
Abstract
Abstract
Objective:
The primary aim of this study was to examine the association between postpartum predischarge depot-medroxyprogesterone acetate (ppDMPA) and in-hospital breastfeeding initiation, and the secondary exploratory aim was to determine if any racial disparities are associated with ppDMPA receipt or its relationship to breastfeeding initiation.
Materials and Methods:
We conducted a cross-sectional retrospective chart review of maternal and newborn records at a large urban academic medical center. Variables extracted included in-hospital feeding choice, obstetrical and sociodemographic variables, infant characteristics, and ppDMPA receipt. The association of ppDMPA and maternal–child characteristics with breastfeeding initiation was examined using logistic regression analysis.
Results:
Among singleton live births of 919 mother–infant pairs (76.5% African American [AA]), 67% initiated breastfeeding (34% exclusive and 33% mixed) and 31.4% received ppDMPA. Breastfeeding rates differed significantly between AA (60.7%) and non-AA mothers (86.6%), and ppDMPA also differed significantly between AA (37.6%) and non-AA mothers (11.6%). Adjusting for other independent predictors, mothers who received ppDMPA were 1.5 times more likely not to initiate breastfeeding if AA, and 5.2 times more likely not to initiate breastfeeding if non-AA.
Conclusions:
ppDMPA receipt was independently associated with decreased rates of breastfeeding initiation. Although more AA mothers received ppDMPA than non-AA, the association of ppDMPA with breastfeeding noninitiation was stronger in non-AA than in AA mothers. Future research should examine this question prospectively to ascertain if there is a cause–effect relationship and should address both physiological effects and social perceptions.
Introduction
B
Risk factors associated with reduced likelihood of BF are also associated with higher risk for unintended pregnancy, including AA race, younger age, single marital status, and low income. 7 Formula feeding choice is associated with higher risk of unintended pregnancies and short intervals between pregnancies, both of which are associated with adverse pregnancy outcomes.8,9 Healthy People 2020 objectives aim to reduce the proportion of pregnancies conceived within 18 months postpartum to 29.8%. 10 Thus, the need for effective and acceptable postpartum contraception that is also BF compatible remains critical.
Depot medroxyprogesterone acetate (DMPA) is an effective, long-acting contraception approved for use immediately postpartum, despite theoretical concerns regarding its possible effects on BF initiation and continuation.11–13 Few studies address this issue in populations at risk for both unintended pregnancy and low BF rates.14,15 Brownell et al. showed no significant detrimental effect of postpartum predischarge DMPA (ppDMPA) on BF among low-income women, while Dozier et al. found that women receiving ppDMPA were more likely to be AA and choose formula feeding.14,15 Both studies were survey based, so we planned a chart review to mitigate selection bias. The primary aim of this study is to examine the association between ppDMPA and in-hospital breastfeeding initiation, and the secondary exploratory aim is to determine if any racial disparities are associated with ppDMPA or its relationship to in-hospital breastfeeding initiation.
Materials and Methods
We conducted a retrospective cross-sectional chart review of maternal and newborn records during the period January to June 2012 at a single large academic center. University Hospitals is a tertiary care center and level III regional perinatal center in Cleveland, OH, with ∼3,600 births annually. This review was specifically conducted before start of Baby Friendly designation work at the birthing hospital in September 2012, so that BF support for mothers during the period of chart review was not differentially impacted. All study mothers were admitted to University Hospitals MacDonald Women's Hospital; well newborns remained at MacDonald Women's Hospital and ill newborns or those of gestational age (GA) <35 weeks were transferred to the Neonatal Intensive Care Unit of University Hospitals Rainbow Babies and Children's Hospital. Inclusion criteria for the study included birth of a live singleton infant during the study period, with availability of both maternal and infant records. Exclusion criteria included multiple births; infant did not survive to discharge home, and lack of documentation of feeding outcome. The study was approved by the University Hospitals Case Medical Center Institutional Review Board.
Consecutively available charts were reviewed until the required sample size was met for maternal–infant pairs meeting inclusion criteria. Variables extracted included the following: maternal age, race, marital status, insurance status, weight, height, parity, depression screen, method of delivery, delivery complications, ppDMPA receipt, in-hospital feeding choice, including whether BF was initiated, infant gestational age (with no exclusions), sex, and weight. Prenatal feeding intention asked at time of admission and postdischarge DMPA (contraceptive) intention asked at time of discharge were also collected (prenatal contraceptive intention was not available). At University Hospitals MacDonald Women's Hospital, DMPA is administered on an opt-out basis to all mothers following delivery; therefore, information on ppDMPA receipt was available in each medical record.
The primary outcome of interest was BF initiation. Maternal feeding choice was described as either “BF initiated” (mothers with exclusive BF plus those with mixed feeding [both BF and formula feeding]) or as exclusive formula feeding. The primary variable of interest was maternal receipt of ppDMPA.
Sample size was estimated for our primary objective of detecting an association between ppDMPA and exclusive BF. Based on preliminary data, the in-hospital rates at that time were ∼40% for exclusive BF and 30% for ppDMPA receipt. Since the majority of women do not receive ppDMPA, we assumed the rate of exclusive BF among women not receiving ppDMPA was close to 40% and hypothesized, based on literature review, that the rate would be 10% lower among those receiving ppDMPA. 16 A sample size of 852 achieves 80% power to detect a 10% difference in exclusive BF between the two groups at a 0.05 significance level using the two-sided Z test with pooled variance.
The main analysis included all mother–infant pairs with in-hospital feeding information. Distributions of each feeding choice (exclusive breast milk, mixed feeding, and formula) in both AA and non-AA mothers were described using frequencies and percentages, and the association of BF initiation with ppDMPA was examined using the chi-square test. For those with prenatal feeding intention recorded, agreement between prenatal BF intention and in-hospital BF initiation was examined using the Kappa statistic and the McNemar's test. The relationship between postdischarge DMPA intention and in-hospital BF initiation was examined using the Cochran–Armitage test for trend. Due to the large proportion of missing information on prenatal feeding intention and postdischarge DMPA intention, the primary focus of the analysis was on actual ppDMPA receipt and actual in-hospital feeding choice. All variables included in the analyses described below had 2.4% or less missing values.
Logistic regression with interaction of race and feeding choice was used to determine whether the impact of ppDMPA on in-hospital BF initiation differed between the two race groups (AA and non-AA). Given similar rates of ppDMPA in the exclusive BF and mixed feeding groups for both race groups, BF initiation (which includes both exclusive BF and mixed feeding) was used as the outcome in further analyses. Maternal and infant characteristics between those who initiated BF and those who fed formula only, and between the two race groups, were compared using chi-square and t tests. Since the impact of ppDMPA on feeding choice and multiple demographic factors were different between the two race groups, the formal analysis of ppDMPA impact was stratified by race. In addition, because the sample size was small for the non-AA group, dichotomous variables were used. Continuous variables were categorized to two groups based on quartile levels or established clinical cut points. Age was dichotomized to <30 and ≥30 years based on the top quartile level and similar rates of any BF in three lower quartile groups (62.5–65.0%). The majority of mothers were overweight or obese (median, body mass index [BMI] 32, interquartile range [IQR] 27–37), so the cut point of BMI >35 for obesity class II was used. Gestational age <37 weeks and birthweight <2,500 g were used to identify preterm and low-birthweight infants. Variables in numerical form were also tested in the analyses. Maternal and infant characteristics that potentially associated with noninitiation of BF in univariate analyses were further examined in multivariate analyses for both race groups, and a multivariate stepwise model selection procedure in logistic regression was then used to identify additional factors that independently associated with noninitiation, using p < 0.15 as the entry criterion. The final race-stratified models included 98.4% of AA and 96.3% of non-AA mothers. Therefore, both factors that independently associated with noninitiation, and those known from literature review to associate with noninitiation, were included in final models for both race groups.4,5
Information on length of stay (LOS) for both infant and mother was not reviewed. Delivery mode or gestational age, or complications related to both, could increase LOS and impact BF initiation, so additional analyses were performed to explore BF initiation differences between those who did and did not receive ppDMPA within vaginal and cesarean section deliveries and within gestational age <35 and ≥35 weeks in both race groups using the chi-square test.
Two-sided p values are presented, and p < 0.05 was considered as statistically significant. All analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC).
Results
Records of 974 maternal–infant pairs were reviewed: 953 were live births, 933 of these were singleton births, and the final cohort of 919 live singleton births with in-hospital feeding information was included in the analysis. Maternal mean age was 25.3 (standard deviation [SD] 5.9), 76.5% of mothers identified as AA, 80.5% had public insurance, 77% were unmarried, and 58% were multiparous; 289 mothers (31.4%) received ppDMPA. Infant mean gestational age was 38.7 weeks (SD 2.6), mean birth weight was 3,113 g (SD 266), 471 (51.3%) were female, and 670 (72.9%) were delivered vaginally.
Of all 919 mothers, 614 (67%) initiated BF (34.0% exclusive and 32.8% mixed feeding) and 305 (33.2%) chose exclusive formula feeding. Prenatal BF intention strongly agreed with actual BF initiation among the 687 women (74.7%) for whom prenatal BF intention was recorded (Kappa value 0.75 [95% CI 0.70–0.81]). Among these 687 women, prenatal BF intention (68%) was very similar to BF initiation (67%), and the paired discrepancy was 6% (McNemar's test), demonstrating good agreement between intention and initiation. Actual feeding choice was significantly different between AA and non-AA race groups, with AA mothers less likely than non-AA mothers to choose either exclusive BF (26.2% vs. 59.3%) or any BF (60.7% vs. 86.6%) (Fig. 1).
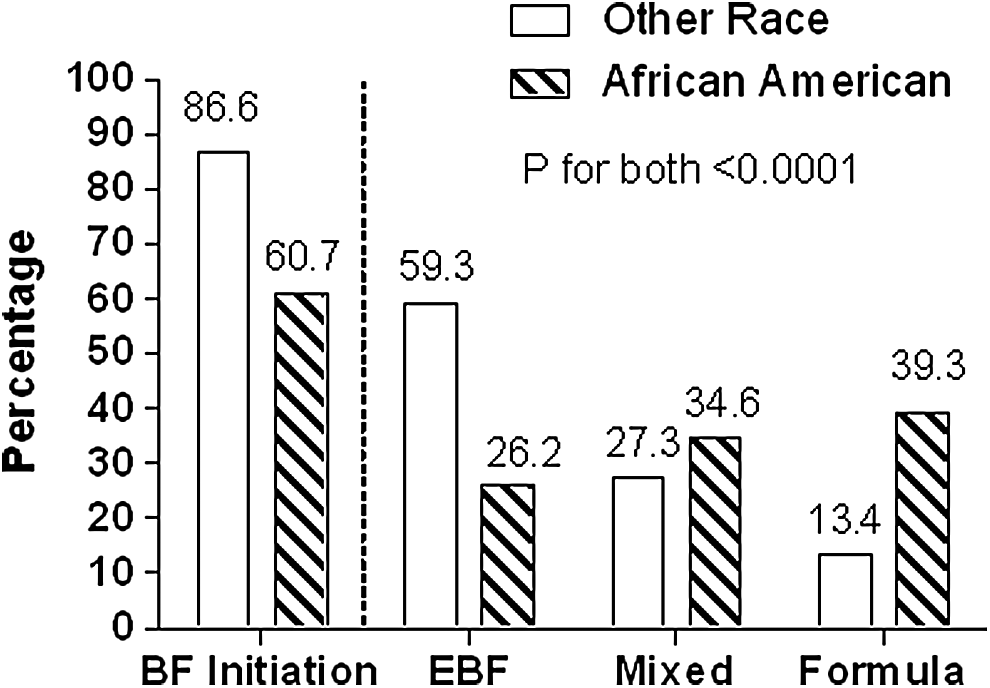
In-hospital feeding choice by race. Distribution of breastfeeding initiation (exclusive breastfeeding or mixed feeding) between African American (patterned bar) and other race mothers (open bar), and distribution of each feeding choice between the two race groups. EBF, exclusive breastfeeding; mixed, combined breast milk and formula feeding; formula, exclusive formula feeding.
The association between ppDMPA and feeding choice is illustrated in Figure 2. Receipt of ppDMPA was significantly higher in AA (37.6%) than non-AA (11.6%) mothers (p < 0.0001). Rates of ppDMPA among mothers who exclusively breastfed and among those who gave both breast milk and formula (mixed feeding) were similar in both race groups (AA [33.2% vs. 32.9%] and non-AA [7.0% vs. 8.8%]). Given that similar rates of ppDMPA receipt were observed in the two groups that initiated BF (exclusive BF and mixed feeding), these two feeding groups were combined as “initiated BF” in further analyses.
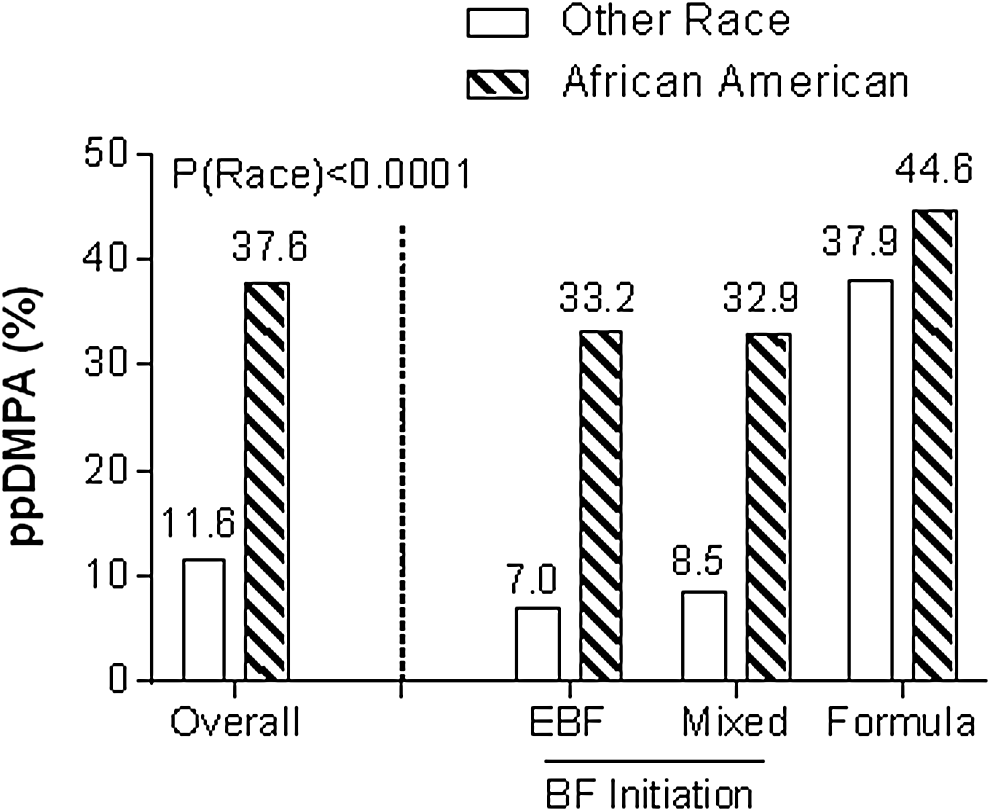
Receipt of ppDMPA (postpartum predischarge depot-medroxyprogesterone acetate) and in-hospital feeding choice by race, comparing rates of ppDMPA receipt between AA (patterned bar) and other race mothers (non-AA, open bar), and rates of ppDMPA receipt in each feeding choice category. EBF, exclusive breastfeeding; mixed, combined breast milk and formula feeding; formula, exclusive formula feeding) between the two race groups. AA, African American; ppDMPA, postpartum predischarge depot-medroxyprogesterone acetate.
Maternal and infant characteristics between mothers choosing formula only compared to initiating BF are presented in Table 1. Both those with ppDMPA receipt and of AA race were less likely to initiate BF. In addition, being multiparous, unmarried, younger, having public insurance, and a vaginal delivery were also potentially associated with feeding formula only. Of note, among the subgroup of 618 mothers (67.2% of all mothers) for whom both ppDMPA receipt and postdischarge DMPA intention were recorded, the rates of BF initiation were 53.6% for mothers who received ppDMPA, 62.2% for those who did not receive ppDMPA but who intended to receive it later (postdischarge contraceptive intention), and 70.6% for those who did not receive ppDMPA and did not intend to receive it at all (p for trend <0.0001).
Descriptor presented by category as used in the multivariate analysis.
Maternal depression as assessed by two-question screening. 25
Maternal obstetrical complications as recorded by the treating physician included gestational diabetes mellitus, T1 or T2 diabetes mellitus, chorioamnionitis, premature rupture of membranes, postpartum hemorrhage requiring transfusion, mild or severe preeclampsia, and prematurity. Maternal complications noted include those associated with breastfeeding initiation or delayed onset of lactogenesis 2 (secretory lactogenesis), and available on record review.
AA, African American; BMI, body mass index; GA, gestational age; ppDMPA, postpartum predischarge depot-medroxyprogesterone acetate; SD, standard deviation.
In addition to the higher rate of ppDMPA receipt among AA compared to non-AA mothers noted above, several maternal characteristics were significantly different between the two race groups. Significantly more AA mothers were unmarried, of younger age, publicly insured, and obese by BMI than non-AA mothers (all p < 0.001; data not shown). The associations between ppDMPA and BF initiation overall and in the two race groups are presented in Figure 3. The overall rates of BF initiation were 72.9% in those not receiving ppDMPA and 53.6% in those who received ppDMPA (p < 0.0001). Figure 3A shows that the association between ppDMPA and BF initiation was stronger in non-AA mothers (90.6% initiated BF among those not receiving ppDMPA vs. 56.0% initiated BF among those receiving ppDMPA) than in AA mothers (65.2% vs. 53.4%, respectively), with p = 0.002 for the interaction between race and ppDMPA. Figure 3B explored whether gestational age at delivery and mode of delivery were associated with differences in BF initiation between those receiving and not receiving ppDMPA in both race groups. The rates of BF initiation in those receiving ppDMPA were significantly lower than in those not receiving ppDMPA within all subgroups (except for GA <35 weeks in non-AA mothers (82% vs. 0%, with small sample size). Since several maternal descriptors, including ppDMPA receipt, as well as the association between ppDMPA and feeding choice, differed between the two race groups, the multivariate analyses were stratified by race.
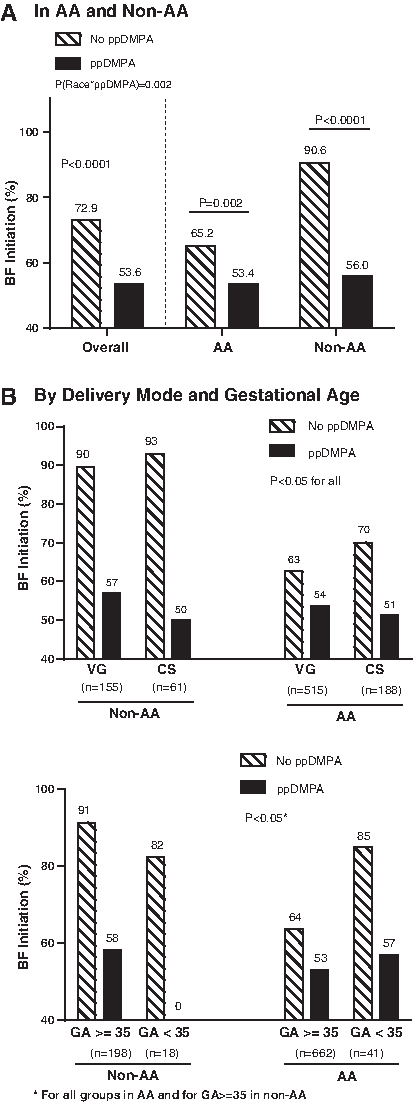
Association between breastfeeding initiation (exclusive breastfeeding and mixed feeding) and ppDMPA by race
The results from multivariate analyses are presented in Table 2. ppDMPA was independently associated with BF noninitiation for both race groups. Other factors independently associated with BF noninitiation included having public insurance for non-AA mothers, and being unmarried and multiparous for AA mothers. Regardless of significance level, factors that were known to associate with BF, including age, marital status, and poverty level (with public insurance serving as a proxy for this variable), were considered in the multivariate analysis for both race groups. Compared to mothers not receiving ppDMPA, the odds ratio for BF noninitiation among those receiving ppDMPA was 5.2 (95% CI 1.7–15.7) for non-AA mothers and 1.5 (95% CI 1.1–2.1) for AA mothers, after adjusting for all other factors included in the final model.
This analysis included 692/703 (98.4%) of AA mothers and 208/216 (96.3%) of non-AA mothers.
Maternal depression as assessed by two-question screening. 25
Maternal obstetrical complications as recorded by the treating physician included gestational diabetes mellitus, T1 or T2 diabetes mellitus, chorioamnionitis, premature rupture of membranes, postpartum hemorrhage requiring transfusion, preeclampsia, and prematurity.
BF, breastfeeding; CI, confidence interval; OR, odds ratio.
Discussion
We found that ppDMPA receipt was associated with failure to initiate BF. In analyses stratified by race, ppDMPA was independently associated with not initiating BF for all mothers. Our findings align with the literature and demonstrate significant racial disparities with respect to DMPA receipt and feeding choice13–16 ; AA mothers were significantly more likely not to initiate BF in-hospital and significantly more likely to receive ppDMPA before discharge. However, we found the negative association between ppDMPA receipt and BF initiation to be stronger among non-AA mothers than among AA mothers. After adjusting for other relevant factors, non-AA mothers receiving ppDMPA were 400% more likely not to initiate BF, and AA mothers receiving ppDMPA were 50% more likely not to initiate BF, compared to those opting out of ppDMPA in the same race group.
The US Selected Practice Recommendations for Contraceptive Use, 2013 (US SPR), from the Centers for Disease Control and Prevention, endorsed by the American College of Obstetricians and Gynecologists, supports administration of DMPA immediately postpartum.11,17 There is controversy regarding this practice due to the inhibitory effects of progesterone on lactogenesis: administration of a progesterone-like hormone could theoretically mimic clinical scenarios in which the usual postpartum drop in progesterone does not occur and copious milk production is inhibited.12,13,18 The WHO guidelines and FDA-approved pharmaceutical inserts recommend DMPA use only beyond 6 weeks postpartum for BF mothers.19,20 Despite conflicting recommendations, however, DMPA is widely used in the immediate postpartum period and is routinely given postpartum predischarge at our institution. Our study shows an association between ppDMPA receipt and BF noninitiation. However, determining whether this association is related to a physiologic impact of ppDMPA on BF initiation, or to other factors such as maternal intent to formula feed, is outside the scope of this study.
Several reports, including ours, have documented demographic differences associated with contraceptive choice, with DMPA recipients more likely to be AA, uninsured, of lower socioeconomic status, of lower educational level, and more likely to have a history of STIs. 21 While we too demonstrated that AA mothers were more likely to receive ppDMPA and more likely not to initiate BF, we found that ppDMPA itself was associated with increased likelihood of not initiating BF independent of race. Moreover, the negative association between ppDMPA receipt and BF initiation was stronger for non-AA mothers than for AA mothers. Although an understanding of any physiological effects of progesterone-only birth control methods is important, it is equally important to consider maternal perceptions of the relationship between postpartum contraception and BF. Little is known about views on the effects of ppDMPA on BF among mothers or how these conceptions might differ by race. Our study may give insight into this relationship.
Strengths of this study include the large number of charts reviewed with in-hospital feeding outcome recorded. In addition, at our institution, ppDMPA is administered as an opt-out postpartum medication, reducing potential confounding by provider preference or medication availability. While all mothers receive contraceptive counseling prenatally and postpartum, and have the opportunity to decline ppDMPA, this “opt-out” approach could create an unintentional treatment disparity because mothers with lower health literacy, which is associated with socioeconomic status and race, may be less likely to decline ppDMPA. Other research has shown that among mothers who received ppDMPA, 72.4% had not planned to receive this contraceptive method in the immediate postpartum period, 16 further complicating understanding of the association with noninitiation of BF documented here. Mothers receive ppDMPA after the initial feeding time or at the time of discharge, but may have made their decision to receive (or not receive) DMPA before the first feeding. Although we had a large amount of missing data regarding DMPA intention after discharge, our data demonstrated a significant difference with regard to BF initiation among mothers who received DMPA in the hospital (53.6%), those who did not receive ppDMPA but intended to receive it later (62.2%), and those who did not want DMPA at all (70.6%).
Our findings indicate that ppDMPA was negatively associated with BF initiation and are consistent with other findings that women who received DMPA either in the hospital or at a later time were more likely planning to formula feed. 15 However, our findings have several limitations. This study is limited by a lack of information on postdischarge feeding practices, and by missing data on prenatal feeding intention and contraceptive intention. The temporal, and more importantly the causal, relationship between a decision to initiate (or not initiate) BF and a decision to receive (or not receive) ppDMPA cannot be determined by this study. We cannot ascertain whether ppDMPA receipt is a risk factor for BF noninitiation, or if noninitiation leads to ppDMPA choice. We included consecutive eligible mother–infant pairs, and stratified the analysis by race, but the smaller (24.5%) proportion of non-AA mothers in our population remains a weakness of the study. In addition, as noted above, University Hospitals MacDonald Womens' Hospital was not designated “Baby Friendly” during the study period, and achieved this designation in 2014. Institutional policy formally endorsed BF during the study period, but individual mothers may have received differing levels of support. LOS was not measured directly, and although it is possible that mothers who stayed longer could have had access to more support and resources, analyses using gestational age and delivery type as proxies for LOS did not suggest any potential impact of LOS on our results. Finally, at the time of this study, predischarge postpartum long acting reversible contraception (LARC) was not available, so mothers' alternative predischarge postpartum contraceptive choices were limited to DMPA, oral contraceptives, and barrier methods.
Given the established benefits of both BF and postpartum contraceptive use, additional data regarding the safety and efficacy of contraception for BF mothers have important public health implications. Mothers must balance the risk of unintended pregnancy with feeding choice. While studies have associated DMPA with lower rates of rapid repeat pregnancy compared to OCP and Patch use, 22 one recent study concluded that ppDMPA administration did not significantly decrease rates of unintended pregnancy within 18 months of delivery. 23 This apparent disconnect between ppDMPA use and effective pregnancy prevention raises concerns for immediate postpartum administration in light of its potential association with BF noninitiation. Further investigation of maternal intentions regarding feeding and birth control method choice is warranted to clarify the association demonstrated by this study between ppDMPA receipt and BF noninitiation. Public health measures should aim to educate mothers about contraceptive options and how they might impact BF and repeat pregnancy. Following this study, our group created a hospital-approved Patient Information Sheet called “BF and Contraception- You have Choices!” as a step in this direction.
Conclusion
Our data provide potential insight into the association between race, feeding choice, and receipt of ppDMPA, and suggest that future research is needed. Little is known about patient perceptions of the relationship between feeding choice and DMPA, and how race, culture, and socioeconomic status might affect these perceptions. Future studies should address both the physiological effects of ppDMPA on BF initiation and the sociocultural views that influence mothers' decisions regarding feeding choice and postpartum contraceptive choice.
Footnotes
Acknowledgments
We gratefully acknowledge the work of Ms. Julie Gartland, who built the study database in REDCap. 24 This work was accepted as a Poster Presentation for the American Academy of Pediatrics National Conference & Exhibition, Washington DC, on October 26, 2015. This material was supported, in part, by the Medicaid Technical Assistance Policy Program (MEDTAPP) through the Ohio Department of Medicaid Healthcare Access Initiative (HCA), Prime Award Number G-1415-07-0060; ODM210409. The MEDTAPP Healthcare Access Initiative supports the development and retention of healthcare practitioners to serve Ohio's Medicaid population using emerging healthcare delivery models and evidence-based practices. Summer Research Fellowships from the Case Western Reserve University School of Medicine supported Dinah Chen and Elena FuellWysong. The Pediatrics Summer Undergraduate Research Program of the Rainbow Babies and Children's Hospital Foundation supported Julie Gartland.
Disclosure Statement
Dr. Perriera is a consultant for Merck & Co. The other authors report no potential conflicts of interest.