
Abstract
Abstract
Background:
Personal breastfeeding behavior of physician mothers is associated with their clinical breastfeeding advocacy, which in turn impacts patients' breastfeeding behavior. Internists can play an important role in breastfeeding advocacy as they usually come in contact with mothers longitudinally.
Objective:
To explore the personal infant-feeding decisions and behavior of physician mothers in internal medicine (IM).
Materials and Methods:
Physicians with current or previous IM training were isolated from our “Breastfeeding Among Physicians” database. The data in the database were gathered from cross-sectional surveys of 130 physician volunteers, mainly affiliated with the Johns Hopkins University School of Medicine (Baltimore, MD) and the University of Florida College of Medicine (Gainesville, FL).
Results:
Seventy-two mothers reported current or previous IM training and had 196 infants. Breastfeeding rates were 96% at birth, 77% at 6 months, and 40% at 12 months. Exclusive breastfeeding rates were 78% at birth, 67% at 3 months, and 30% at 6 months. While maternal goal for breastfeeding duration correlated with duration of both exclusive and any breastfeeding, there was a consistent and appreciable disparity between maternal duration goal and actual breastfeeding duration. The participants reported work-related reasons for early supplementation and breastfeeding cessation.
Conclusions:
We have described for the first time in the literature the personal infant-feeding intentions and behavior of a cohort of IM physician mothers. Workplace interventions to enable internists to maintain breastfeeding after return to work and to achieve their breastfeeding goals might improve the health of these mothers and their infants and positively impact their clinical breastfeeding advocacy.
Introduction
B
While several studies have assessed physician mothers' personal breastfeeding behavior, to our knowledge, none have evaluated internists specifically or captured a large cohort of internal medicine specialties. Internists can play an important role in breastfeeding advocacy. The U.S. Preventive Services Task Force recommends interventions by primary care providers during pregnancy and after birth to promote and support breastfeeding. 10 As primary care providers, internists are in a unique position to impact women's decision to breastfeed even before conception as they often have a long-term relationship with their patients, which includes providing preconception counseling. Mothers' intention to breastfeed before delivery is a strong predictor of subsequent breastfeeding behavior. 11 Internists can also encourage breastfeeding continuation postpartum as many mothers encounter breastfeeding obstacles after return to work and long after they have been released from obstetrical care.
Given the lack of data specific to internists and increasing number of female internists, 12 we sought to explore the infant-feeding intentions and behavior of physician mothers, in training or practicing, in internal medicine or one of its subspecialties (collectively referred to as IM). We hypothesized that IM physicians would have high breastfeeding initiation rates similar to previous physician studies but higher continuation rates compared to previous physician studies that were done among other specialties.
Materials and Methods
Data for this study were extracted from our “Breastfeeding Among Physicians” database. The data in the database were gathered from two cross-sectional studies of 130 physician volunteers, mainly affiliated with 2 academic institutions (Johns Hopkins University School of Medicine [JHU] and University of Florida College of Medicine [UF]). Criteria for participation were identical for both studies and included being a female physician (doctor of medicine or doctor of osteopathic medicine) and having at least one biological child. Eligible participants were included whether they were in training (e.g., resident or fellow) or had completed training (e.g., faculty at academic site or community practice). Participants were included regardless of their infant-feeding methods (formula, breast milk, or combination). Details of each individual study have previously been reported and will be summarized here.9,13
JHU study
The Institutional Review Board (IRB) at the JHU approved this study. 13 The initial questionnaire was developed in 2008 after review of the instruments used in previous similar studies.14–17 The final instrument contained 49 items, with questions about demographic information and previous breastfeeding education. Participants were also asked the age of each of their children, infant-feeding intention, whether the infant was breastfed, mother's goal for breastfeeding duration when infant was born, age of infant at the time of first supplementation and at the time of complete weaning from breast milk, and work-related factors and other enablers and obstacles of breastfeeding.
Participants were asked to describe their work environment during each pregnancy as “very supportive,” “somewhat supportive,” “neutral,” “somewhat unsupportive,” or “very unsupportive.” They were asked to scale their emotional state during each breastfeeding period as “no,” “mild,” or “severe depression.” Energy level during breastfeeding was rated as “seldom,” “sometimes,” “often,” or “always tired.” To assess availability of time and an appropriate place for milk expression at work, participants chose between “never,” “occasionally,” “sometimes,” “often,” and “always.” Participants were also asked to rate the support they had received in general for their breastfeeding efforts while working from their colleagues, attending physicians if applicable, and program director or chief. Participants rated their satisfaction with their breastfeeding duration as “satisfied,” “somewhat satisfied,” or “not satisfied.”
Recruitment was initiated through an e-mail that contained information about the study and contact information for the principal investigator (PI). This e-mail was sent once to the head of the institution's Women's Task Force as well as residency program directors, with request for dissemination. The PI set up interviews with potential participants as they responded to express interest in the study and conducted 50 eligible interviews (by telephone and in person) between February and August 2009. To maintain privacy of study participants, their names were not entered into the study database.
UF study
The IRB at the UF approved the protocol for this study. 9 Further survey items and response scales were developed in 2009 and incorporated into the JHU questionnaire mainly to assess breastfeeding advocacy of participants. This modified instrument contained 53 items and took approximately 20–30 minutes to complete. The recruitment e-mail was sent once in 2009 to residency and fellowship program directors and once in 2010 to the institution's listserv for house staff and faculty. The PI set up interviews with potential participants as they responded to express interest in the study. Eighty eligible participants were interviewed in person between October 2009 and July 2011 by the PI. To maintain privacy of study participants, their names were not entered into the study database.
Statistical analyses
Data from the two institutional studies were merged using REDCap electronic data capture tools hosted at the UF to generate the “Breastfeeding Among Physicians” database. 18 We abstracted data from physicians who reported current or previous IM training to form the cohort for this analysis. Descriptive statistics were calculated with SPSS software version 16 (SPSS, Chicago, IL). We used the infant as the unit of analysis for calculation of rates because infant-feeding practices of some multiparous participants varied with different offspring.
We used repeated measures methods (Proc Mixed SAS 9.3) for the inferential analysis since many participants had multiple births. Duration of any breastfeeding was the primary dependent variable. Secondarily, we used duration of exclusive breastfeeding and maternal goal for breastfeeding duration. To circumvent censoring, as some participants were still breastfeeding their youngest at the time of the survey, we only included children aged 12+ months in the inferential analysis. One child from a set of twins was excluded to retain within-mother independence. A compound symmetric covariance structure was presumed for the analysis.
Results
Characteristics of mothers and children
Seventy-two participants in the database had reported current or past IM training. Their ages ranged from 27 to 58 years at the time of the study (mean age of 38 years). Nineteen participants (26.4%) were in training at the time of study, and 53 (73.6%) had completed training. Table 1 summarizes additional maternal demographic characteristics. Thirty-one (43%) participants reported current training (residency/fellowship)/practice in general internal medicine, and 41 (57%) reported further subspecialty training (allergy/immunology, cardiology, geriatrics, gastroenterology, hematology–oncology, infectious disease, integrative medicine, nephrology, pulmonary, rheumatology, and vascular fellowship). The 72 mothers had 139 children, ranging from 6 weeks to 27 years of age, at the time of the study. Only 26.4% (n = 19) of IM physicians reported education about breastfeeding during medical school and fewer still during residency (6.9%; n = 5).
Breastfeeding intentions and behavior
Intention to breastfeed was 100% for the IM cohort. The two most frequent reasons cited by participants for breastfeeding intention were infant health (94%) and bonding (58%). In nine pregnancies, the mothers did not report a numerical goal regarding the duration of breastfeeding. In the remaining 130 pregnancies (94%), mothers expressed numerical goals, ranging from 1 to 24 months. In 63.3% of cases (n = 88), mothers planned to breastfeed for 12 months or more.
Of the 139 IM children, 109 were exclusively breastfed at birth (78.4%), 24 received a combination of breast milk and formula (17.3%), and 6 received formula only (4.3%). Regarding infants who did not receive breast milk, mothers reported lack of breast milk in two cases, maternal health reasons in two, and infant health reasons in two. Mothers successfully transitioned two of the six infants who started life with formula only to exclusive breastfeeding and one to a combination of breast milk and formula within the first few weeks postpartum. Of the 24 infants who started life with a combination of breast milk and formula, 10 were successfully transitioned to only breast milk in the first few weeks postpartum.
The mean duration of exclusive breastfeeding for the IM cohort was 3.36 months (standard deviation [SD] 2.27, range 0–9), and the mean duration of any breastfeeding was 9.73 months (SD 6.054, range 0–36). Using the infant as the unit of analysis, breastfeeding initiation rate was 95.7%, and continuation rates were 77.0% at 6 months and 40.3% at 12 months (Fig. 1). Exclusive breastfeeding rates were 78.4% at birth, 66.9% at 3 months, and 30.2% at 6 months. In 124 instances, mothers continued breastfeeding after return to employment. Return to work (n = 13) and/or inadequate milk supply (n = 49) accounted for 89.9% of cases of supplementation before 6 months. Inadequate milk supply (n = 33) and/or insufficient time at work for milk expression (n = 26) accounted for 73.8% of cases of complete breastfeeding cessation before 12 months. Sixteen children were still receiving breast milk at the time of the study.
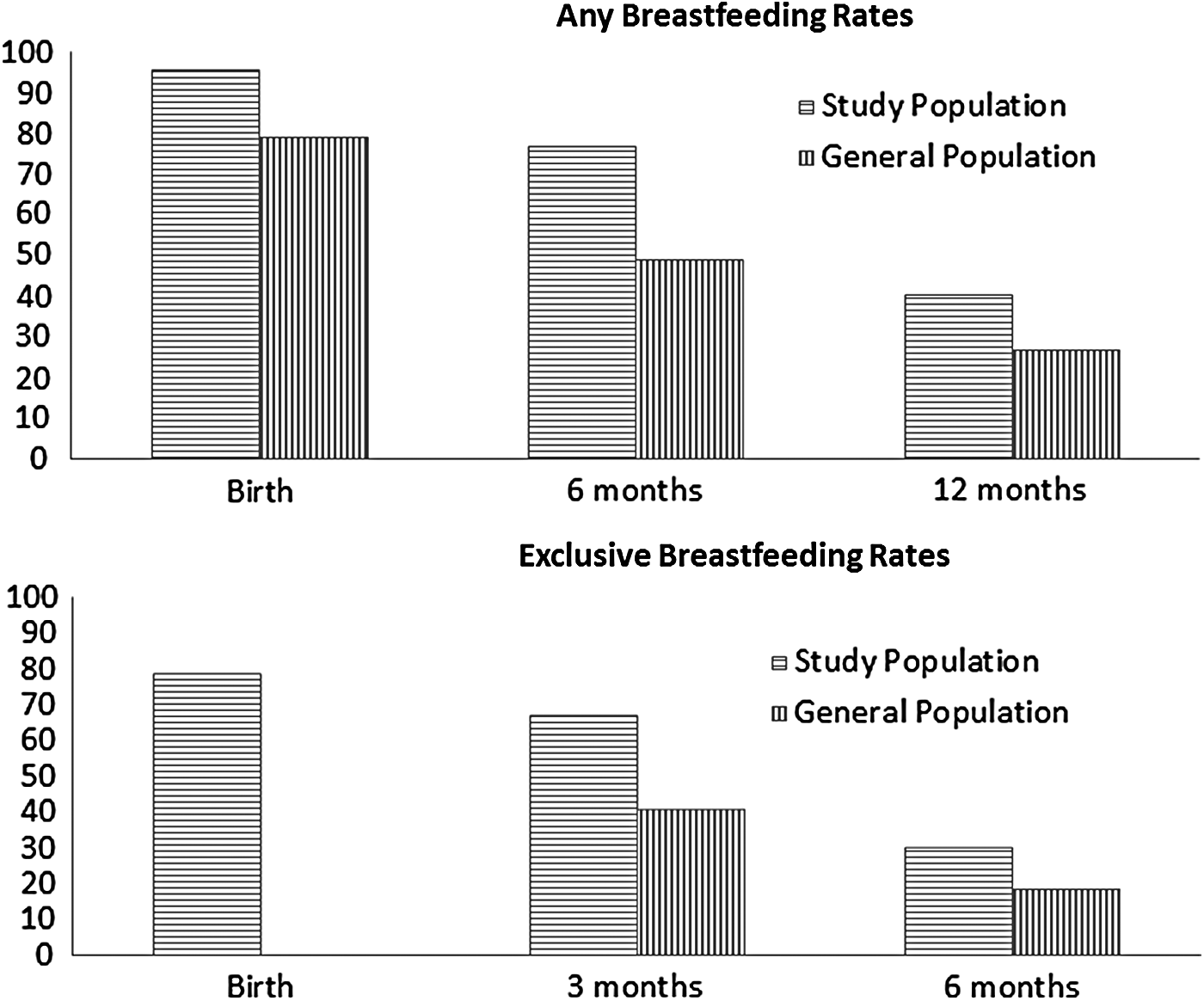
Breastfeeding and exclusive breastfeeding rate of the internal medicine cohort compared to the rates of the general population. 26
Maternal factors
IM mothers reported no postpartum depression in 97 cases (69.8%), mild depression in 35 (25.2%), and severe depression in 7 instances (5.0%). They reported being “seldom tired” in 13 cases (9.4%), “sometimes tired” in 64 (46.0%), “often tired” in 51 (36.7%), and “always tired” in 11 instances (7.9%). Mothers stated that they were satisfied with their actual breastfeeding duration in 86 cases (61.9%), somewhat satisfied in 33 (23.7%), and not satisfied in 20 instances (14.4%).
Work environment
IM mothers worked during 138 of the pregnancies and reported very supportive work environments during 62 pregnancies (44.9%), somewhat supportive environments in 50 (36.2%), neutral work environments in 9 (6.5%), somewhat unsupportive environments in 7 (5.1%), and very unsupportive environments in 10 (7.2%). The average length of maternity leave was 9.97 weeks (SD 8.23), and the average duration of paid leave was 7.97 weeks (SD 6.93). While we did not formally survey the study participants about their institutional family leave policies, many volunteered that they had used sick leave, short-term disability, vacation days, or a combination thereof to arrange for maternity leave. The participants reported returning to work after 138 deliveries and did so on a full-time basis in 113 cases. Participants reported flexibility with their postpartum work schedules in 82 instances (59%), “somewhat” flexible schedules in 11 (8%), and “no” flexibility in 45 cases (33%).
In 117 instances, mothers reported expressing milk while at work. They reported always having time to express milk at work in 23 cases (19.7%), often having time in 33 (28.2%), sometimes having time in 39 (33.3%), occasionally having sufficient time in 18 (15.4%), and never having sufficient time to do so in 4 instances (3.4%). Regarding availability of an appropriate place at work for milk expression, mothers reported always having access in 49 cases (41.9%), often in 31 (26.5%), sometimes in 16 (13.7%), occasionally in 14 (12.0%), and never having access in 7 instances (6.0%). Table 2 summarizes the level of support reported by IM participants for their breastfeeding efforts at work. Several mothers reported that inadequate time at work for milk expression led to insufficient milk supply, which resulted in early supplementation or complete weaning from breast milk. In fact, the two main reasons for supplementation before 6 months cited by participants were return to work and inadequate milk supply, and the two main reasons for complete breastfeeding cessation before 12 months were insufficient time for milk expression and inadequate milk supply.
Inferential analysis
Not surprisingly, maternal goal for breastfeeding duration correlated with duration of both exclusive and any breastfeeding (Tables 3 and 4). Each month of increase in maternal breastfeeding duration goal was associated on average with a 0.88-month increase in actual breastfeeding duration. Duration of any breastfeeding also had a statistically significant association with duration of maternity leave with approximately 5-day increase in breastfeeding for each extra week of maternity leave. However, this correlation did not remain significant after adjustment for maternal breastfeeding duration goal. Another correlation that was almost statistically significant after adjustment for maternal goal was the level of support mothers perceived from their program director or chief for their attempts to continue breastfeeding after return to work. Each unit increase reported in the level of support was associated with approximately 5-week increase in total duration of breastfeeding.
Each month of increase in maternal breastfeeding duration goal was associated on average with a 0.88 month increase in actual breastfeeding duration. Before adjustment for maternal breastfeeding duration goal, duration of any breastfeeding had a statistically significant association with duration of maternity leave, with an approximately 5-day increase in breastfeeding for each extra week of maternity leave. After adjustment for maternal goal, duration of any breastfeeding had an almost statistically significant correlation with the level of support mothers perceived from their program director or chief for their attempts to continue breastfeeding after returning to work, with each unit increase reported in level of support associated with an approximately 5-week increase in total duration of breastfeeding.
BFD, breastfeeding duration; SE, standard error.
Each month of increase in maternal breastfeeding duration goal was associated on average with a 0.29 month increase in exclusive breastfeeding duration.
Discussion
Consistent with other physician studies,14–17,19–22 we found high breastfeeding initiation rates among the 72 physician mothers in the IM cohort. It is encouraging that more than one half of the infants in this study were able to continue receiving breast milk at 6 months of age and that there was a statistically significant correlation between maternal goal for breastfeeding duration and actual breastfeeding duration. However, our data also demonstrated that while 96% of infants were breastfed at birth and intent to breastfeed for at least 12 months was 63%, only 40% of infants continued to receive breast milk at 12 months of age. This discrepancy and the main reasons for complete breastfeeding cessation before 12 months (insufficient time for milk expression and inadequate milk supply) suggest that work-related factors not only influence physician mothers' breastfeeding behavior but also might have a larger impact than their education and intentions on their breastfeeding duration.
It is also concerning that in more than half of the cases, IM mothers reported only having time to express milk at work sometimes, occasionally, or even never. Furthermore, mothers reported that inadequate time at work for milk expression led to insufficient milk supply, which resulted in early supplementation or complete weaning from breast milk. Since sufficiency of time at work for milk expression has a positive correlation with a female physician's breastfeeding duration, 23 scheduling regular breaks and protected time during the workday for milk expression might enable new IM mothers to maintain breastfeeding longer after return to work with minimal burden on colleagues and patient outcomes. Of note, while the Patient Protection and Affordable Care Act of 2010 requires employers with 50 or more employees to provide reasonable break time and a private nonbathroom space for nursing mothers to express breast milk during the workday for up to 1 year postpartum, the current law only applies to nonexempt employees in jobs that are covered by the overtime provisions of the Fair Labor Standards Act and not to exempt (salaried) employees, which usually includes resident, fellow, and practicing physicians. 24
While our sample size might have been too small to detect significant associations between work-related factors and breastfeeding duration, previous studies have identified other modifiable work-related factors associated with breastfeeding duration of physician mothers, including perceived level of support from colleagues, program director for physicians-in-training, and division chiefs for physicians-in-practice. 23 It is encouraging that in the majority of cases (61.8%), IM participants felt that their colleagues were either always or usually supportive of their breastfeeding efforts at work. However, in the remaining cases, the participants reported that their colleagues were oppositional, were neither supportive nor oppositional, or did not even know that they were breastfeeding. It is also concerning that the IM participants reported that in the majority of cases, their immediate superiors (program directors or chiefs) did not know they were breastfeeding (30.5%), were neither oppositional nor supportive (19.5%), or were actually oppositional (2.5%). Educational campaigns to promote workplace awareness that breastfeeding is optimal might effectively increase support level at work as well as breastfeeding duration of physician mothers.
Work-related factors might have also influenced IM mothers' decision to supplement with formula earlier than recommended. The average length of maternity leave in our study was 2.5 months, and the mean duration of exclusive breastfeeding was 3.4 months. The main reasons reported for supplementation before 6 months (return to work and inadequate milk supply) along with supplementation of infants within the first month of mother's return to employment support the impact of work-related factors on physician mothers' exclusive breastfeeding duration. This study also highlights other issues that deserve attention by educators, administrators, and policymakers. For example, the majority of IM physicians reported receiving no breastfeeding education during medical school or training. Unfortunately, mothers reported somewhat or very unsupportive work environments during 12% of pregnancies, only occasional access or never having access to an appropriate place for milk expression at work in 18% of cases, and no flexibility in their postpartum schedules in 33% of cases. It is also noteworthy that these IM mothers reported some degree of depression after 32% of the births, much higher than 13%, which is the average reported prevalence of postpartum depression in the general population. 25
Our study has potential limitations, including recall bias since we collected data on infant-feeding practices reported over a span of nearly 30 years. Our data may also have been skewed by self-selection bias as our participants were volunteers who might not be representative of all IM physicians, thereby limiting the generalizability of our results to all internists. Furthermore, since we relied on institutional listservs and dissemination by program directors and the Women's Task Force, we do not have information available regarding the proportion of respondents compared to physicians who would have been eligible to participate in our study and received the e-mail (e.g., women, parents). We also recognize that infant-feeding practices as well as working environments of physicians have changed over time and that infant-feeding practices in 1980 may not be equivalent to those in 2010. Finally, we did not collect data regarding participants' race/ethnicity. Despite these limitations, our study is the first reported assessment of infant-feeding intentions and behavior among IM physicians (MEDLINE; 1946–May 2012; English language; search terms of “internal medicine,” and “breastfeeding”) and may help provide information to shape medical curriculum as well as policy in relation to internists. Ideally, prospective studies will be conducted that can better characterize the issues for the health of the internists and their children as well as overall health of IM training and practice.
Conclusion
IM physician mothers in this study reported intention to breastfeed as well as awareness of benefits of breastfeeding and current recommendations. Their intentions and knowledge correlated with their breastfeeding practices but did not seem sufficient for achieving their personal breastfeeding duration objectives. Rather, breastfeeding maintenance seemed to be determined by interaction of work-related factors with personal ones, such as intent and knowledge. While our study cohort might have been too small for detection of significant relationships between work-related factors and breastfeeding duration, previous physician studies have identified lack of time and place for breastfeeding/milk expression, lack of collegial or attending support, and inadequate milk supply after return to work as work-related obstacles to breastfeeding maintenance.14–17,19–23
Programs to promote breastfeeding duration, including formal maternity leave policies, part-time employment opportunities, longer paid maternity leave, nonclinical duties when physician mothers first return to work, on-site childcare facilities, protected time for milk expression at work, designated lactation rooms and sanitary storage for breast milk, as well as support and reinforcement at the work-site, especially from colleagues, program directors, and chiefs, are modifiable institutional factors that might influence IM physician mothers' breastfeeding duration after return to work. Effective workplace strategies to promote breastfeeding duration among IM physician mothers returning to work might not only improve the health of the physicians and their children but also enhance their role as breastfeeding advocates and improve breastfeeding rates in the community.
Footnotes
Acknowledgments
This work was partially supported by the NIH grant no. 1UL1TR000064 from the National Center for Advancing Translational Sciences and by the Clinical and Translational Science Institute, NIH grant no. 1UL1RR029890.
Disclosure Statement
No competing financial interests exist.