses and LCs also stated that women needed to be better prepared for breastfeeding before hospital admission and suggested more prenatal teaching through lactation consults, breastfeeding classes, or prenatal La Leche League meetings.
Better follow-up postpartum was also discussed as being necessary. HPs suggested that home visits or postpartum phone calls would help bridge gaps (Q2, LC). Many of the LCs already provided postpartum phone calls to women and believed that this was helpful. Home visits were perceived by some, including the one home-visiting nurse who participated, as a better solution than phone calls alone. Barriers to more women receiving home visits, however, included cost and the perception that many home-visit nurses are not well trained in providing breastfeeding assistance (Q3, MD). Additionally, it was suggested that pediatric care providers also needed more training in breastfeeding support to avoid providing information and advice that was counterproductive (Q4, LC).
Discussion
Discontinuity of breastfeeding care emerged in this study as an overarching barrier for providing adequate breastfeeding care within the healthcare system in central New York. Given that most HPs relied on other HPs to provide breastfeeding care, the concern truly may be “who is the captain of the ship?” Breastfeeding care was largely presented as disjointed with gaps in care and discontinuity between providers and specialties across time. Postnatal gaps in care may be at the root of some aspects of discontinuous breastfeeding care. The current system provides frequent maternal care prenatally, but less so to the new dyad postnatally when breastfeeding support may be essential. Our study confirmed and built on the findings of Martin et al. 8 that the postpartum gap in care is problematic and that few HPs are providing care or know what care is provided during this time. Also consistent with prior research, 9 there was general consensus among our participants that better prenatal breastfeeding care is needed to prepare women before labor and delivery.
It is clear that the most effective breastfeeding support interventions include components of care coordinated across the continuum. 15 Ideally, women should have a consistent HP with whom a trusting patient–provider relationship develops during pregnancy and continues postnatally for provision of breastfeeding support, but this is atypical in the Central New York healthcare system. Obstetricians and midwives have the opportunity to develop such relationships, but these end abruptly after delivery. Meanwhile, pediatricians could provide key support for the breastfeeding infant after discharge, but they often have no previously established relationship with the mothers and thus have not established trust. Family physicians who provide both prenatal and pediatric care may be a better model but are not suited to every situation, particularly with increasing numbers of high-risk pregnancies and deliveries. 16 Moreover, the proportion who provide such care has declined substantially, with only 6% of prenatal care being provided by family physicians in the U.S. 17
Although U.S. healthcare typically separates care for the dyad, other countries have models in which continuity is more likely. For example, in Canada, 42% and 55% of family physicians provide prenatal and well-child care, respectively. 18 In fact, in a recent study Canadian family physicians were more likely to observe the dyad breastfeeding than were pediatricians, a finding postulated to be a result of their stronger relationships with the mothers. 19 However, fewer than half of these physicians believed it was their responsibility to evaluate breastfeeding. 19 As increasing patient- and family-centered care becomes a major focus, breastfeeding represents an important opportunity to develop systems that provide continuity across pre- and postnatal healthcare to support the mother–infant dyad.
Interdisciplinary clinics implemented at Kaiser Permanente, which are staffed by obstetrics, pediatrics, neonatology, lactation services, and other ancillary services for the dyad postdischarge, are one example of efforts to improve continuity. Although data have not been published, internal reports showed that these clinics resulted in improved breastfeeding outcomes and cost savings (C.L. Wade, MD, personal communication, January 2015).
Our study confirmed prior research findings6,7,20 that HPs continue to experience the primary barriers of lack of time and knowledge or skills to manage breastfeeding. Suboptimal training has been well documented in medical and nursing curricula21–23 and textbooks.24–26 Importantly, we identified that this lack of time and skills was present across disciplines, with the exception of LCs who reported adequate skills but inadequate time. These barriers are problematic to patients if omission of breastfeeding conversations conveys that breastfeeding is not important and if the information and assistance provided are inconsistent or incorrect. It has been reported that despite pediatricians' improved confidence levels in providing breastfeeding care, many defer breastfeeding questions to other HPs whose knowledge and training are unknown, possibly because of time constraints.7,27 Although HPs generally believe they are supportive of breastfeeding, relying solely on other HPs to provide breastfeeding care may be insufficient.
Targeting training during residency with a single curriculum has been shown to improve knowledge, breastfeeding management practices, and confidence in providing breastfeeding support among pediatricians, obstetricians/gynecologists, and family medicine physicians. 23 Use of this curriculum was also associated with an increase in institutional exclusive breastfeeding rates. 23 Implementation of such a program has the potential not only to improve knowledge and care provided by each physician, but also to improve continuity of care through exposure of different medical specialties to the same training curriculum. Future research should explore the effect of a single curriculum on continuity in messages and the effect of improved knowledge on reliance on other HPs to provide breastfeeding care. This, in turn, may disentangle the effects on breastfeeding outcomes of insufficient training versus insufficient time, which could inform future needs and strategies to address the barrier of insufficient time.
Expanding lactation services to improve the quality and continuity of breastfeeding care is also now a feasible option as coverage of lactation services is mandated under the Affordable Care Act. 28 This legislation mandates coverage of services “during pregnancy and/or in the postpartum period.” There is evidence that provision of such services across the continuum would be of greatest benefit. 15 Expanding lactation services with Internationally Board Certified Lactation Consultants to provide breastfeeding care for all women through home visits and consultations in clinical settings has the potential to streamline breastfeeding care through the identification of an HP as the “captain of the ship” across the continuum. Assigning each woman to a LC, or at least to a specific lactation service, would reduce confusion about who was providing the care and would decrease the inconsistent messages being provided. Research is needed to develop strategies for structures and implementation of such services that would reach the largest population.
All three hospitals at which our participants worked participate in a state-sponsored hospital-based breastfeeding initiative and tout that they are committed to breastfeeding support, yet HPs discussed substantial problems with breastfeeding care in these settings. Thus, even in hospitals that support breastfeeding, discontinuity of care and inconsistent messages exist. The Baby Friendly Hospital Initiative improves continuity of breastfeeding care through training and implementation of policies that support breastfeeding 29 and, if adopted, could remove some hospital-based problems encountered by our participants, such as conflicts regarding rooming-in.
Discontinuity disproportionately affects women in low socioeconomic groups, certain racial and ethnic groups, or those with low social support, all of whom are at higher risk of poorer breastfeeding outcomes.8,30,31 In our study, physicians noted that time providing breastfeeding care may not be reimbursable, which may be an important barrier, particularly for those who care for a high proportion of women of low socioeconomic status and work in busy clinics. Furthermore, one physician reported that he primarily provides breastfeeding care for his private patients. National data show disparities in access to maternity care practices that support breastfeeding that are consistent with our findings. 32 Improving continuity for high-risk women may help to avoid increasing disparities in breastfeeding rates.
This study provided a broad range of perspectives across the continuum of care and included participants from a variety of practice settings (three different hospitals, 11 different outpatient practices, and community-based professionals). By including two regions in Central New York with diverse populations, we obtained a sample that is likely similar to other regions in the United States. Generalizability is not possible with the qualitative research approach, nor is it the goal.
To identify the unique needs of each type of HP to improve breastfeeding care would require a larger number of participants than is used in qualitative studies such as this. We did, however, include an adequate number who provide care in each period of the care continuum to attain data saturation for each period in the continuum.
Conclusions
In this study, we identified discontinuity of breastfeeding care as a major barrier to providing the type of care that could help us attain our national breastfeeding goals. To improve breastfeeding care for mother–infant dyads, the challenges of inadequate training, gaps in care, and reliance on others must be addressed in our system in which no HPs are in charge of breastfeeding across the continuum. Increasing and improving training of HPs will be critical to improve care. Expanding lactation services has the potential to streamline breastfeeding care, and incorporating these services into interdisciplinary prenatal and postpartum clinics is also likely to be effective. Interdisciplinary collaborations are needed to develop and implement strategies to structure improved breastfeeding care services within the healthcare system and to identify and allocate the resources that could improve continuity of breastfeeding care across the prenatal to postnatal continuum.
Footnotes
Acknowledgments
The authors acknowledge Deanna Nardella, BS, for assistance with transcription and coding. C.D.G. was supported by the Ruth L. Kirschstein National Institute of Child Health and Human Development training grant 5 T32 HD007331 to K.M.R., as well as U.S. Department of Agriculture Hatch Grant 399449.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.